Gephyrin: The Synaptic Scaffold That Controls Your Brain's Inhibitory Tone
By Jacob Gordon, INHC, FMT-CThis article contains affiliate links. As an Amazon Associate, MyBioHack earns from qualifying purchases at no extra cost to you. We only link products we research and stand behind.
Gephyrin is a scaffolding protein that determines how well your brain can suppress overactivity, and when it fails, the consequences range from anxiety and seizures to autism and schizophrenia.
In this post, we will discuss what gephyrin is, how it works at inhibitory synapses, what disrupts it, which conditions link to its dysfunction, how to support it nutritionally, relevant genetics, and what to test.
What Is Gephyrin
Gephyrin is a 93 kDa protein encoded by the GPHN gene (chromosome 14q23.3) that serves two entirely separate biological functions. R
Its first function is synaptic: it forms a submembrane scaffold at inhibitory synapses that clusters and anchors GABA-A receptors and glycine receptors in precise postsynaptic densities.
Its second function is metabolic: in the cytoplasm, gephyrin synthesizes molybdenum cofactor (MoCo), which is required by enzymes including sulfite oxidase and xanthine oxidoreductase. R
These two functions are structurally separated within the protein: the G-domain handles MoCo synthesis, while the E-domain mediates receptor clustering. R
Without gephyrin, GABA-A and glycine receptors drift away from synapses and inhibitory transmission collapses. R
What Gephyrin Does
Anchoring Inhibitory Receptors
Gephyrin self-assembles into a hexagonal lattice just beneath the postsynaptic membrane at inhibitory synapses. R
This lattice physically traps GABA-A receptor subunits (primarily those containing β and γ subunits) and glycine receptor β-subunits via direct protein-protein binding. R
The density of gephyrin clustering directly determines inhibitory tone: more clustered receptors means stronger, faster inhibitory postsynaptic currents. R
When gephyrin disperses or is degraded, receptor density at the synapse drops, inhibitory transmission weakens, and the neuron becomes hyperexcitable.
Collybistin and Synaptic Targeting
Gephyrin cannot reach inhibitory synapses on its own in all brain regions: it requires collybistin, a guanine nucleotide exchange factor encoded by ARHGEF9. R
Collybistin activates the small GTPase Cdc42, which reorganizes the local actin cytoskeleton to recruit gephyrin to the correct postsynaptic site. R
Loss-of-function mutations in ARHGEF9 cause gephyrin to mislocalize and produce a syndrome of hyperekplexia, epilepsy, and intellectual disability. R
Excitatory/Inhibitory Balance
Gephyrin is the primary molecular determinant of the excitatory/inhibitory (E/I) balance at the cellular level.
When gephyrin clusters are stable and dense, inhibitory input can match excitatory drive and neurons fire in controlled patterns.
When gephyrin is reduced, even normal excitatory input produces disproportionate neuronal firing, a state seen across neuroinflammation, epilepsy, and anxiety disorders.
What Disrupts Gephyrin
Neuroinflammation
IL-6 and TNF-α both reduce gephyrin cluster size and number at inhibitory synapses. R
This is a direct mechanism linking systemic or central inflammation to reduced inhibitory tone without any change in receptor expression.
The effect is rapid: cytokine exposure can disperse gephyrin clusters within minutes in cell models.
Phosphorylation by Kinases
Gephyrin is a substrate for multiple kinases, and excess phosphorylation drives it away from synapses. R
CDK5 phosphorylates gephyrin at Ser270, reducing cluster size and inhibitory strength. R
GSK3β phosphorylates gephyrin at Ser270 and Ser268, promoting its proteolytic degradation by calpain. R
ERK and CaMKII also phosphorylate gephyrin and shift the balance toward dispersal under conditions of high excitatory activity. R
Palmitoylation (a lipid modification) can stabilize gephyrin at synapses and counteract phosphorylation-driven dispersal. R
Stress Hormones
Corticotropin-releasing factor (CRF) acutely disperses gephyrin clusters in hippocampal neurons. R
This provides a synaptic mechanism for stress-induced anxiety: CRF release reduces inhibitory synaptic strength within minutes, before any change in gene expression.
When the stress system has already lost CRH sensitivity, this dispersal effect can become chronic and self-perpetuating.
See the post on CRH resistance.
Chronic glucocorticoid exposure also downregulates gephyrin expression over longer time scales. R
Withdrawal States
Long-term benzodiazepine use downregulates gephyrin expression as part of tolerance development. R
Alcohol withdrawal sharply reduces gephyrin-dependent inhibitory clustering, contributing to withdrawal seizures and hyperexcitability. R
Toxins and Environmental Factors
Heavy metals including lead and mercury disrupt gephyrin function through kinase activation and oxidative stress at synapses. R
Organophosphate pesticides impair inhibitory synapse formation partly through effects on the gephyrin scaffolding system. R
Conditions Linked To Gephyrin Dysfunction
Autism Spectrum Disorder
Rare de novo microdeletions and point mutations in GPHN are found in individuals with autism. R
These variants cluster in the E-domain and reduce gephyrin's ability to scaffold GABA-A receptors, directly reducing inhibitory tone during critical developmental windows. R
The E/I imbalance that results is one of the most reproducible neurobiological findings in autism genetics.
Epilepsy
Point mutations in GPHN cause epileptic encephalopathy, including forms that overlap with Dravet syndrome phenotypically. R
These mutations reduce gephyrin's self-oligomerization, producing sparse inhibitory synapses and a cortex that cannot suppress seizure propagation. R
Schizophrenia
Postmortem studies show reduced gephyrin immunoreactivity in prefrontal cortex of schizophrenia cases. R
Reduced GABAergic inhibition in prefrontal circuits is one of the most replicated biological findings in schizophrenia, and gephyrin loss is a plausible upstream mechanism.
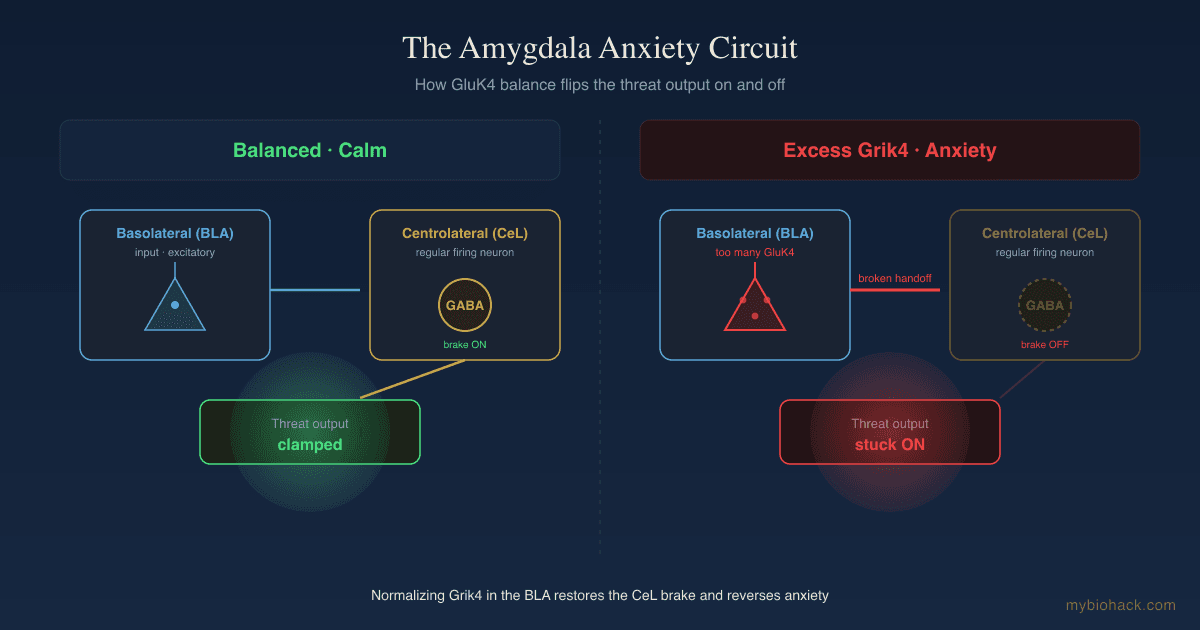
Anxiety and PTSD
CRF-mediated gephyrin dispersal in the hippocampus and amygdala provides a mechanistic link between trauma, stress, and sustained anxiety states. R
Reduced inhibitory tone in the basolateral amygdala, where gephyrin cluster density is high under baseline conditions, is associated with fear generalization and PTSD-like phenotypes in animal models. R
Hyperekplexia
Hyperekplexia (startle disease) results from loss-of-function mutations in glycine receptor subunits or in collybistin, the gephyrin trafficking partner. R
Without proper gephyrin scaffolding, glycine receptors fail to cluster at spinal inhibitory synapses, and the normal startle response becomes pathologically exaggerated.
Depression
Emerging evidence links reduced gephyrin expression in limbic circuits to anhedonia and treatment-resistant depression, possibly through impaired serotonergic modulation of inhibitory circuits. R
There is a big MAYBE here: the evidence is mostly postmortem and animal data, not yet replicated in human clinical studies.
How To Support Gephyrin Clustering
None of these are approved treatments for any gephyrin-related condition.
Work with a clinician before adding any of the below to a treatment regimen.
Magnesium
Magnesium is required for the activity of phosphatases that reverse pathological gephyrin phosphorylation. R
Magnesium also directly modulates NMDA receptor activity, reducing the excitatory kinase cascade (CDK5, ERK) that drives gephyrin dispersal.
Magnesium Glycinate combines two gephyrin-relevant compounds: magnesium and glycine, the primary ligand for glycine receptors that gephyrin clusters.
Typical doses studied for neurological support: 200 to 400 mg elemental magnesium daily.
Lithium Orotate
Lithium is a direct inhibitor of GSK3β, the kinase most strongly linked to gephyrin phosphorylation and degradation. R
By inhibiting GSK3β, lithium reduces the phosphorylation signal that recruits calpain to cleave gephyrin.
Lithium Orotate at low doses (5 to 15 mg elemental lithium) is available over the counter and differs from the high-dose lithium carbonate used in psychiatry.
Therapeutic monitoring is not required at orotate doses, but anyone with kidney or thyroid conditions should discuss this with a physician first.
Zinc
Zinc modulates inhibitory synapse function and supports GABAergic neurotransmission. R
Zinc deficiency is associated with reduced GABA-A receptor subunit expression and impaired inhibitory synapse formation.
Zinc Bisglycinate at 15 to 30 mg/day is typically sufficient for repletion.
Balance zinc with copper at a roughly 8:1 ratio to avoid copper deficiency.
L-Theanine
L-theanine increases GABA and glycine in the brain while reducing cortisol-mediated stress signaling. R
By dampening CRF release, it may indirectly reduce gephyrin dispersal in stress-sensitive circuits.
L-Theanine at 100 to 200 mg is a low-risk intervention with good tolerability.
Ashwagandha (KSM-66)
Ashwagandha reduces cortisol and CRF signaling, indirectly protecting gephyrin clusters from stress-driven dispersal. R
Withanolides, the active constituents, also have direct GABA-A receptor modulating activity in animal models.
KSM-66 Ashwagandha at 300 to 600 mg/day is the best-studied standardized extract.
Inositol
Inositol supports phosphatidylinositol signaling, which intersects with the collybistin/Cdc42 pathway that recruits gephyrin to synapses. R
It also reduces anxiety and panic at higher doses (12 to 18 g/day) through mechanisms that likely include GABAergic synapse stabilization.
Inositol Powder is the most economical form.
Lemon Balm
Lemon balm (Melissa officinalis) contains rosmarinic acid, which inhibits GABA transaminase (the enzyme that degrades GABA) and increases synaptic GABA. R
Higher synaptic GABA activity maintains gephyrin clustering through receptor occupancy and downstream stabilizing signals.
Lemon Balm Extract standardized to rosmarinic acid at 300 to 600 mg/day.
Valerian
Valerian root contains valerenic acid, which acts as a partial allosteric modulator of GABA-A receptors and supports inhibitory tone. R
It does not substitute for proper gephyrin scaffolding but may compensate partially when clustering is reduced.
Valerian Root Extract at 300 to 600 mg before bed.
What To Stay Away From
- Alcohol (chronic): Downregulates gephyrin expression and produces rebound hyperexcitability on withdrawal. R
- Benzodiazepines (long-term): Tolerance involves gephyrin downregulation; withdrawal produces the same hyperexcitable state as alcohol withdrawal. R
- Chronic stress: Sustained CRF and cortisol disperses gephyrin clusters in hippocampal and amygdalar circuits. R
- Heavy metals: Lead and mercury activate CDK5 and ERK at inhibitory synapses, driving gephyrin phosphorylation and dispersal. R
- Inflammatory diet: Elevates IL-6 and TNF-α, which directly reduce gephyrin cluster density. R
- Organophosphate pesticides: Impair inhibitory synapse formation through gephyrin-dependent mechanisms. R
- Sleep deprivation: Increases CDK5 activity and disrupts synaptic homeostasis at inhibitory contacts. R
Testing
No direct clinical test for gephyrin function exists outside research settings.
The following panels probe the biological systems most relevant to gephyrin stability.
Neuroinflammation and Immune Markers
CBC with Differential screens for immune activation patterns that drive cytokine release.
High-sensitivity CRP and ferritin indicate systemic inflammatory burden, which correlates with central neuroinflammation.
Neurotransmitter Metabolites
Organic Acids Test (OAT) measures urinary metabolites including vanilmandelic acid, homovanillic acid, and 5-HIAA, which reflect monoamine and GABAergic neurotransmitter activity indirectly.
Elevated quinolinic acid (a kynurenine pathway marker on OAT) indicates neuroinflammation severe enough to shift tryptophan metabolism away from serotonin and toward excitotoxic metabolites, a state that stresses inhibitory synapse systems.
Mineral Status
RBC Magnesium (request specifically, as serum magnesium is largely uninformative) reflects intracellular stores relevant to kinase regulation.
Zinc with concurrent copper to assess ratio.
Mechanisms Of Action
Simple
- Gephyrin acts like a molecular anchor that holds GABA and glycine receptors in place at synapses so they can receive inhibitory signals.
- When gephyrin clusters break up, those receptors drift away and the synapse becomes effectively deaf to inhibitory input.
- Stress hormones, inflammation, and excess kinase activity all physically scatter gephyrin within minutes.
- Supporting gephyrin means reducing the signals that scatter it (kinases, CRF, cytokines) and providing the nutritional cofactors (magnesium, zinc) that keep stabilizing pathways active.
Advanced
- Gephyrin trimerizes via its G-domain and dimerizes via its E-domain to form a hexagonal submembrane lattice with nanoscale spacing matched to inhibitory postsynaptic densities. R
- The E-domain binds directly to the large intracellular loops of GlyR-β subunits and GABA-A receptor β/γ subunits through a conserved binding motif. R
- Collybistin (ARHGEF9) contains an SH3 domain that binds gephyrin and a DH/PH domain that activates Cdc42, generating PI(3)P-rich membrane microdomains that anchor the gephyrin lattice. R
- CDK5-mediated phosphorylation at Ser270 reduces gephyrin's self-oligomerization capacity, shrinking cluster size without eliminating clusters entirely. R
- GSK3β phosphorylation at Ser268/Ser270 creates a phosphodegron recognized by calpain, leading to proteolytic degradation of gephyrin. R
- S-palmitoylation at Cys212 and Cys284 anchors gephyrin to the inner leaflet of the plasma membrane, stabilizing clusters against phosphorylation-driven dispersal. R
- CRF activates PKA/PKC cascades that phosphorylate gephyrin and simultaneously increase CDK5 activity through p25 generation, producing a feed-forward dispersal signal during acute stress. R
- Lithium inhibits GSK3β by competing with magnesium at the active site and by promoting Ser9 phosphorylation (the inactivating site), reducing gephyrin turnover. R
- The MoCo synthesis function of gephyrin (G-domain) is independent of synaptic scaffolding but is required for sulfite oxidase activity; MoCo deficiency produces a separate severe neonatal encephalopathy distinct from synaptic gephyrin dysfunction. R
Genetics
GPHN (Chromosome 14q23.3)
GPHN encodes full-length gephyrin (736 amino acids) and undergoes extensive alternative splicing generating over 10 tissue-specific isoforms.
Brain-specific exons (C3, C4, C5) regulate collybistin binding affinity and synaptic targeting efficiency. R
rs7525519
This is the most studied common variant in GPHN, located in an intronic regulatory region.
It has been associated with altered gephyrin expression levels in cortical tissue in several eQTL datasets. R
Minor allele carriers show modest but reproducible differences in anxiety-related traits in population studies. R
Effect size is small: this is a risk modifier, not a deterministic variant.
Rare De Novo Variants in GPHN
Whole-exome sequencing studies have identified de novo mutations in GPHN in autism, epileptic encephalopathy, and schizophrenia cohorts. R
Mutations in the E-domain reduce receptor binding affinity; mutations in the G-domain impair oligomerization. R
Copy number variants at 14q23.3 involving GPHN deletions are enriched in autism and intellectual disability cohorts. R
ARHGEF9 (Xq11.1, Collybistin)
ARHGEF9 encodes collybistin, gephyrin's obligate trafficking partner for targeting to inhibitory synapses in the hippocampus, amygdala, and cortex. R
Loss-of-function mutations in ARHGEF9 cause X-linked hyperekplexia with epilepsy and intellectual disability in males. R
The syndrome is clinically distinct from GPHN mutations because collybistin loss only affects the subset of inhibitory synapses where gephyrin targeting depends on PI(3)P-rich membrane domains, producing a regionally selective reduction in inhibitory tone. R
More Research
- Activity-dependent gephyrin plasticity: Inhibitory synapses undergo homeostatic plasticity that adjusts gephyrin cluster size in response to sustained changes in network activity, a finding with direct relevance to post-viral neurological symptoms where baseline excitatory drive is elevated. R
- Autism severity correlation: The degree of GPHN mutation impact on E-domain receptor binding correlates with autism severity scores in carriers, supporting gephyrin as a functional severity modifier rather than a binary locus. R
- BDNF-gephyrin interaction: BDNF signaling through TrkB modulates gephyrin cluster dynamics, providing a mechanistic link between aerobic exercise (which raises BDNF) and improved GABAergic inhibition. R
- Ketogenic diet and gephyrin: Animal models of ketogenic diet show increased gephyrin expression and inhibitory synapse density in hippocampus, suggesting a dietary mechanism for the diet's anti-seizure effects beyond simply reducing glucose availability. R
- MoCo deficiency phenotype: When both the synaptic and MoCo functions of gephyrin are disrupted (as in complete GPHN knockouts), the resulting phenotype is catastrophic neonatal encephalopathy driven by sulfite toxicity, distinct from the more subtle synaptic phenotypes seen with partial E-domain dysfunction. R
- Neuroligin-collybistin interaction: Neuroligin-2 recruits collybistin and thereby gephyrin to nascent inhibitory contacts, establishing a clear pathway from synaptic specification signals to inhibitory receptor clustering. R
- Propofol and gephyrin: General anesthesia with propofol acutely modifies gephyrin cluster geometry, which may contribute to the prolonged cognitive effects seen in vulnerable populations after surgery. R
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Lion's Mane
1000mg/day
Omega-3 (DHA)
2g/day
Phosphatidylserine
100mg 3x/day