The Ventromedial Hypothalamus: How A Tiny Brain Region Stores Your Exercise History And Drives Endurance
By Jacob Gordon, INHC, FMT-CThis article contains affiliate links. As an Amazon Associate, MyBioHack earns from qualifying purchases at no extra cost to you. We only link products we research and stand behind.
The ventromedial hypothalamus is a small brain nucleus that controls metabolic rate, glucose handling, fear, aggression, and now appears to store a physical "memory" of past exercise.
In this post, we will discuss what the ventromedial hypothalamus actually does, the new finding that its SF1 neurons encode endurance training, what disrupts VMH function, how to support it, and what this means for fatigue, metabolic disease, and chronic illness.

Basics Of The Ventromedial Hypothalamus
The ventromedial hypothalamus (VMH) is a paired nucleus sitting just above the optic chiasm and lateral to the third ventricle. R
It is one of the densest signal-integrating regions in the mammalian brain.
The VMH has two main subregions with distinct functions, the dorsomedial VMH (VMHdm) and the ventrolateral VMH (VMHvl). R
VMHdm neurons are dominated by steroidogenic factor-1 (SF1, also called NR5A1) expression and drive metabolic and defensive output.
VMHvl neurons express estrogen receptor alpha (ERα) and progesterone receptor and drive social and reproductive behavior. R
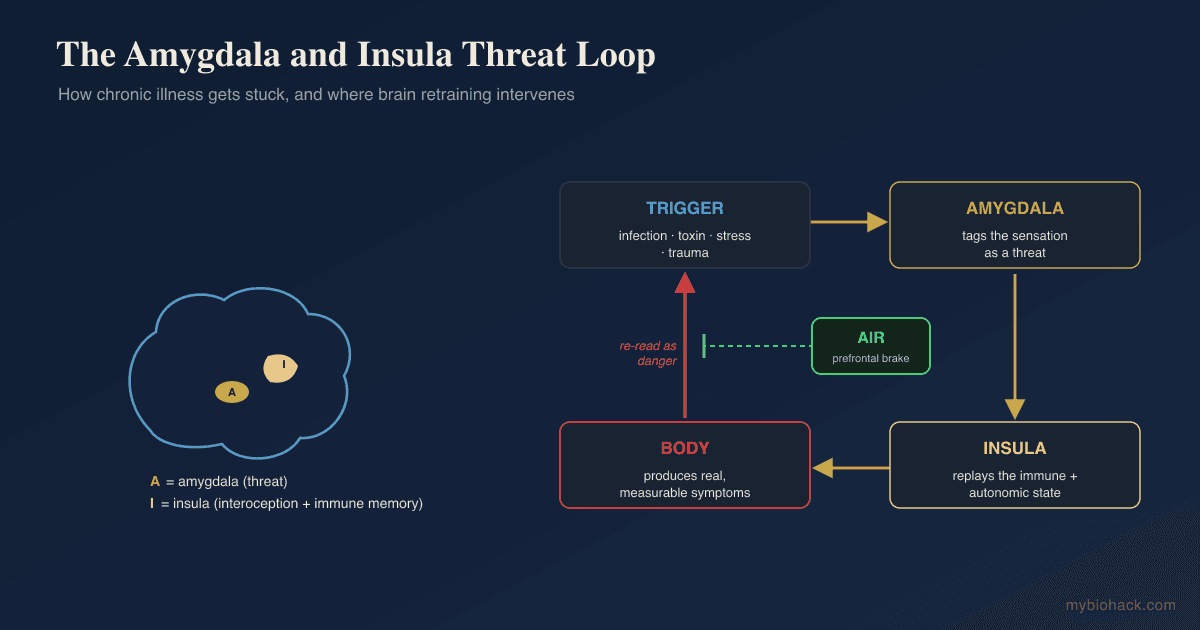
The VMH receives input from the arcuate nucleus (leptin, ghrelin, melanocortin signals), the amygdala (threat input), and brainstem viscerosensory nuclei.
It projects to the paraventricular nucleus (PVN), the periaqueductal gray (PAG), the dorsomedial hypothalamus (DMH), and several brainstem autonomic nuclei. R
The VMH is the only hypothalamic nucleus where SF1 is expressed in adult neurons, which makes SF1-Cre mice the standard tool for selectively manipulating VMH circuits. R
What The VMH Controls
The VMH sits at the intersection of metabolism, autonomic tone, and survival behavior.
Its outputs include:
- Defensive behavior (predator avoidance, freezing, fight-or-flight via VMHdm projections to the PAG) R
- Energy expenditure and brown fat thermogenesis (via SF1 projections to sympathetic preganglionic neurons) R
- Female mating and aggression (via VMHvl ERα neurons) R
- Glucose counterregulation and hypoglycemia sensing (VMH glucose-inhibited and glucose-excited neurons trigger glucagon and epinephrine release) R
- Insulin sensitivity in skeletal muscle and liver (SF1-leptin signaling shapes peripheral glucose disposal) R
- Locomotor activity and endurance (a new finding covered in detail below) R
Lesion studies dating to the 1940s showed that bilateral VMH destruction produces hyperphagia and obesity, which earned it the old label "satiety center."
That label is too narrow.
The VMH is better understood as a metabolic and behavioral gain controller that scales output to perceived energetic and environmental demand.

SF1 Neurons And The Exercise Memory Finding
A 2025 paper in *Neuron* from the Williams lab at UT Southwestern reported that SF1 neurons in the VMH encode a structural and functional memory of exercise training. R
The core findings:
- SF1 neurons are activated by a single bout of treadmill exercise.
- With repeated training over three weeks, post-exercise SF1 activation becomes progressively larger.
- Training increases intrinsic excitability of SF1 neurons (depolarized resting membrane potential, higher spontaneous firing).
- Training roughly doubles the density of excitatory synapses and dendritic spines on SF1 dendrites.
- Chemogenetic inhibition of SF1 neuron output during training blocks the endurance gains.
- Chemogenetic stimulation of SF1 neurons after exercise extends endurance past the normal three-week plateau.
In other words, exercise capacity is not stored only in mitochondria, capillaries, and muscle fiber type.
A significant chunk of it is stored in the brain as VMH plasticity.
This is a feed-forward loop.
Exercise activates SF1 neurons, which undergo synaptic potentiation, which makes the next exercise bout produce a larger SF1 response, which drives larger peripheral adaptation.
Block the loop and the peripheral gains do not happen.
This reframes "exercise intolerance" in chronic illness.
If SF1 neurons are silenced or their plasticity is blocked (by chronic inflammation, hypothalamic gliosis, or hypoperfusion), then training stimulus does not translate into training adaptation no matter how hard the patient tries.
The downstream targets that mediate the endurance phenotype are still being mapped, but VMH SF1 projections to the DMH, PVN, and rostral ventrolateral medulla are the leading candidates because they control sympathetic outflow to skeletal muscle and brown adipose tissue. R
What Disrupts VMH Function
The main causes of VMH dysfunction include: (not exclusive list)
- Chronic neuroinflammation (microglial activation around the VMH from high-fat diet, LPS, or post-viral states degrades SF1 neuron function) R
- Hypothalamic gliosis (visible on MRI as mediobasal hypothalamic signal change in obese humans, tracks insulin resistance) R
- Hypoperfusion (chronic capillary leak and microcirculatory failure from Junction Dysfunction restricts oxygen delivery to a metabolically demanding nucleus)
- Leptin resistance (SF1 neurons require functional leptin signaling for normal output, leptin resistance reduces the VMH metabolic response) R
- LPS and endotoxin exposure (acute LPS reduces SF1 neuron firing and induces sickness behavior with reduced locomotion) R
- Mitochondrial dysfunction in SF1 neurons (SF1-specific knockout of mitochondrial proteins produces obesity and insulin resistance in mice) R
- Persistent stress and glucocorticoid exposure (chronic cortisol remodels VMH dendritic architecture and reduces excitability) R
- Post-viral states (SARS-CoV-2 produces hypothalamic inflammation and microglial activation that overlaps with the VMH region) R
- TCLS-driven capillary rarefaction (loss of capillary density in deep brain nuclei from glycocalyx degradation, see TCLS)
VMH And Overlapping Conditions
VMH dysfunction shows up across a recognizable cluster of conditions.
- Chronic fatigue syndrome / ME/CFS (impaired exercise capacity, blunted sympathetic response on tilt, post-exertional malaise consistent with failure of central training adaptation)
- Hypothalamic obesity (after surgical resection or radiation, classic VMH-pattern hyperphagia and reduced energy expenditure)
- Long COVID (exercise intolerance, blunted heart rate response, dysautonomia, see long COVID and the glycocalyx)
- Metabolic syndrome and type 2 diabetes (mediobasal hypothalamic gliosis precedes peripheral insulin resistance in human imaging studies) R
- Vasoadaptive POTS (orthostatic intolerance with blunted exercise tolerance, see vasoadaptive POTS)
The common thread is a brain that cannot translate effort into adaptation.
How To Support VMH Function
1. Train In Repeating Doses, Even At Low Intensity
The Williams paper makes the case for repeated, frequent exercise exposure over total weekly volume. R
Five short sessions per week produced the SF1 plasticity in mice.
For deconditioned and chronically ill patients, this maps onto recumbent or supine exercise, short interval doses, and avoiding the post-exertional crash that would force long lay-off periods.
The point is to keep stimulating SF1 plasticity at a dose the system can absorb.
2. Reduce Hypothalamic Neuroinflammation
crosses the BBB at relevant concentrations, reduces hypothalamic microglial activation in high-fat-diet models.
DHA accumulates in hypothalamic membranes, reduces saturated-fat-driven microglial activation.
endogenous fatty acid amide that reduces neuroinflammation via PPAR-alpha, with human data in chronic pain and neurodegeneration.
inhibits CD38 and microglial NF-kB activation.
3. Restore Leptin Signaling
SF1 neurons need functional leptin signaling. R
In leptin resistance, the goal is to lower the chronic hyperleptinemia that occupies and desensitizes the receptor.
improves insulin sensitivity and lowers circulating leptin.
Time-restricted eating (8 to 10 hour window):
lowers fasting leptin and restores diurnal leptin rhythm.
Sleep restoration to 7 to 9 hours:
sleep deprivation independently raises leptin resistance markers.
4. Protect The Microcirculation Supplying The Hypothalamus
The hypothalamus is metabolically demanding and relies on intact capillary perfusion.
Glycocalyx restoration is the upstream lever here.
Rhamnan sulfate (mekabu seaweed extract):
restores the endothelial glycocalyx in human trials.
Citrus bioflavonoids (hesperidin, diosmin):
support endothelial function and reduce capillary fragility.
heparan-sulfate-based agent with direct glycocalyx restoration data (prescription in many countries).
See TCLS for the full framework.
5. Support SF1 Neuron Mitochondrial Function
SF1 neurons are unusually mitochondria-dense and their function collapses fast under metabolic stress. R
restores electron transport chain function.
buffers cerebral ATP, with direct effects on cognitive performance in low-energy states.
cofactor for ATP synthesis and stabilizer of NMDA receptor function on SF1 neurons.
raises tissue NAD+ and supports SIRT-mediated mitochondrial biogenesis.
6. Lower Chronic Glucocorticoid Burden
Chronic cortisol remodels VMH dendrites in the wrong direction. R
blunts the cortisol response to physical and mental stress.
Ashwagandha (KSM-66 or Sensoril):
lowers serum cortisol in chronically stressed humans.
shifts EEG toward alpha and reduces sympathetic reactivity.
What To Stay Away From
- Chronic high-saturated-fat diets (drive hypothalamic microglial activation and SF1 dysfunction in animal models) R
- Chronic sleep restriction (independently degrades leptin signaling and hypothalamic glucose sensing)
- High-fructose intake (drives insulin resistance and hypothalamic inflammation)
- Long stretches of total inactivity (lose the SF1 plasticity dose-response, much harder to recover than to maintain)
- LPS-driving gut states (treat dysbiosis and intestinal permeability before expecting central improvements)
- Reflexive use of beta-blockers as the only intervention in POTS (treats the tachycardia, leaves the upstream VMH/TCLS driver in place)
Mechanisms Of Action
Simple:
- The VMH is a small brain region that tells the body how hard to work and how much fuel to burn.
- The SF1 cells in the VMH light up when you exercise.
- If you exercise repeatedly, those cells grow more connections and fire more easily.
- That stored "exercise memory" is what makes the next workout produce real gains.
- If those cells are inflamed, starved, or cut off from blood flow, the gains do not happen even with training.
Advanced:
- SF1/NR5A1 transcriptional program. SF1 is a nuclear receptor required for VMH neuron specification and adult function. Loss-of-function in adult SF1 neurons produces obesity, reduced energy expenditure, and impaired thermogenic response to cold. R
- Leptin-LepRb-STAT3 signaling on SF1 neurons. Leptin acts via LepRb on SF1 neurons to drive STAT3 phosphorylation, which is required for normal peripheral insulin sensitivity in skeletal muscle. SF1-specific deletion of LepRb produces obesity independent of food intake. R
- Glutamatergic plasticity at SF1 dendrites. Repeated exercise increases AMPA-receptor-mediated excitatory drive onto SF1 neurons and increases dendritic spine density, consistent with NMDA-dependent LTP. R
- Intrinsic excitability shift. Exercise training depolarizes the resting membrane potential of SF1 neurons and increases spontaneous action potential frequency, suggesting a change in voltage-gated potassium or HCN channel expression.
- VMH-PAG defense circuit. VMHdm SF1 projections to the dorsolateral PAG mediate predator defense and freezing. The same projection contributes to autonomic activation during high-effort exercise. R
- VMH-DMH-RVLM sympathetic output. SF1 projections drive sympathetic preganglionic neurons in the intermediolateral cell column via DMH and RVLM relays, controlling brown-fat UCP1 expression and skeletal muscle blood flow.
- Hypothalamic gliosis. TLR4-driven microglial activation in the mediobasal hypothalamus from saturated fatty acids (especially palmitate) produces local insulin and leptin resistance, which silences SF1 output. R
- HIF-mediated suppression in TCLS. Hypoperfusion of the VMH from TCLS stabilizes HIF1a in local astrocytes and microglia, which drives VEGF and TGFb1 release, contributing to capillary rarefaction and further metabolic suppression of SF1 firing.
Genetics
- NR5A1 (SF1) loss-of-function mutations in humans cause 46,XY disorders of sex development and adrenal insufficiency, reflecting SF1's role in steroidogenic tissues. Hypothalamic phenotypes in humans are less well characterized due to the systemic phenotype dominating presentation. R
- LEPR (leptin receptor) loss-of-function produces severe early-onset obesity with hyperphagia and reduced sympathetic output, phenocopying SF1 leptin signaling failure.
- MC4R mutations are the most common monogenic obesity cause and interact with VMH output via melanocortin signaling from arcuate POMC neurons.
- TRKB (NTRK2) and BDNF haploinsufficiency produce hyperphagia and obesity. BDNF is expressed in VMH and is required for normal VMH function. R
More Research
The Williams et al. paper does not yet identify which afferent inputs deliver the "exercise has occurred" signal to SF1 neurons.
Leading candidates are circulating myokines (IL-6, irisin, lactate), interoceptive signals from skeletal muscle via the nucleus tractus solitarius, and direct hypothalamic temperature sensing during exercise-induced hyperthermia.
A second open question is whether human VMH plasticity follows the same time course as the three-week mouse data.
Human exercise adaptation studies suggest a 2 to 6 week window for the largest gains in untrained subjects, which is consistent.
The therapeutic frame the authors propose is producing "exercise mimetic" central activation in patients who cannot train (paralysis, severe deconditioning, ICU patients).
That framing applies equally well to ME/CFS and long COVID, where the limit is not motivation but the failure of central training adaptation.
For clinical assessment of hypothalamic involvement in chronic illness, mediobasal hypothalamic gliosis can be seen on standard T2 MRI as increased signal in the mediobasal hypothalamus.
It correlates with peripheral insulin resistance and obesity but is not routinely reported by radiologists.
For biomarker testing I use the Organic Acids Test to assess mitochondrial function and neurotransmitter precursors that affect hypothalamic output, the Total Toxicology Test to identify chemical exposures driving hypothalamic inflammation, and a fasting leptin and HOMA-IR panel to assess upstream leptin and insulin signaling on SF1 neurons.
There is a big MAYBE on whether peripheral interventions (TCLS-targeted, anti-inflammatory, mitochondrial) can fully restore VMH plasticity after years of dysfunction, or whether some plasticity capacity is lost and only partially recoverable.
The Williams paper is in mice trained from baseline health.
The translation to chronically ill humans is the next frontier, and one of the most important targets in chronic fatigue research.
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Lion's Mane
1000mg/day
Omega-3 (DHA)
2g/day
Phosphatidylserine
100mg 3x/day