7 Benefits Of Berberine: AMPK, Blood Sugar, Lipids, And The Honest "Nature's Ozempic" Question
By Jacob Gordon, INHC, FMT-CThis article contains affiliate links. As an Amazon Associate, MyBioHack earns from qualifying purchases at no extra cost to you. We only link products we research and stand behind.
Berberine is a plant alkaloid that activates the same metabolic energy sensor as metformin and delivers meta-analytic blood sugar improvements that rival some oral diabetes drugs, which is why the internet started calling it "nature's Ozempic."
In this post, we will discuss what berberine is, its seven best-supported benefits, where it comes from, how to dose it safely, its mechanisms of action, the genetics that shape your response, and why the "nature's Ozempic" label is mostly wrong.

What Is Berberine
Berberine is a bright yellow isoquinoline alkaloid found in the roots, bark, and rhizomes of several plants used in traditional Chinese and Ayurvedic medicine for centuries.
It has been studied most heavily as a metabolic agent, where its headline action is activation of AMP-Activated Protein Kinase (AMPK), the enzyme that acts as the cell's fuel gauge.
The one fact that shapes everything else about berberine is that it is barely absorbed.
Oral bioavailability in rats is roughly 0.36 percent, because most of an oral dose is destroyed by intestinal first-pass metabolism and heavily extracted into the liver before it ever reaches systemic circulation. R
That poor absorption is not only a limitation.
It means a large share of berberine's benefit happens in the gut itself, where concentrations are high, rather than in the bloodstream, and it explains why the gut microbiome keeps showing up in the mechanism.
The Benefits Of Berberine
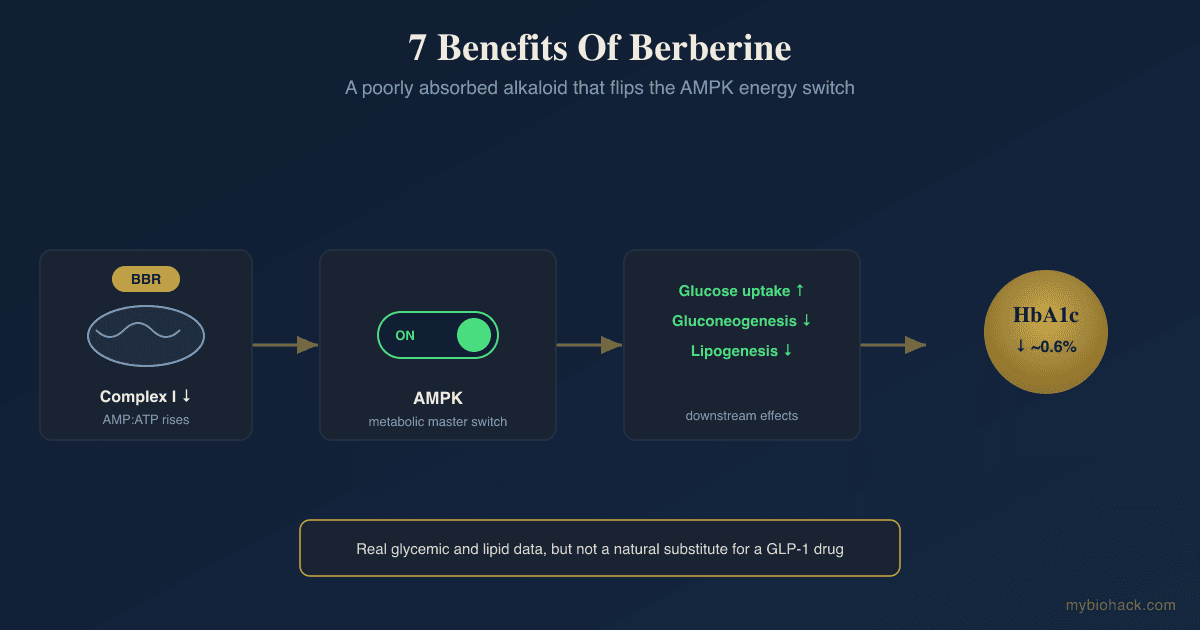
1. It Activates AMPK, The Cell's Metabolic Master Switch
AMPK is the enzyme cells switch on when energy runs low, and turning it on shifts the body toward burning glucose and fat rather than storing them.
Berberine activates AMPK indirectly.
It mildly inhibits Complex I of the mitochondrial respiratory chain, which raises the AMP to ATP ratio, and that rise is the signal that flips AMPK on. R
This is the same upstream mechanism used by metformin, which is why the two compounds are so often compared.
It also puts berberine in the same conversation as other exercise mimetics that work through AMPK and PGC-1alpha, since physical exercise activates AMPK through the exact same energy-stress logic.
There is a big MAYBE worth stating here.
Several cell studies found berberine still drives glucose uptake when AMPK is chemically blocked or silenced, which means AMPK is a major mechanism but probably not the only one. R
2. It Lowers Blood Sugar About As Well As Some Oral Diabetes Drugs
This is berberine's strongest and best-replicated benefit.
In a head-to-head trial in type 2 diabetics, berberine lowered HbA1c by roughly 2 percent and fasting glucose to a degree that was statistically similar to metformin. R
A later meta-analysis of 37 randomized trials in 3,048 patients confirmed the pattern, with berberine reducing fasting plasma glucose by about 0.82 mmol/L and HbA1c by about 0.63 percent versus control. R
The honest framing is that berberine is comparable to some oral hypoglycemics for glycemic control, not superior to them, and the trial quality is generally lower than what a prescription drug goes through.
3. It Lowers LDL And Triglycerides Through A PCSK9 Mechanism
Berberine improves the lipid panel through a route that is genuinely different from statins.
A meta-analysis of randomized trials found berberine reduced total cholesterol by about 0.61 mmol/L, LDL cholesterol by about 0.65 mmol/L, and triglycerides by about 0.50 mmol/L. R
The mechanism is what makes it interesting.
Berberine upregulates the Low-Density Lipoprotein Receptor (LDLR) on liver cells, which pulls more LDL out of the blood, and it does this by suppressing Proprotein Convertase Subtilisin/Kexin Type 9 (PCSK9), the protein that normally degrades that receptor. R R
Statins raise PCSK9 as an unwanted side effect, so berberine's PCSK9-lowering action is mechanistically complementary rather than redundant.
4. It Reshapes The Gut Microbiome
Because so little berberine is absorbed, the gut is where a lot of the action lives.
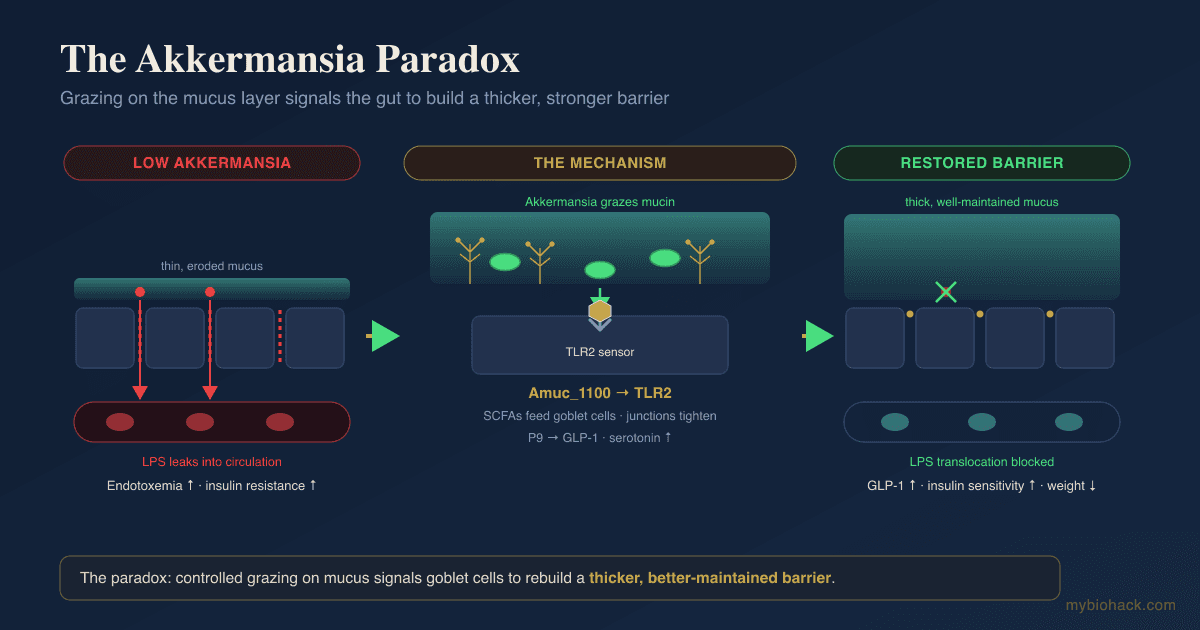
Berberine selectively enriches short-chain fatty acid producers and one bacterium in particular, Akkermansia muciniphila, which is tied to a healthier gut lining and better metabolic markers.
In high-fat-fed rats, berberine restructured the gut community and increased SCFA-producing genera such as Blautia and Allobaculum, alongside a measured rise in fecal short-chain fatty acids. R
In atherosclerosis-prone mice, berberine markedly increased Akkermansia and lowered the metabolic endotoxemia that drives low-grade inflammation. R
This is a plausible mechanism for readers working on dysbiosis, though it is worth being honest that the strongest microbiome data are still from animals.

5. It Reduces Liver Fat
Berberine's combination of glucose lowering, lipid lowering, and gut effects converges on the liver.
In a randomized controlled trial in patients with non-alcoholic fatty liver disease, adding berberine to lifestyle intervention reduced hepatic fat content from 52.7 percent to 36.4 percent and outperformed pioglitazone on body weight and lipid profile. R
That is a meaningful reduction in liver fat for an over-the-counter compound.
6. It Improves Insulin Sensitivity And Metabolic Syndrome Markers
The blood sugar and lipid effects are two faces of the same underlying improvement in insulin resistance.
Across trials berberine improves HOMA-IR, a standard index of insulin resistance, which is the thread connecting its glucose, lipid, and liver-fat benefits. R
For readers with clustered metabolic risk, this is the reason berberine gets used as a broad metabolic lever rather than a single-marker fix.
7. It Produces Modest Weight And Waist Reduction
Berberine does move weight and waist size, but the honest magnitude is small.
A dose-response meta-analysis found berberine reduced BMI by about 0.29 kg/m squared and waist circumference by about 2.75 cm, with no statistically significant change in absolute body weight. R
That is a real effect at the level of body composition and central fat, and it is nowhere near what the injectable drugs do, which is the whole point of the next section.
Is Berberine "Nature's Ozempic"?
The short answer is no.
The label is a marketing frame, and comparing berberine to semaglutide honestly requires holding two facts at once.
Berberine works upstream on cellular energy metabolism through AMPK, glucose handling, and lipid clearance.
The GLP-1 receptor agonists like semaglutide and tirzepatide work through a completely different route, binding GLP-1 receptors in the brain's appetite centers, slowing gastric emptying, and driving large appetite suppression.

The magnitude gap is the honest dealbreaker.
Berberine's meta-analytic weight effect is a fraction of a BMI point and a couple of centimeters of waist. R
Semaglutide at weight-management doses produces roughly 15 percent of total body weight loss over about a year, which is on the order of five to ten times larger.
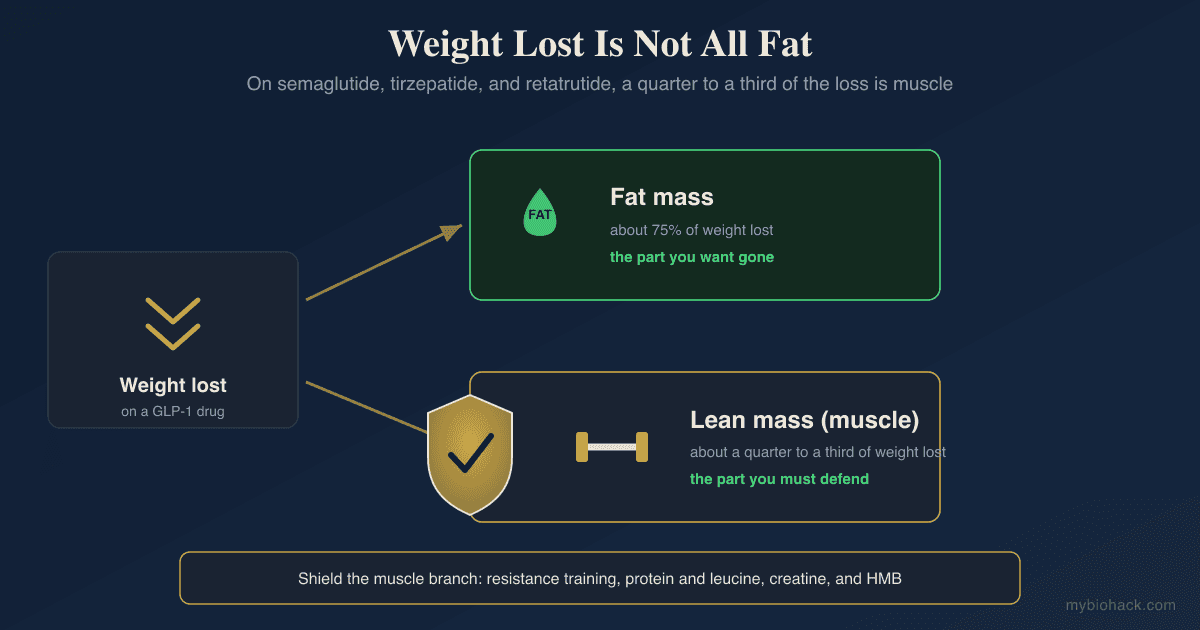
There is also a body-composition caveat that runs the other way.
The GLP-1 drugs cause meaningful muscle loss alongside fat loss, a problem berberine does not share simply because its effect is so much smaller.
The fair conclusion is that berberine is a legitimate metabolic compound with real glycemic and lipid data, and it is not a natural substitute for a GLP-1 drug.
Calling it "nature's Ozempic" oversells the weight effect and misrepresents the mechanism.
Natural Sources
Berberine is not made by a single plant but concentrated in several, most of which are bitter yellow-rooted species used in traditional medicine.
Berberine-containing plants (listed alphabetically):
- Barberry (Berberis vulgaris)
- Chinese goldthread (Coptis chinensis)
- Goldenseal (Hydrastis canadensis)
- Oregon grape (Mahonia aquifolium)
- Phellodendron (Phellodendron amurense)
- Tree turmeric (Berberis aristata)
You cannot reach a therapeutic dose through food.
The amounts studied for blood sugar and lipids come from concentrated extracts standardized to berberine content, which is why this is a supplement conversation rather than a diet one.
Dosage And Safety
Standard Dosing
The dose used in most metabolic trials is 500 mg taken two to three times per day, for a total of 1,000 to 1,500 mg daily, always with meals. R
The split dosing is not optional.
Berberine has a short half-life and poor absorption, so one large dose is both less effective and harder on the gut than divided doses.
Standard Berberine is sold as berberine HCl, and starting at a single 500 mg dose with food for the first week reduces the gut side effects.
Better-Absorbed Forms
Because plain berberine is barely absorbed, two upgrades are worth knowing.
The first is dihydroberberine.
The gut microbiome actually converts a portion of swallowed berberine into dihydroberberine using bacterial nitroreductases, and that reduced form is absorbed roughly five times better before converting back to berberine in tissue. R
Taking Dihydroberberine directly skips that bottleneck, and a human pharmacokinetic study found it reaches higher blood levels than an equivalent oral berberine dose, so effective doses are lower (often 100 to 200 mg). R
The second is pairing berberine with silymarin from milk thistle.
A meta-analysis of five randomized, double-blind, placebo-controlled trials found the Berberine plus silymarin combination improved LDL by about 29 mg/dL, triglycerides by about 28 mg/dL, and fasting glucose by about 7.5 mg/dL, with silymarin thought to improve berberine's absorption. R
Side Effects
Gastrointestinal complaints are by far the most common problem, reported in a meaningful share of trial participants.
Common berberine side effects (not an exclusive list):
- Abdominal cramping
- Constipation
- Diarrhea
- Flatulence and bloating
- Nausea
These usually peak in the first week and ease as the gut adjusts, and starting low with food blunts them. R
Drug Interactions
This is the part most people skip and should not.
Berberine inhibits the drug-metabolizing enzymes CYP3A4, CYP2D6, and CYP2C9, plus the P-glycoprotein transporter, which means it can raise the blood levels of many prescription drugs.
In healthy volunteers, two weeks of berberine at 300 mg three times daily increased exposure to the CYP3A4 probe drug midazolam by about 40 percent. R
Practical caution is warranted with cyclosporine, statins, warfarin, digoxin, and other agents cleared by these pathways, and berberine stacked with prescription glucose-lowering drugs can push blood sugar too low.
Who Should Not Take It
Berberine is contraindicated in pregnancy and breastfeeding.
It crosses the placenta, passes into breast milk, and can displace bilirubin from albumin, which raises the risk of neonatal jaundice and, in severe cases, kernicterus. R
It should also be used with caution in people with glucose-6-phosphate dehydrogenase deficiency, where berberine-containing herbs have been linked to hemolysis in case reports, though the evidence is mixed. R
Mechanisms Of Action
Simple:
- Berberine gently stresses the cell's energy supply, which flips on a master switch (AMPK) that tells the body to burn sugar and fat instead of storing them.
- Most of a berberine dose never gets absorbed, so a lot of its benefit comes from reshaping the bacteria in your gut.
- It helps the liver pull more cholesterol out of the blood by blocking a protein (PCSK9) that would otherwise destroy the liver's cholesterol vacuum cleaners.
Advanced:
- AMPK activation via mitochondrial inhibition Berberine mildly inhibits Complex I of the electron transport chain, lowering ATP production and raising the AMP:ATP and ADP:ATP ratios, which allosterically and covalently activates AMPK (with LKB1 and CaMKKbeta acting as upstream kinases). Activated AMPK increases GLUT4-mediated glucose uptake, suppresses hepatic gluconeogenesis, and inhibits lipogenesis. R
- PCSK9 suppression and LDLR stabilization Berberine downregulates PCSK9 transcription through effects on SREBP2 and HNF1alpha and activates ERK1/2 signaling, while also stabilizing LDLR mRNA post-transcriptionally, and the net result is more LDL receptors on hepatocytes and greater clearance of circulating LDL. R R
- Microbiome remodeling and endotoxemia reduction In the gut lumen, where berberine concentrations are highest, it enriches SCFA-producing taxa and Akkermansia muciniphila while suppressing opportunists, raising luminal short-chain fatty acids and reducing lipopolysaccharide-driven metabolic endotoxemia and the inflammation that follows. R R
- Microbial pro-drug conversion Gut bacterial nitroreductases reduce berberine to dihydroberberine, a form absorbed roughly five-fold better, which then re-oxidizes back to berberine in tissue, making the microbiome part of berberine's own pharmacokinetics. R
Genetics
PCSK9
PCSK9 encodes the protein that berberine suppresses to lower LDL, so variation in this gene shapes both baseline LDL and, plausibly, the room berberine has to work.
Loss-of-function variants lower PCSK9 activity, which keeps more LDL receptors on the liver and lowers circulating LDL.
rs11591147 (R46L) is a loss-of-function variant associated with roughly 15 to 28 percent lower LDL cholesterol and a substantially reduced risk of coronary heart disease. R
UGT1A1
UGT1A1 encodes the sole liver enzyme that conjugates bilirubin so it can be cleared, which matters because berberine displaces bilirubin from albumin.
Reduced-function promoter variants lower enzyme expression and raise circulating bilirubin, the basis of Gilbert's syndrome.
rs887829 (linked to the UGT1A1*28 allele) reduces UGT1A1 expression and raises total bilirubin, so carriers already run a lower conjugation reserve. R
G6PD
G6PD encodes glucose-6-phosphate dehydrogenase, the enzyme that protects red blood cells from oxidative damage.
Deficiency variants leave red cells vulnerable to oxidative stress and hemolysis from certain drugs and compounds.
Berberine-containing herbs have been flagged for caution in G6PD deficiency because of case reports of hemolysis and hyperbilirubinemia, although the controlled evidence is contradictory. R
More Research
- AMPK may not be the whole story, because berberine still drives glucose uptake in cells where AMPK is silenced or blocked, which points to additional insulin-signaling and glycolytic pathways that are not fully mapped. R
- Dihydroberberine has strong human pharmacokinetic data showing better absorption, but long-term outcome trials on hard endpoints like HbA1c are still thin compared with the large berberine literature. R
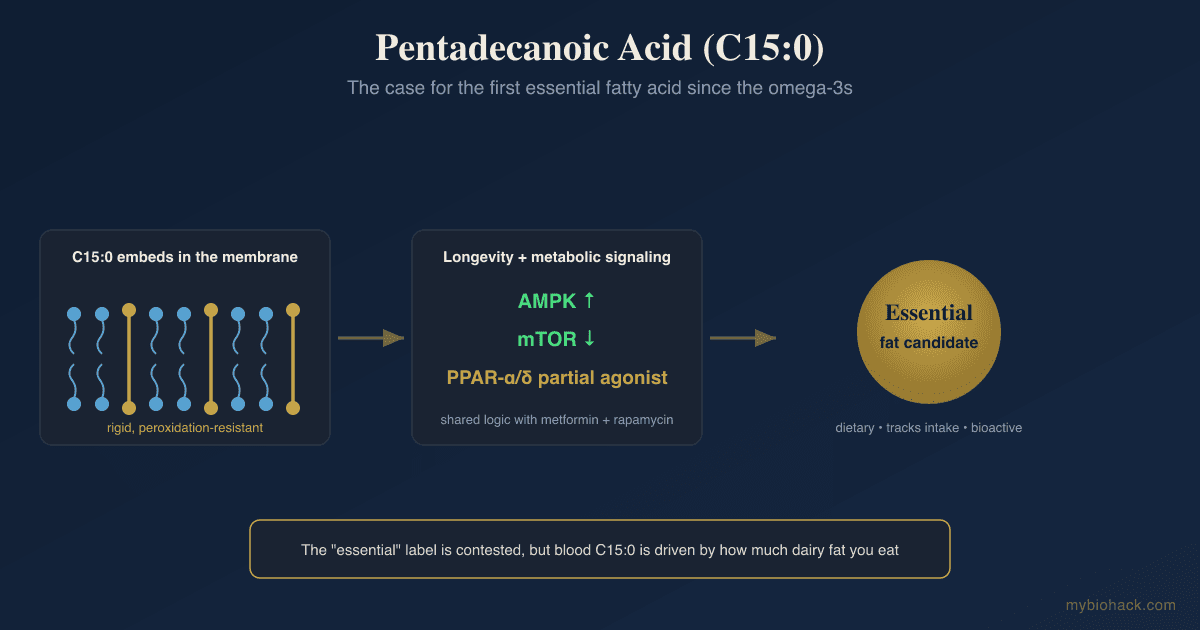
- For readers stacking metabolic support, pentadecanoic acid (C15:0) is a different lever that works on membrane stability and mitochondrial function rather than AMPK, and the two are not redundant.
- The gut-first mechanism means berberine's benefits may depend partly on an individual's starting microbiome, which could explain some of the variability in who responds, and this is an open and active research question. R
- The trial base for berberine is large but generally lower in methodological quality than pharmaceutical trials, so effect sizes should be read as promising rather than definitive.
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Electrolyte Complex
1 scoop/day
CoQ10
200mg/day
Magnesium Glycinate
400mg at bedtime