Salicylate Sensitivity: The Overlooked Mast Cell and Prostaglandin Trigger
By Jacob Gordon, INHC, FMT-CThis article contains affiliate links. As an Amazon Associate, MyBioHack earns from qualifying purchases at no extra cost to you. We only link products we research and stand behind.
Salicylate sensitivity is a non-allergic food and chemical intolerance that produces asthma, hives, flushing, and gut symptoms without ever showing up on an allergy test.
In this post, we will discuss what salicylates are, where they hide in supposedly healthy foods, the cyclooxygenase mechanism that drives pseudoallergic reactions, why the condition is so easily confused with histamine intolerance and mast cell activation, and a practical evidence-based way to sort out whether salicylates are actually your problem.

Basics Of Salicylate Sensitivity
Salicylates are a family of plant compounds built around salicylic acid, the same molecule that aspirin is chemically derived from.
Plants make them as a defense chemical against insects, fungi, and disease, which is why they concentrate in the parts of a plant most exposed to stress.
The reaction some people have to them is called Salicylate Intolerance (SI), and it is best understood as a pharmacological intolerance rather than a true allergy. R
This distinction matters, because an allergy involves the immune system producing Immunoglobulin E (IgE) antibodies against a specific protein, and salicylate reactions do not.
Instead the reaction is a pseudoallergy, meaning it produces allergy-like symptoms through a direct chemical effect on inflammatory pathways rather than through antibody recognition. R
Because there is no antibody involved, standard skin-prick and IgE blood testing come back negative, and the person is often told nothing is wrong.
The typical presentations are respiratory (rhinitis, asthma, nasal polyps), cutaneous (urticaria, or hives, and angioedema), and gastrointestinal (cramping, loose stools, reflux). R
Salicylate intolerance is a documented masquerader of multiple adverse drug reactions precisely because the same mechanism is triggered by aspirin, other anti-inflammatory drugs, and dozens of everyday foods. R
What Causes Salicylate Sensitivity
Salicylate sensitivity is not one disease with one cause, and it is better thought of as a threshold problem.
Everyone can metabolize a certain amount of salicylate, and symptoms appear when intake plus impaired clearance push a person over their individual tolerance line.
The main drivers are below (not an exclusive list):
- Detoxification capacity (salicylic acid is cleared mainly by glycine conjugation, a saturable pathway that is easy to overwhelm) R
- Genetic variation in the enzymes that build and break down inflammatory eicosanoids R
- Gut dysbiosis (an altered microbiome raises the background load of amines and inflammatory signaling, lowering the threshold) R
- High dietary intake from unpeeled fruits, vegetables, herbs, and spices R
- Underlying mast cell and prostaglandin dysregulation that removes the normal brakes on the reaction R
The reason two people can eat the same tomato-heavy meal and only one reacts comes down to where each of them sits relative to that threshold.
Fixing the modifiable inputs, especially dysbiosis and glycine-conjugation capacity, is how you move the line rather than just avoiding more foods.
How Salicylates Actually Trigger The Reaction
This is the part that separates salicylate sensitivity from ordinary food intolerance, and it is worth understanding in detail.
Salicylates inhibit an enzyme called cyclooxygenase-1 (COX-1), the same enzyme that aspirin and most NSAIDs block. R
COX-1 normally converts arachidonic acid into prostaglandins, including Prostaglandin E2 (PGE2).
When COX-1 is inhibited, that arachidonic acid does not simply disappear, and it gets shunted down the other available pathway.
That other pathway is the 5-lipoxygenase (5-LOX) route, which converts arachidonic acid into cysteinyl leukotrienes (CysLTs) like LTC4, LTD4, and LTE4. R
Cysteinyl leukotrienes are extremely potent inflammatory mediators that cause bronchoconstriction, vascular leak, mucus, and hives, which is exactly the symptom picture of a salicylate reaction.
There is a second half to the mechanism that most explanations leave out, and it is the more important one.
The PGE2 that COX-1 was producing is not just a pro-inflammatory molecule, and at baseline it acts as a brake on mast cells and eosinophils through the E-prostanoid 2 (EP2) receptor. R
PGE2 signaling through EP2 blocks mast cell degranulation and dampens leukotriene production by phosphorylating 5-LOX and shutting it down. R
So inhibiting COX-1 does two things at once: it removes the PGE2 brake on mast cells, and it redirects the freed-up arachidonic acid straight into leukotriene production. R
The result is disinhibited mast cells firing while the leukotriene pathway is simultaneously flooded with substrate.
This is why salicylate reactions look so much like mast cell reactions, because at the tissue level they are mast cell reactions triggered by a prostaglandin mechanism rather than by an allergen.
Salicylate Sensitivity And Overlapping Conditions
The overlap with other intolerances is the single biggest reason salicylate sensitivity gets misdiagnosed.

Histamine Intolerance
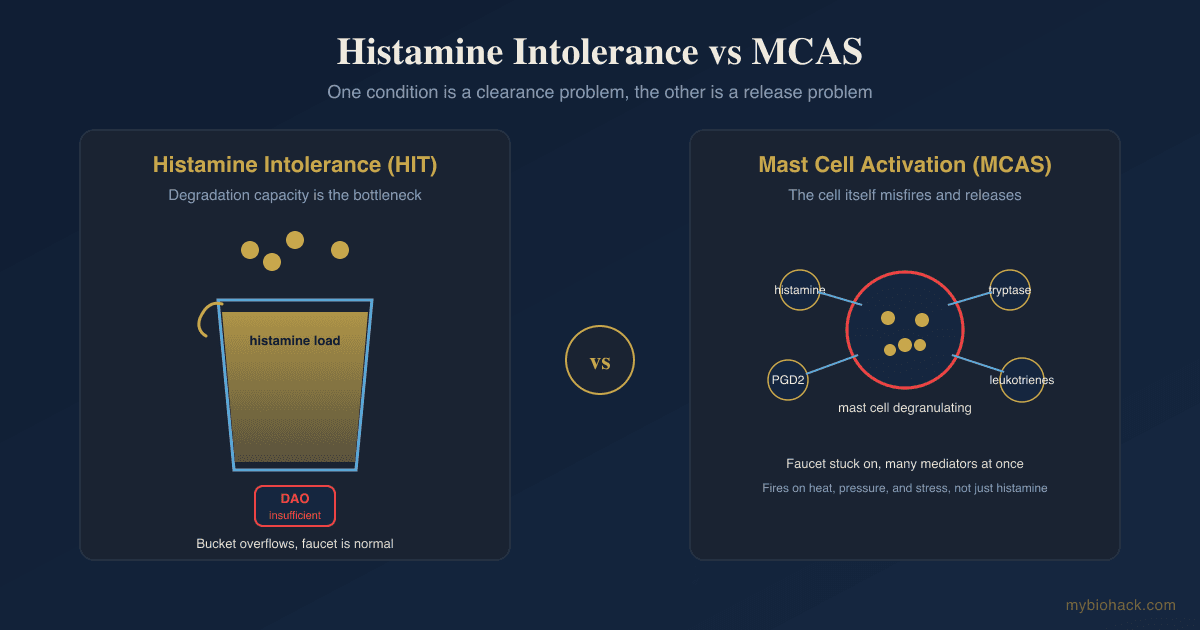
Histamine intolerance is caused by an imbalance between histamine load and the capacity to degrade it, mainly through the enzyme Diamine Oxidase (DAO). R
The symptom lists for the two conditions are nearly identical: flushing, headache, hives, congestion, loose stools, and racing heart.
They also share a striking amount of genetic ground, and the same DAO gene variant that reduces histamine breakdown is specifically associated with cross-reactive hypersensitivity to aspirin and salicylates. R
Many people carry both problems at once, which is why an elimination diet that only removes histamine often gives partial relief.
For the full comparison of the histamine pathways, see how to treat histamine intolerance and mast cells naturally.
Mast Cell Activation Syndrome
Mast Cell Activation Syndrome (MCAS) involves inappropriately triggered mast cells releasing histamine, tryptase, prostaglandins, and leukotrienes.
Salicylates are a well-documented non-immune mast cell trigger, so in someone with an already-twitchy mast cell population a salicylate load can tip them into a full flare. R
The relationship runs both ways, because underlying mast cell disease lowers the salicylate threshold, and salicylates then drive further mast cell activation.
NSAID And Aspirin Hypersensitivity
The clearest proof of the mechanism is NSAID-Exacerbated Respiratory Disease (N-ERD), also called aspirin-exacerbated respiratory disease or Samter's triad. R
In N-ERD, aspirin and other COX-1 inhibitors reliably trigger asthma and nasal symptoms through exactly the leukotriene-shunting pathway described above, and patients show elevated urinary LTE4 as a biomarker of that shunt. R
Dietary salicylate sensitivity sits on the same mechanistic spectrum as this drug hypersensitivity, just driven by food-level rather than drug-level COX-1 inhibition. R
Other Overlaps
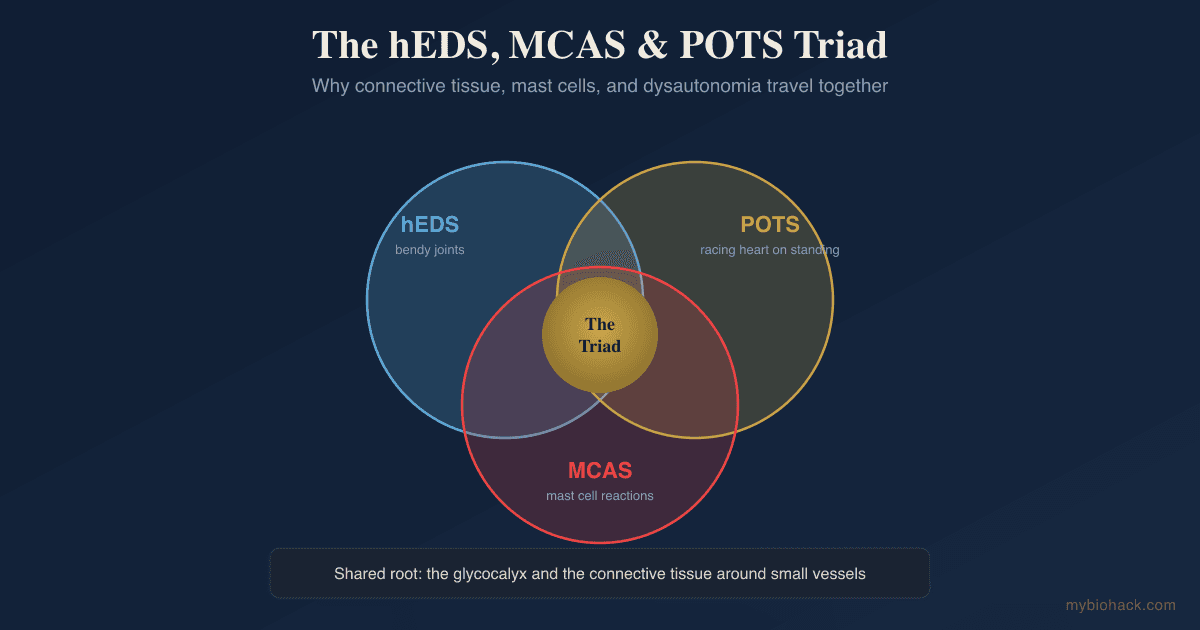
Salicylate sensitivity also clusters with chemical intolerance seen in CIRS and mold illness, with dysautonomia and POTS, and with irritable bowel patterns where dietary salicylates provoke functional gut symptoms. R
Where Salicylates Hide In Healthy Foods
The cruel irony of salicylate sensitivity is that the foods highest in salicylate are the ones marketed as the healthiest.
The foundational data comes from Swain and colleagues, who analyzed 333 foods and found that berries, dried fruits, and many vegetables carry meaningful salicylate loads, while herbs and spices are in a category of their own. R
A more recent Australian analysis by Malakar and colleagues re-measured salicylate in common foods and confirmed the pattern, while adding an important detail about where salicylate concentrates. R
The highest-salicylate categories are below (not an exclusive list):
- Berries and stone fruits (blackberries, raspberries, strawberries, cherries, apricots)
- Dried fruits (raisins, prunes, dates, dried apricots)
- Herbs and spices (curry powder, paprika, thyme, rosemary, cumin, turmeric)
- Nightshade and colored vegetables (tomatoes, peppers, radishes, gherkins)
- Nuts and seeds (almonds, water chestnuts)
- Tea, mint, and many "superfood" extracts
Two practical facts fall out of the analysis.
First, salicylate concentrates in the skin and outer layers, so peeled fruits and vegetables contain far less than unpeeled ones. R
Second, herbs and spices deliver enormous salicylate per gram, so a heavily spiced meal can carry more salicylate than a bowl of berries even though the portion looks small. R
The lowest-salicylate foods tend to be peeled pears, most meats and fish, eggs, and plain grains, which is why a base diet built around them is the standard starting point.

How To Improve Salicylate Sensitivity
The goal is not lifelong deprivation, and it is to lower the load, restore clearance capacity, and stabilize the mast cell and leukotriene machinery so the threshold rises.
1. Run A Structured Elimination And Reintroduction
This is the actual diagnostic test, since no blood test confirms the condition (more on that in Testing).
Drop to a low-salicylate base diet for two to four weeks, track symptoms daily, and then reintroduce one salicylate-containing food at a time to map your personal threshold.
Prospective trials of pseudoallergen-elimination diets report symptom improvement in roughly 28 to 73 percent of chronic urticaria patients, so this step both treats and diagnoses. R
The honest caveat is that when individual foods are re-challenged in blinded fashion, only a minority reproduce symptoms, so some people who feel better on the diet are responding to a broader change rather than salicylate specifically. R
2. Support Glycine Conjugation
Salicylic acid is cleared primarily by conjugation with the amino acid glycine to form salicyluric acid, and this pathway saturates easily. R
Glycine: Supplying extra glycine gives the conjugation pathway more raw material to work with.
Magnesium: A cofactor for the conjugation and broader detoxification enzymes, and magnesium glycinate conveniently pairs it with glycine.
3. Stabilize Mast Cells
Because the reaction runs through mast cells, mast-cell-stabilizing nutrients blunt the downstream response.
Quercetin: A flavonoid that stabilizes mast cell membranes and reduces mediator release.
Vitamin C: Supports histamine degradation and has a mild mast-cell-stabilizing effect (buffered ascorbate is gentler than ascorbic acid).
4. Address The Histamine Overlap
If you carry the common histamine overlap, lowering histamine load in parallel raises the combined threshold.
DAO Enzyme: Supplemental diamine oxidase taken before meals improved symptoms in histamine-intolerant patients in controlled work. R
5. Repair The Gut
A healthier microbiome lowers the background amine and inflammatory load that keeps the threshold low, so correcting dysbiosis is foundational rather than optional.
This is slower work, but it is what lets people eventually reintroduce foods they previously reacted to.
What To Stay Away From
- Aspirin and NSAIDs (they are the drug version of the same COX-1 trigger, see the full COX inhibitor list)
- Concentrated botanical extracts (willow bark, berry concentrates, turmeric and curcumin, peppermint oil)
- High-salicylate spice blends (curry powder, paprika, cayenne, garam masala)
- Mint and menthol products (toothpaste, gum, lozenges, topical rubs)
- Salicylate skincare (methyl salicylate, aspirin masks, many acne and anti-aging products absorb through skin)
- Wintergreen oil (methyl salicylate, one of the most concentrated salicylate sources that exists)
The skin and mucous membrane exposures matter more than people expect, because methyl salicylate is absorbed transdermally and can provoke reactions with no food involved at all.
Testing
There is no single validated blood test that confirms salicylate sensitivity, and the diagnosis is made by structured elimination and reintroduction as described above.
What testing does well is rule out mimics and quantify the overlapping problems that share the threshold.
Blood And Urine Markers
Urinary LTE4 is the research biomarker of the leukotriene shunt, and it is elevated in aspirin and NSAID hypersensitivity, though it is mostly used in specialist and study settings rather than routine care. R
I use the Plasma Histamine test (Quest) alongside the Tryptase test (Quest) to gauge how much of a person's picture is mast-cell and histamine driven, since a persistently elevated tryptase points toward an underlying mast cell disorder rather than pure salicylate intolerance.
Functional Lab Panels
I use the Immune Zoomer (Vibrant Wellness) to assess mast cell markers and systemic immune reactivity when the reactions are severe or systemic.
I use the Gut Zoomer (Vibrant Wellness) to map the dysbiosis and permeability that lower the amine threshold, with the GI-MAP (Diagnostic Solutions) as a PCR-based alternative.
A Food Sensitivity Complete panel (Vibrant Wellness) is worth ordering to exclude genuine IgG and IgE food reactions, but with an important honest caveat: because salicylate intolerance is not antibody-mediated, this panel will not detect it and a clean result does not rule it out. R
Provocation Testing
Supervised aspirin challenge is the gold-standard provocation test used to confirm the drug end of this spectrum in specialist clinics, and it should never be attempted at home given the risk of a severe reaction. R
For the dietary end, the elimination-and-reintroduction protocol is the practical provocation test, ideally logged carefully and reviewed with a practitioner if the picture is complex (contact for personalized guidance).
Mechanisms Of Action
Simple:
- Salicylates block the COX-1 enzyme, which both releases the brake on your mast cells and pushes the raw material into a pathway that makes powerful inflammation chemicals called leukotrienes.
Advanced:
- COX-1 inhibition and eicosanoid diversion Salicylic acid inhibits cyclooxygenase-1, reducing conversion of arachidonic acid to prostaglandins and diverting the substrate pool toward the 5-lipoxygenase pathway, which overproduces cysteinyl leukotrienes (LTC4, LTD4, LTE4) that drive bronchoconstriction, vascular permeability, and urticaria. R
- Loss of the PGE2-EP2 brake Constitutive COX-1-derived PGE2 tonically inhibits mast cells and eosinophils via the EP2 receptor, and EP2 signaling suppresses degranulation while phosphorylating and inactivating 5-lipoxygenase, so COX-1 inhibition simultaneously removes mast cell inhibition and de-represses leukotriene synthesis. R R
- Convergence with histamine clearance Reduced diamine oxidase activity raises circulating histamine, and shared genetic variation in DAO links salicylate cross-hypersensitivity with histamine intolerance, so the two pathways summate at the level of mast-cell-mediated symptoms. R
- Saturable detoxification Salicylate elimination depends on glycine conjugation to salicyluric acid, a capacity-limited pathway, so once conjugation saturates, plasma salicylate and its downstream effects rise disproportionately with additional intake. R
Genetics
ALOX5
ALOX5 encodes 5-lipoxygenase, the enzyme that converts arachidonic acid into leukotrienes.
Variants that increase its activity or expression bias the whole system toward leukotriene overproduction.
Promoter and coding variants in ALOX5 have been associated with aspirin-exacerbated respiratory disease, the drug counterpart of dietary salicylate sensitivity. R
LTC4S
LTC4S encodes leukotriene C4 synthase, the enzyme that makes the cysteinyl leukotrienes responsible for the reaction.
rs730012: the −444A>C promoter variant, whose C allele was identified as a risk factor for aspirin hypersensitivity in some populations, though the association did not replicate consistently across all ethnic groups. R
AOC1 (DAO)
AOC1 encodes diamine oxidase, the primary enzyme that breaks down ingested histamine.
Reduced-function variants impair histamine clearance and lower the shared threshold that salicylate and histamine both push against.
rs10156191: the Thr16Met variant, whose minor allele is associated with both histamine intolerance and crossed hypersensitivity to NSAIDs and aspirin. R
HNMT
HNMT encodes histamine N-methyltransferase, the enzyme that degrades histamine inside cells.
rs11558538: the Thr105Ile variant reduces enzyme activity and is linked to impaired histamine clearance, compounding the overlap with salicylate reactions.
MS4A2
MS4A2 encodes the beta subunit of the high-affinity IgE receptor on mast cells and basophils.
rs573790: a variant associated with aspirin-exacerbated respiratory disease in a candidate-gene replication study, consistent with the mast-cell-centered mechanism. R
More Research
Aspirin desensitization protocols in specialist care show that repeated controlled exposure can raise tolerance in NSAID hypersensitivity, which hints that the dietary threshold may also be partly trainable rather than fixed, though this has not been formally proven for food salicylates. R
Blinded food-challenge data remain the honest weak point of the field, because far fewer patients reproduce symptoms on blinded single-food challenge than improve on an open elimination diet, so there is a big MAYBE around how many self-diagnosed cases are truly salicylate-specific versus responding to a broader dietary change. R
For biomarker testing I use the Plasma Histamine and Tryptase tests to separate mast cell disease from pure intolerance, and the Gut Zoomer to find the dysbiosis that lowers the threshold in the first place.
Intolerance to salicylates and biogenic amines together is more prevalent in atopic dermatitis than in the general population, reinforcing that these pseudoallergic intolerances cluster rather than occur in isolation. R
Peeling produces a large and under-appreciated reduction in salicylate exposure, so for people who react to whole fruits and vegetables, peeling is a low-effort intervention worth testing before eliminating the food entirely. R
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Quercetin
500mg 2x/day
Vitamin D3 + K2
5000 IU + 200mcg/day
DAO Enzyme
1 cap before meals