GLP-1 And The GLP-1 Receptor: How The Hormone Works, What The Drugs Actually Do, And How To Support It Naturally
By Jacob Gordon, INHC, FMT-CThis article contains affiliate links. As an Amazon Associate, MyBioHack earns from qualifying purchases at no extra cost to you. We only link products we research and stand behind.
Glucagon-like peptide-1 (GLP-1) is an incretin hormone produced in the gut and brain that regulates blood glucose, suppresses appetite, slows gastric emptying, and does a remarkable number of things outside the pancreas that most people, including most prescribing physicians, do not fully appreciate.
The pharmaceutical industry has spent the last two decades engineering drugs to exploit GLP-1's receptor with increasing potency and duration.
Those drugs are now reshaping medicine.
But before you can understand why semaglutide and tirzepatide work the way they do, or why natural strategies to support GLP-1 function have real but limited effect, you need to understand what GLP-1 is, what its receptor is and how it signals, and what happens when you activate it continuously versus in short physiological pulses.
This post covers the biology of GLP-1 from synthesis to degradation, the GLP-1 receptor as a class B GPCR in mechanistic detail, the pharmaceutical agonists from exenatide to retatrutide with honest efficacy data, natural strategies to stimulate GLP-1 secretion, clinical applications beyond diabetes, and the side effect profile with particular attention to the areas of genuine uncertainty.
What Is GLP-1 And Where Does It Come From
GLP-1 is a 30 amino acid peptide hormone derived from the post-translational processing of proglucagon. R
The proglucagon gene is expressed in three different tissues, and the same precursor protein gets processed into completely different hormones depending on where it is expressed.
In pancreatic alpha cells, proglucagon is cleaved by prohormone convertase 2 (PC2) to produce glucagon.
In intestinal L-cells and brainstem neurons, proglucagon is cleaved by prohormone convertase 1/3 (PC1/3) to produce GLP-1, GLP-2, glicentin, and oxyntomodulin. R
The initial full-length product GLP-1(1-37) is biologically inactive.
PC1/3 cleavage and C-terminal processing generate two equipotent biologically active forms: GLP-1(7-36) amide (the predominant form, accounting for over 80% of circulating GLP-1 in humans) and GLP-1(7-37). R
The 7 prefix indicates that the first six amino acids of the original sequence have been removed; what remains is a peptide beginning with histidine at position 7 of the proglucagon-derived sequence.
This is not a trivial nomenclature detail: the N-terminal histidine of GLP-1 is essential for receptor activation, and it is precisely this residue that dipeptidyl peptidase-4 (DPP-4) attacks to inactivate the hormone.
L-cells are enteroendocrine cells concentrated in the distal jejunum, ileum, and colon.
They are directly exposed to luminal nutrients and respond to fat, protein, carbohydrate, and bile acids passing through the intestine.
GLP-1 is secreted within minutes of eating and continues for several hours, in a pattern roughly proportional to caloric load and macronutrient composition.
The DPP-4 Problem
DPP-4 is a serine protease expressed on the surface of virtually every endothelial cell in the body, on hepatocytes in high abundance, and in soluble form throughout the circulation.
It cleaves the His-Ala dipeptide from the N-terminus of GLP-1(7-36), generating the inactive metabolite GLP-1(9-36), which has negligible GLP-1R agonist activity. R
Because DPP-4 is expressed directly on endothelial cells lining intestinal capillaries, it begins degrading GLP-1 immediately at the site of secretion, before the hormone even reaches the portal circulation.
Fewer than 25% of secreted GLP-1 escapes the intestinal wall intact.
An additional 40-50% of remaining active GLP-1 is degraded across the liver by DPP-4 on hepatocytes.
The result: only 10-15% of secreted GLP-1 reaches systemic circulation intact, with a plasma half-life of approximately 2 minutes. R
Fasting plasma GLP-1 levels are 0-15 pmol/L.
Peak postprandial levels reach only 15-50 pmol/L.
This extreme brevity of native GLP-1 action is why pharmaceutical agonists needed to be designed with resistance to DPP-4 cleavage built in, and why natural GLP-1 stimulation strategies, while real, cannot replicate the pharmacological concentrations achieved with injectable agonists.
The GLP-1 Receptor: A Class B GPCR
GLP-1R is a class B1 G protein-coupled receptor (GPCR), belonging to the secretin/glucagon subclass that also includes the glucagon receptor (GCGR), the glucose-dependent insulinotropic peptide receptor (GIPR), the glucagon receptor, and the VIP receptor family. R
Understanding what class B means matters.
Class A GPCRs (rhodopsin family, the largest class) primarily bind small molecule ligands that insert into the transmembrane bundle from outside.
Class B GPCRs are peptide-hormone receptors.
They have a large extracellular N-terminal domain (ECD) of approximately 150 amino acids that performs the initial high-affinity binding to the peptide ligand's C-terminal region.
The peptide N-terminus then inserts into the transmembrane helical bundle to trigger receptor activation.
This two-step binding mechanism is called the "two-domain" or "peptide docking" model, and it is why small molecule agonists of class B GPCRs were historically so difficult to develop: they had to compete with a peptide that docks through a two-stage process involving both the large ECD and the transmembrane core.
GLP-1R consists of 463 amino acids with an extracellular N-terminal domain, seven transmembrane helices, three extracellular loops, three intracellular loops, and an intracellular C-terminal tail. R
The ECD contains six conserved cysteine residues that form three disulfide bonds (Cys46-Cys71, Cys62-Cys104, Cys85-Cys126), stabilizing its structure for peptide capture. R
Residues Trp72 and Trp110 in the ECD are highly conserved across class B GPCRs and play essential roles in agonist binding.
The N-terminal His7 of GLP-1 is required for receptor activation but not for binding: you can create GLP-1 fragments that bind the receptor with high affinity but do not activate it, which is exactly how the antagonist exendin-9-39 works (it uses the exendin-4 C-terminus for high-affinity ECD binding but lacks the activating N-terminus).
GLP-1R Signaling: From Binding To Insulin Exocytosis
GLP-1R couples exclusively and consistently to the Galphas (stimulatory) subunit of heterotrimeric G proteins. R
This is the defining functional identity of GLP-1R: every study to date in which GLP-1R signaling has been examined has found cAMP increases.
Claims that GLP-1R couples to Gq/11 proteins at physiological concentrations have not been substantiated; the few studies showing this used cells overexpressing the receptor at supraphysiological levels.
The core signaling cascade proceeds as follows:
1. Ligand binding and receptor activation. GLP-1 binds the ECD and transmembrane bundle. The receptor undergoes conformational change. The Galphas subunit exchanges GDP for GTP, dissociates from Gbetagamma, and both are now free to activate downstream effectors.
2. Adenylyl cyclase activation and cAMP generation. Galphas activates membrane-bound adenylyl cyclase (AC). AC converts ATP to cyclic AMP (cAMP). cAMP rises rapidly within seconds of GLP-1R activation. R
3. PKA activation. cAMP binds to the regulatory subunits of protein kinase A (PKA), releasing the catalytic subunits. PKA phosphorylates multiple targets. In pancreatic beta cells, PKA closes ATP-sensitive potassium channels (K-ATP channels), causing membrane depolarization. Depolarization opens voltage-gated L-type calcium channels, flooding the cell with Ca2+. The Ca2+ spike triggers exocytosis of insulin-containing granules. PKA also phosphorylates CREB, activating insulin gene transcription and increasing insulin synthesis.
4. Epac activation. cAMP also activates exchange protein directly activated by cAMP (Epac1 and Epac2). Epac2 activates Rap1, which mobilizes additional intracellular Ca2+ stores via ryanodine receptors and IP3 receptors, amplifying the exocytotic signal. Epac-mediated signaling operates in parallel with PKA and extends the duration of the secretory response.
5. PI3K/Akt pathway. GLP-1R activation also engages class I PI3Ks through the Gbetagamma subunits released during G protein activation. PI3K converts PIP2 to PIP3, activating Akt. Akt enhances beta cell survival, promotes beta cell proliferation, and improves peripheral insulin sensitivity. R
Glucose dependence is the critical safety feature.
K-ATP channel closure in beta cells only causes insulin exocytosis when blood glucose is elevated.
At fasting glucose levels, the cell is already relatively depolarized and the GLP-1 signal adds to an insufficient baseline.
This is why GLP-1 receptor agonists essentially cannot cause hypoglycemia when used as monotherapy.
They amplify glucose-stimulated insulin secretion rather than causing glucose-independent secretion the way sulfonylureas do.
In pancreatic alpha cells, GLP-1R expression is lower.
GLP-1 suppresses glucagon primarily through indirect paracrine mechanisms: the insulin secreted by beta cells inhibits alpha cells, and somatostatin secreted by delta cells (also stimulated by GLP-1R activation) inhibits glucagon release. R
Receptor Internalization, Endosomal Signaling, And Biased Agonism
This section matters specifically for understanding why different pharmaceutical agonists have different pharmacological profiles despite acting at the same receptor.
After ligand binding and G protein activation, GLP-1R undergoes a standard GPCR desensitization sequence:
1. Phosphorylation by GRKs. G protein-coupled receptor kinases (GRKs) phosphorylate serine and threonine residues on the receptor's intracellular C-terminal tail.
2. Beta-arrestin recruitment. Phosphorylated GRK sites recruit beta-arrestin-2 (and to a lesser extent beta-arrestin-1). Beta-arrestins sterically block further G protein coupling, terminating cAMP generation. They also serve as scaffolds for clathrin-mediated endocytosis.
3. Receptor internalization. The GLP-1R/beta-arrestin complex is internalized into endosomes. This reduces cell surface receptor density, blunting subsequent responses to agonist (desensitization/downregulation). R
4. Endosomal signaling. Here is the counterintuitive discovery: internalized GLP-1Rs can continue generating cAMP from inside endosomes. Galphas is recruited to Rab5-positive early endosomes where it activates adenylyl cyclase. This compartmentalized endosomal cAMP contributes to insulin granule exocytosis. Blocking receptor internalization with dominant-negative dynamin constructs reduces GLP-1R cAMP responses, confirming that endosomal signaling is functionally significant. R
5. Recycling or degradation. Endosomal GLP-1Rs are sorted either back to the plasma membrane for reactivation (recycling) or to lysosomes for degradation. The metalloprotease ECE1 in endosomes facilitates recycling by processing endosomal GLP-1, promoting receptor release from the endosome. Fast-recycling ligands (like native GLP-1) lead to better receptor recovery than slow-recycling ligands (like exendin-4).
Biased agonism refers to the ability of different ligands to differentially engage Galphas signaling versus beta-arrestin recruitment at the same receptor.
A biased agonist that preferentially activates Galphas without recruiting beta-arrestin would produce cAMP-mediated insulin secretion without receptor internalization and desensitization.
This would theoretically allow sustained signaling without the receptor downregulation seen with chronic agonist exposure.
The concept is pharmacologically important because pharmaceutical GLP-1R agonists differ in their degree of biased agonism: some trigger more beta-arrestin recruitment (and therefore more rapid receptor internalization and potential desensitization) than others. R
This is an active area of drug development.
GLP-1R Distribution: Everywhere That Matters
GLP-1R is not just a pancreatic receptor.
Its expression in multiple organ systems explains GLP-1's effects far beyond glucose metabolism and is the biological basis for the expanding clinical applications of GLP-1R agonists. R
Pancreas: highest expression; beta cells (insulin secretion), alpha cells (glucagon suppression indirect), delta cells (somatostatin secretion).
Central nervous system: hypothalamus (appetite suppression, satiety signaling), brainstem nucleus of the solitary tract (gastric motility regulation), reward circuitry (dopaminergic modulation), cortex. GLP-1R in the CNS mediates the appetite-suppressing and nausea-inducing effects of GLP-1R agonists. This is also where potential neurodegeneration-protective effects arise.
Heart: ventricular and atrial cardiomyocytes; GLP-1R activation improves myocardial glucose uptake, reduces ischemia-reperfusion injury, has mild chronotropic effects (increased heart rate, a common side effect of pharmaceutical agonists).
Kidneys: proximal tubule and collecting duct; GLP-1R activation reduces sodium reabsorption, has natriuretic effects, and may slow decline in estimated GFR.
Gastrointestinal tract: enteric nervous system, gastric parietal cells, intestinal L-cells (auto-stimulation); GLP-1R activation slows gastric emptying, which delays glucose absorption and contributes to postprandial satiety.
Liver: GLP-1R expression is low and debated; effects on hepatic gluconeogenesis and lipid metabolism may be indirect, mediated via the CNS and pancreatic hormones rather than direct hepatic GLP-1R activation.
Skeletal muscle: present but expression is low; effects on muscle glucose uptake appear partially mediated through insulin.
Immune cells: macrophages, lymphocytes, natural killer T cells; GLP-1R activation has anti-inflammatory effects through PKA-mediated CREB activation and NF-kB inhibition. R
What GLP-1 Actually Does In The Body
Synthesizing the receptor distribution above into physiological function:
Glucose regulation: Augments glucose-stimulated insulin secretion from beta cells. Suppresses glucagon secretion from alpha cells (indirectly via insulin and somatostatin). Reduces hepatic gluconeogenesis. Slows gastric emptying, flattening the postprandial glucose curve. All of these effects are glucose-dependent: they are attenuated or absent during fasting or hypoglycemia.
Appetite and body weight: GLP-1R activation in the hypothalamus and brainstem generates satiety signals. Slowed gastric emptying extends the physical sensation of fullness. GLP-1R agonists reduce caloric intake and body weight not primarily through nausea (though nausea is a side effect) but through central satiety signaling.
Beta cell protection: GLP-1 promotes beta cell proliferation and neogenesis in animal models. It inhibits beta cell apoptosis through PI3K/Akt-mediated survival signaling. Whether these effects are clinically significant in humans is still under investigation, but they suggest GLP-1R agonists may slow disease progression in type 2 diabetes beyond glucose control.
Cardiovascular effects: Mild chronotropy (increased heart rate 2-5 bpm, a consistent side effect of pharmaceutical agonists). Improved myocardial glucose uptake and mitochondrial function during ischemia. Reduced vascular inflammation. Anti-atherosclerotic effects through improved lipid profiles and direct endothelial effects.
Pharmaceutical GLP-1 Receptor Agonists
The pharmaceutical development of GLP-1R agonists required solving the DPP-4 degradation problem.
Native GLP-1 has a 2-minute half-life; a therapeutic agent needs at least hours.
Three strategies have been employed: (1) substituting Ala8 to prevent DPP-4 cleavage, (2) acylation or albumin binding to extend half-life via albumin recycling, and (3) using structurally distinct peptides (like exendin-4 from Gila monster venom) that are resistant to DPP-4 from the start.
Exenatide (Byetta, Bydureon)
Exenatide is the synthetic form of exendin-4, a 39 amino acid peptide originally isolated from the saliva of the Gila monster (Heloderma suspectum). R
It shares 53% sequence identity with human GLP-1 but has glycine at position 2 (instead of alanine), making it resistant to DPP-4 cleavage.
Exenatide also lacks DPP-4 cleavage sites in its longer C-terminus, contributing further to stability.
Half-life: approximately 2-4 hours (twice-daily injection for immediate-release Byetta) or 2 weeks (once-weekly Bydureon extended-release microspheres).
Exenatide was the first GLP-1R agonist approved by the FDA, in 2005.
It produces modest HbA1c reductions and 2-3 kg weight loss at the 10 mcg twice-daily dose.
Liraglutide (Victoza, Saxenda)
Liraglutide is a GLP-1 analog with 97% sequence identity to native GLP-1, differing by one amino acid substitution (Arg34 to Lys) and the addition of a C-16 fatty acid chain via a glutamic acid linker.
The fatty acid chain enables reversible albumin binding, dramatically extending half-life to approximately 13 hours through albumin recycling via the neonatal Fc receptor.
Approved for type 2 diabetes (Victoza, 1.2-1.8 mg daily) and obesity (Saxenda, 3.0 mg daily).
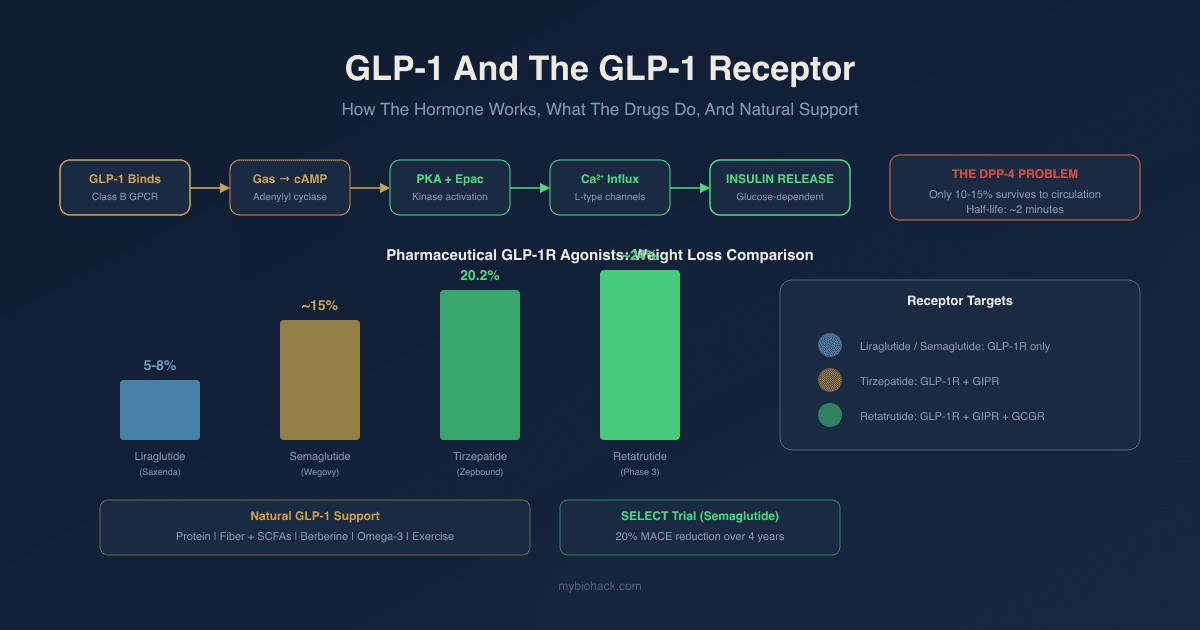
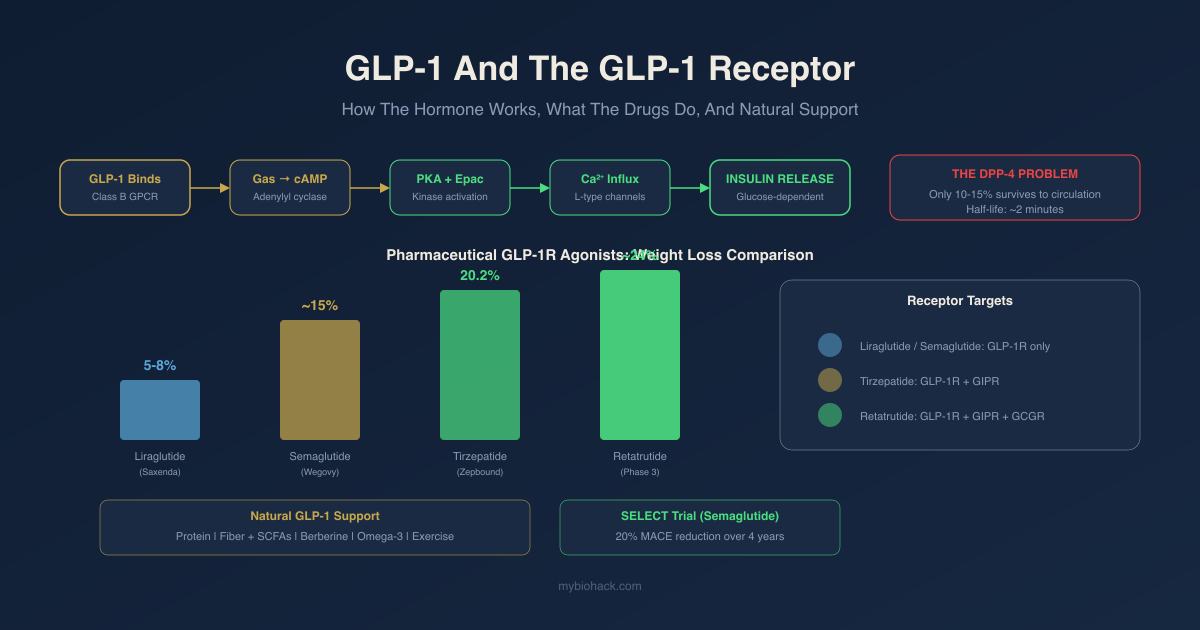
At the 3.0 mg obesity dose, liraglutide produces approximately 5-8% body weight reduction in clinical trials.
Semaglutide (Ozempic, Wegovy, Rybelsus)
Semaglutide has two amino acid modifications from native GLP-1 (Aib8 substitution for DPP-4 resistance, Arg34 to Lys) and a C-18 fatty diacid chain via a two-Aeg linker that provides far stronger albumin binding than liraglutide.
Half-life: approximately 7 days.
Once-weekly subcutaneous injection (Ozempic 0.5-2 mg for type 2 diabetes, Wegovy 2.4 mg for obesity) or once-daily oral tablet (Rybelsus 3-14 mg, with only approximately 1% oral bioavailability requiring absorption through a SNAC co-absorption technology).
Wegovy (2.4 mg weekly) is currently the most effective single-receptor GLP-1R agonist.
The STEP trials showed approximately 15% body weight reduction over 68 weeks in adults with obesity without diabetes.
The SELECT trial showed a 20% reduction in major adverse cardiovascular events (MACE) in 17,604 adults with preexisting cardiovascular disease, overweight or obesity, but without diabetes, over 4 years. R
This cardiovascular benefit is partly independent of weight loss.
Tirzepatide (Mounjaro, Zepbound)
Tirzepatide is the first approved dual agonist, acting at both GLP-1R and the glucose-dependent insulinotropic peptide receptor (GIPR).
It is a 39 amino acid synthetic peptide, sometimes called a "twincretin," that was specifically designed to agonize both incretin receptors simultaneously.
GIPR activation adds complementary metabolic effects: further reduction in food intake, enhanced energy expenditure, and potentially improved adipose tissue function.
Approved for type 2 diabetes (Mounjaro) and obesity (Zepbound).
The SURMOUNT-5 Phase 3 trial directly compared tirzepatide vs. semaglutide 2.4 mg at 72 weeks: tirzepatide produced 20.2% mean body weight reduction vs. 13.7% with semaglutide, with tirzepatide patients 2 times more likely to achieve 25% or greater weight loss. R
Real-world cardiovascular outcome data show similar levels of MACE reduction for tirzepatide and semaglutide in patients with obesity and type 2 diabetes. R
Retatrutide (Phase 3)
Retatrutide is a triple agonist at GLP-1R, GIPR, and the glucagon receptor (GCGR).
Adding glucagon receptor agonism increases energy expenditure and lipolysis beyond what GLP-1/GIP dual agonism achieves, at the cost of some potential increase in hepatic glucose output (which GLP-1R co-activation is intended to offset).
In the Phase 2 NEJM trial, retatrutide at 12 mg weekly produced approximately 24% mean body weight reduction at 48 weeks, the highest published efficacy of any single agent to date. R
Phase 3 trials are ongoing.
DPP-4 Inhibitors (Gliptins)
A separate but related class of drugs: rather than providing exogenous GLP-1R agonists, DPP-4 inhibitors (sitagliptin/Januvia, saxagliptin/Onglyza, linagliptin/Tradjenta, alogliptin/Nesina) block the enzyme that degrades native GLP-1.
This raises native GLP-1 levels 2-3 fold.
Effect is modest compared to injectable agonists because you are amplifying a physiological signal (10-50 pmol/L) rather than achieving pharmacological concentrations.
HbA1c reduction: approximately 0.5-0.8%.
Minimal weight loss effect.
No cardiovascular outcome benefit (neutral in large trials).
Useful primarily in patients who cannot tolerate injectable agonists and want a simpler add-on to metformin.
Natural GLP-1 Stimulators And Mimetics
Before covering these, the honest context: no natural strategy comes remotely close to the pharmacological GLP-1R activation achieved by pharmaceutical agonists.
Native GLP-1 has a 2-minute half-life and peaks at 50 pmol/L postprandially.
Pharmaceutical agonists achieve sustained receptor engagement at concentrations orders of magnitude higher.
Natural strategies work within the physiological system; they improve the GLP-1 pulse you generate from food rather than bypass it.
That is still worth doing, because poor dietary patterns suppress GLP-1 secretion, damage L-cell function, and dysregulate the physiological system.
Restoring physiological GLP-1 function is meaningful for metabolic health even if it does not produce pharmaceutical-grade weight loss.
Dietary Protein
Protein is the strongest macronutrient stimulus for GLP-1 secretion from L-cells.
Amino acids reaching the gut stimulate L-cells directly via amino acid sensing receptors (including GPRC6A and CaSR).
Whey protein, due to rapid digestion and high leucine content, produces one of the strongest acute GLP-1 responses among protein sources.
Distributing 25-30g protein across each meal provides consistent L-cell stimulation throughout the day rather than concentrating protein in one meal.
Dietary Fiber And Short-Chain Fatty Acids
Fermentable dietary fiber (inulin, FOS, resistant starch, pectin, beta-glucan) reaches the colon where gut bacteria ferment it to short-chain fatty acids (SCFAs): butyrate, propionate, and acetate.
SCFAs activate free fatty acid receptors FFAR2 (GPR43) and FFAR3 (GPR41) on L-cells, directly stimulating GLP-1 secretion. R
Butyrate additionally directly stimulates GLP-1 expression in L-cells and promotes L-cell differentiation from intestinal progenitors.
Fiber has a dual mechanism: immediate direct L-cell stimulation from fiber particles, and sustained delayed stimulation via SCFA production.
This makes fiber consistently the strongest natural GLP-1 enhancer with human evidence.
Target: 30-40g/day of varied fermentable fiber.
Dietary Fats And Bile Acids
Dietary fat stimulates GLP-1 through two mechanisms.
First, long-chain fatty acids directly activate GPR120 (FFAR4) and GPR40 (FFAR1) on L-cells, triggering GLP-1 secretion.
Second, fat ingestion triggers bile acid release from the gallbladder.
Bile acids activate TGR5 (Takeda G-protein-coupled receptor 5) on L-cells, a distinct receptor that potently stimulates GLP-1 secretion. R
This explains why mixed meals (protein + fat + fiber) produce stronger and more sustained GLP-1 responses than any single macronutrient alone.
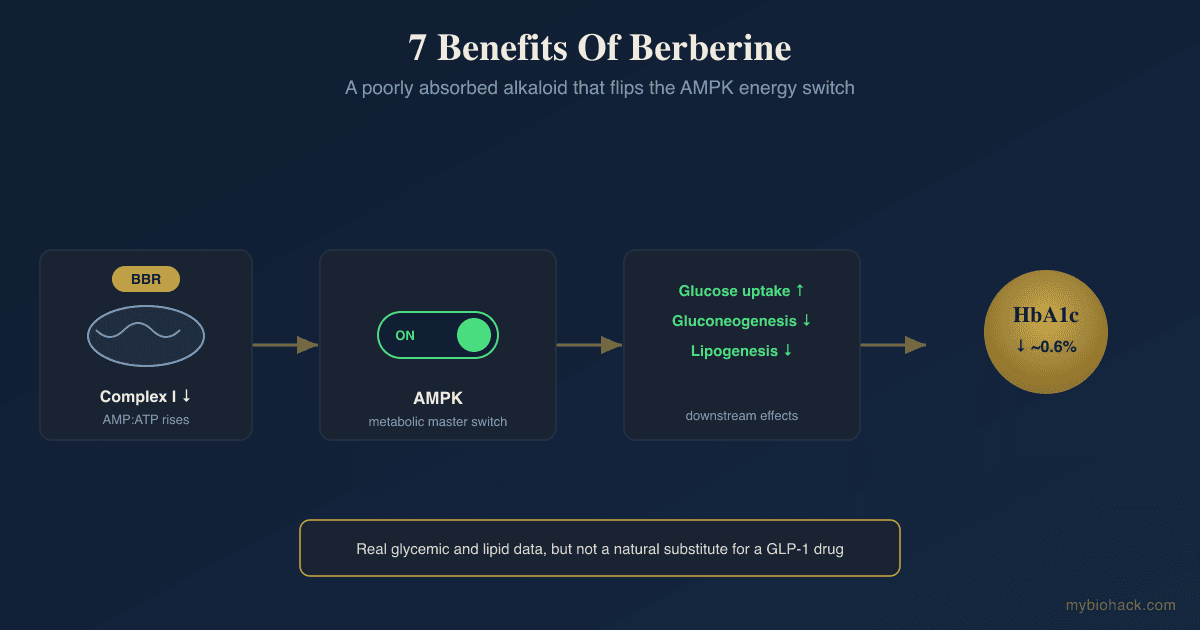
Berberine
Berberine (BBR) is the most studied natural compound for GLP-1 system support.
Its mechanisms are multiple and interrelated.
BBR activates AMPK (AMP-activated protein kinase), the cellular energy sensor, through inhibition of mitochondrial complex I.
BBR restores GLP-1 secretion in diet-induced obese models by reversing mitochondrial dysfunction in colon enterocytes, directly preventing the L-cell mitochondrial damage that suppresses GLP-1 expression under metabolic stress. R
BBR reshapes the gut microbiome toward increased SCFA-producing bacteria (Blautia, Akkermansia muciniphila), indirectly amplifying SCFA-mediated GLP-1 stimulation. R
Berberine metabolites (berberrubine, palmatine) show direct stimulation of GLP-1 production in cell studies.
A meta-analysis of 37 studies found berberine reduced fasting blood glucose and HbA1c comparably to conventional diabetes medications, suggesting the GLP-1 axis is a meaningful part of its metabolic action.
The honest caveat: berberine's clinical weight loss effect is approximately 2-4 kg in most trials, a fraction of pharmaceutical agonist outcomes.
It supports the physiological GLP-1 system rather than pharmacologically overriding it.
Dose: 500mg three times daily with meals.
Berberine inhibits CYP2D6 and CYP3A4 and can interact with metformin, statins, and blood thinners; consult a practitioner before combining.
Dietary Fiber Supplementation
Where whole food fiber is insufficient, targeted fiber supplements provide consistent prebiotic support for GLP-1-producing gut bacteria.
Psyllium Husk: soluble fiber with strong evidence for glycemic benefit; dissolves and reaches the colon largely intact.
Inulin / FOS: rapidly fermented by Bifidobacteria and Lactobacilli to SCFAs; strong prebiotic effect on L-cell-stimulating bacteria.
Resistant Starch (green banana flour, raw potato starch): reaches the colon as intact starch, fermented to high-yield butyrate.
Omega-3 Fatty Acids
EPA and DHA activate GPR120 on L-cells and have been associated with improved GLP-1 receptor sensitivity.
Omega-3s also reduce the chronic low-grade inflammation that impairs L-cell function in obesity and metabolic syndrome.
Omega-3 Fish Oil: 2-4g EPA+DHA daily.
Exercise
Acute aerobic exercise increases postprandial GLP-1 secretion.
Chronic aerobic training improves GLP-1 receptor sensitivity in peripheral tissues.
The mechanism includes improved gut blood flow, enhanced L-cell secretory capacity, and improved gut microbiome composition toward SCFA-producing bacteria.
Both aerobic exercise and resistance training contribute, with consistency more important than intensity.
Intermittent Fasting And Meal Timing
Extended fasting periods increase sensitivity to GLP-1 receptor signaling.
Eating earlier in the day (front-loading calories) produces stronger GLP-1 responses than identical caloric intake consumed later.
This aligns with circadian biology: GLP-1 secretion from L-cells is influenced by circadian rhythms in the gut.
Capsaicin
Capsaicin activates TRPV1 channels on L-cells and enteric neurons, triggering GLP-1 secretion via a Ca2+-dependent mechanism.
Preclinical evidence is strong; human trial data showing clinically meaningful GLP-1 augmentation is limited.
Practical application: consuming spicy food is unlikely to produce therapeutic GLP-1 levels but contributes to the overall dietary stimulus.
Clinical Applications Beyond Diabetes
Cardiovascular Disease
The SELECT trial (semaglutide 2.4 mg, 17,604 adults with cardiovascular disease and obesity but without diabetes, 4 years) demonstrated a 20% relative risk reduction in major adverse cardiovascular events. R
This is now an approved indication: semaglutide (Wegovy) is FDA-approved to reduce cardiovascular risk in adults with cardiovascular disease and obesity or overweight, regardless of diabetes status.
The cardiovascular benefit likely has multiple contributors: weight loss reducing hemodynamic stress, direct anti-inflammatory effects through GLP-1R activation on macrophages and endothelium, improved lipid profiles, and reduced blood pressure.
Whether the benefit is fully mediated by weight loss or includes weight-independent GLP-1R cardiac effects is still being studied.
Non-Alcoholic Fatty Liver Disease / MASH
GLP-1R agonists reduce hepatic fat, fibrosis markers, and hepatic inflammation in NASH (now called MASH, metabolic dysfunction-associated steatohepatitis).
Semaglutide showed histological improvement in NASH in Phase 2 trials.
Retatrutide's triple agonism (adding glucagon receptor activity, which increases hepatic fat oxidation) shows particular promise for liver disease.
Resmetirom (a thyroid hormone receptor-beta agonist) has separate approval for MASH, but GLP-1R agonists are now considered in guidelines for this indication.
Kidney Disease
GLP-1R agonists slow decline in eGFR and reduce albuminuria in patients with type 2 diabetes and chronic kidney disease, through both weight-dependent and weight-independent mechanisms (natriuresis, reduced glomerular hyperfiltration, anti-inflammatory effects).
Neurodegeneration
GLP-1R agonists have shown neuroprotective effects in animal models of Alzheimer's and Parkinson's disease through multiple mechanisms: reduced neuroinflammation, improved mitochondrial function, reduced amyloid aggregation, and promotion of neurogenesis.
A JAMA Network Open cohort study found lower incidence of neurodegenerative disease and cerebrovascular events in patients with type 2 diabetes and obesity receiving semaglutide or tirzepatide compared to matched controls. R
Phase 3 trials of semaglutide for Parkinson's disease and Alzheimer's are ongoing.
Obstructive Sleep Apnea (OSA)
GLP-1R agonists significantly reduce OSA severity, both through weight loss (which reduces upper airway fat deposition) and potentially through direct effects on upper airway muscle tone.
Tirzepatide reduced the apnea-hypopnea index (AHI) by 55-63% in Phase 3 trials (SURMOUNT-OSA), compared to approximately 22% in the placebo group.
Side Effects And Safety: What The Evidence Actually Shows
Gastrointestinal Effects
The most common side effects are nausea, vomiting, diarrhea, and constipation, all dose-dependent and most prominent during dose titration.
These occur because GLP-1R activation in the enteric nervous system and brainstem directly slows gastric motility and triggers nausea pathways.
Slow titration dramatically reduces discontinuation rates.
Nausea typically attenuates within 4-8 weeks as the body accommodates.
In SURMOUNT-5, approximately 76-79% of patients in both tirzepatide and semaglutide arms experienced at least one adverse event, most commonly gastrointestinal, with 5.6% of tirzepatide patients and 2.7% of semaglutide patients discontinuing due to GI side effects. R
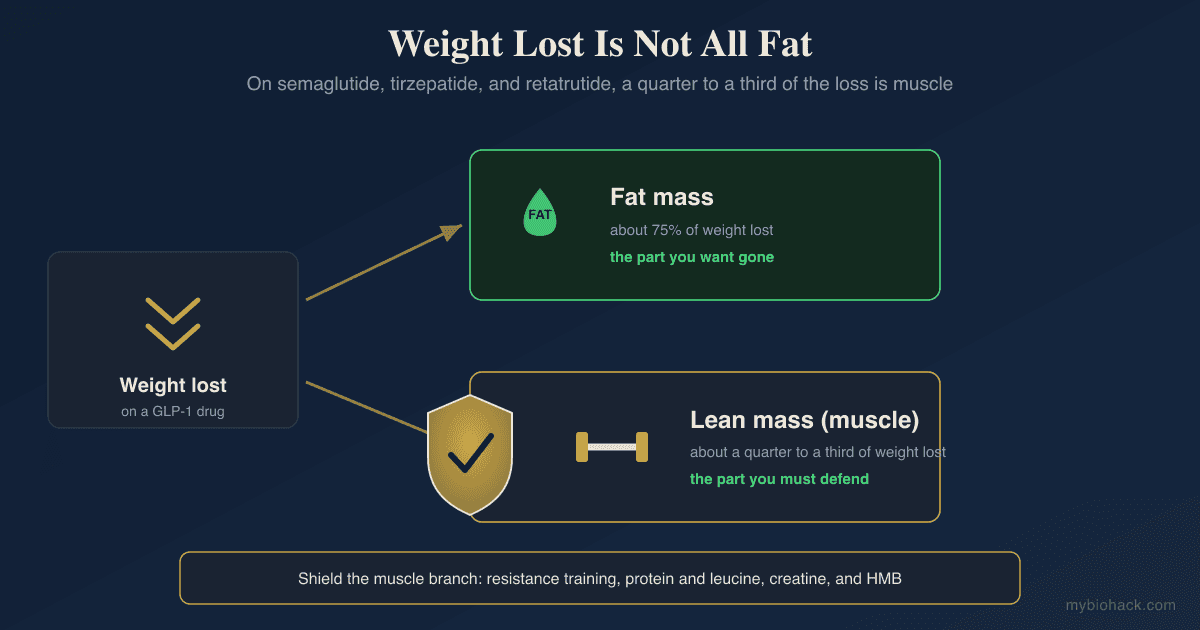
Muscle Mass Loss (Sarcopenia)
This is a genuine and underappreciated concern.
Rapid weight loss from any cause includes loss of lean mass alongside fat mass.
In GLP-1R agonist trials, approximately 25-40% of total weight lost is lean mass rather than fat.
This is more than what occurs with equivalent caloric restriction plus exercise.
The mechanism involves both reduced protein intake (from appetite suppression) and possible direct effects of GLP-1R signaling on skeletal muscle metabolism.
Resistance training and adequate protein intake (1.2-1.6g/kg body weight daily) during treatment are essential to preserve lean mass.
This is a critical gap in current prescribing practice.
Cholelithiasis (Gallstones)
GLP-1R agonists significantly increase gallstone risk, likely through slowed gallbladder motility causing bile stasis.
This was confirmed in multiple large trials.
Risk is increased approximately 2-3 fold compared to placebo.
Patients with prior gallstone disease should be counseled before starting therapy.
Thyroid C-Cell Concerns
GLP-1R agonists carry an FDA boxed warning against use in patients with a personal or family history of medullary thyroid carcinoma (MTC) or Multiple Endocrine Neoplasia type 2 (MEN2).
The warning originates from rodent toxicology studies in which chronic GLP-1R agonist administration caused C-cell hyperplasia, adenomas, and carcinomas in rats and mice.
Rodents have high GLP-1R expression on thyroid C-cells and respond to GLP-1R activation with cAMP-dependent calcitonin secretion and C-cell proliferation.
Humans appear fundamentally different: GLP-1 receptors are expressed on fewer than 30% of human C-cells, and calcitonin levels do not rise in response to GLP-1R agonist administration in humans even in long-term trials. R
Large human observational studies are reassuring: a Scandinavian cohort of 145,000 GLP-1R agonist users found no increased risk for thyroid cancer or MTC. R
A 2024 meta-analysis of 64 randomized controlled trials found a modest statistically significant association (OR 1.52) with low absolute risk increase (5-year number needed to harm: 1,349) and a fragility index of 1, meaning a single event difference would flip statistical significance. R
The honest reading: the FDA boxed warning is appropriate for patients with MTC or MEN2 history as an absolute contraindication.
For patients without those risk factors, the human evidence does not support a clinically meaningful thyroid cancer risk at this point, but long-term data beyond 5 years remain limited.
This warrants continued surveillance rather than alarm.
Pancreatitis
Early pharmacovigilance raised concerns about pancreatitis based on GLP-1R activation in pancreatic acinar cells.
Large randomized trials have not confirmed this.
A systematic review and meta-analysis found no increased risk for pancreatitis with GLP-1R agonists (relative risk 0.96). R
In patients with a history of pancreatitis, caution and physician discussion remain appropriate.
Nonarteritic Ischemic Optic Neuropathy (NAION)
A genuine signal emerged: semaglutide use is associated with increased risk of NAION, a rare condition causing sudden vision loss from ischemia to the optic nerve.
Hazard ratio of 2.81 (95% CI 1.67-4.75) for semaglutide versus SGLT2 inhibitors was found in one study. R
The absolute risk remains low given NAION's rarity, but this is a real finding that warrants discussion with patients who have pre-existing optic disc abnormalities or risk factors for NAION.
Muscle Loss Mitigation
When using pharmaceutical GLP-1R agonists, address lean mass preservation proactively:
Creatine Monohydrate: 5g daily supports muscle energy metabolism and has its own independent anti-atrophy effects.
Leucine or Whey Protein: mTOR activation from leucine stimulates muscle protein synthesis even when caloric intake is reduced.
Resistance training 2-3 times weekly: the non-negotiable component.
What To Stay Away From
- Starting pharmaceutical agonists without a resistance training protocol in place: the lean mass loss during rapid weight loss is a real problem that standard prescribing ignores entirely; if you are going to use these drugs, pair them with progressive resistance training and adequate protein from day one
- Relying on natural GLP-1 strategies expecting pharmaceutical outcomes: berberine, fiber, and protein support the physiological GLP-1 system and provide meaningful metabolic benefit; they do not replicate semaglutide or tirzepatide; being clear-eyed about this prevents both under-treatment of serious metabolic disease and over-investment in unproven natural products
- DPP-4 inhibitors as a substitute for GLP-1R agonists in cardiovascular or weight management indications: gliptins raise native GLP-1 modestly but have no demonstrated cardiovascular outcome benefit and minimal weight effect; the cardiovascular protection seen with semaglutide has not been replicated by DPP-4 inhibitors
- GLP-1R agonists in patients with personal or family history of medullary thyroid carcinoma or MEN2: absolute contraindication per FDA label; the rodent thyroid risk has a plausible human mechanism in this subpopulation even if the general population risk is less clear
- Abrupt discontinuation without a tapering and diet strategy: weight regain is substantial after GLP-1R agonist discontinuation; the physiological systems that the drug was overriding (appetite, satiety) return to their prior state; discontinuation without a plan for diet and lifestyle maintenance almost guarantees most weight is regained within 12 months
- Ignoring cholelithiasis risk: patients on GLP-1R agonists with rapid weight loss should be counseled on gallstone symptoms; right upper quadrant pain, particularly after fatty meals, should prompt immediate evaluation
Testing
The following labs are clinically relevant when starting pharmaceutical GLP-1R agonists or when investigating metabolic dysfunction where GLP-1 biology is relevant.
Comprehensive Metabolic Panel: baseline liver and kidney function; relevant because GLP-1R agonists have renal effects and because NASH is an emerging indication.
HbA1c + Fasting Glucose + Fasting Insulin + HOMA-IR: the metabolic context for deciding pharmaceutical vs. natural GLP-1 strategy, and for monitoring response.
Lipid Panel: GLP-1R agonists improve lipid profiles; baseline required.
Body Composition (DEXA): before and during pharmaceutical agonist use; the lean mass loss concern makes body composition monitoring, not just body weight, essential for appropriate dosing and intervention decisions.
Calcitonin: baseline calcitonin and monitoring during pharmaceutical GLP-1R agonist use is appropriate for patients with any thyroid risk factors; serum calcitonin elevation would be the first signal of C-cell activation.
Mechanisms Of Action
Simple:
- GLP-1 is released from the gut after eating and signals the pancreas to release insulin only when blood sugar is high, which is why drugs that activate the GLP-1 receptor cannot cause hypoglycemia the way insulin does.
- The GLP-1 receptor works like a light switch that activates the cAMP/PKA signaling cascade; when GLP-1 binds, cAMP rises rapidly, PKA activates, potassium channels close, calcium floods in, and insulin granules are released.
- Natural GLP-1 survives for about 2 minutes before an enzyme called DPP-4 destroys it, which is why pharmaceutical drugs were designed to mimic GLP-1 but resist DPP-4 degradation, with some lasting 7 days on a single injection.
- Semaglutide stays active for a week because it is attached to a fatty acid chain that makes it bind reversibly to albumin in the blood, which continually re-releases it as a reservoir and protects it from clearance.
- Tirzepatide adds a second receptor (GIPR) to the GLP-1 target, which explains its greater weight loss versus semaglutide, while retatrutide adds glucagon receptor agonism on top of both, driving even higher energy expenditure and the strongest weight loss data published so far.
Advanced:
- GLP-1R as a class B1 GPCR and the two-domain binding mechanism: Class B GPCRs have a large extracellular N-terminal domain (ECD) that captures the C-terminal region of the peptide ligand with high affinity, positioning the peptide for its second step: insertion of the N-terminal activating sequence into the seven-transmembrane helical bundle. This two-domain model explains why small molecule agonists of class B receptors took decades to develop (they must compete with a two-step docking process), why truncating GLP-1's N-terminus (as DPP-4 does) eliminates agonist activity while retaining some binding affinity, and why exendin-9-39 (which retains the high-affinity C-terminus but lacks the activating N-terminus) acts as a competitive antagonist. Cryo-EM structures of GLP-1R in complex with Gs are now available and have confirmed the two-domain binding model at atomic resolution. R
- cAMP compartmentalization and endosomal signaling: After GLP-1R activation at the plasma membrane, Galphas drives cAMP synthesis for seconds to minutes before GRK-mediated receptor phosphorylation recruits beta-arrestin and triggers clathrin-mediated internalization. Critically, cAMP generation does not stop at the plasma membrane: Galphas follows the internalized receptor into Rab5-positive early endosomes, where it continues to activate adenylyl cyclase within the endosomal lumen. This compartmentalized endosomal cAMP pool signals to different downstream effectors than plasma membrane cAMP, potentially explaining why some GLP-1R agonists (including those that promote slower receptor trafficking) produce qualitatively different cellular responses despite activating the same second messenger. A-kinase anchoring proteins (AKAPs) target PKA to specific subcellular compartments, coupling discrete cAMP signals to calcium mobilization from the ER and insulin granule trafficking. R
- Biased agonism and differential GRK-arrestin engagement: Ligands differ in how strongly they stabilize the active receptor conformation relative to how well they engage GRK phosphorylation sites. A GLP-1R agonist that strongly stabilizes Galphas coupling without efficiently engaging GRKs would produce sustained cAMP signaling without the desensitization that comes from beta-arrestin recruitment. Conversely, an agonist that preferentially recruits beta-arrestin (arrestin-biased agonist) would produce less acute cAMP signaling but might engage arrestin-scaffolded signaling pathways and produce different physiological outputs. Several pharmaceutical agonists have now been characterized for their bias profiles: exendin-4 drives more beta-arrestin recruitment (and correspondingly more receptor internalization) than native GLP-1, which helps explain exendin-4's longer physiological duration despite having a similar receptor on-rate. Tirzepatide's GLP-1R engagement appears to have distinct internalization kinetics compared to semaglutide, possibly contributing to its different efficacy profile. R
- The SCFA-TGR5-L-cell GLP-1 secretion axis: Gut microbiome fermentation of dietary fiber generates butyrate, propionate, and acetate in the colon. Butyrate and propionate activate FFAR2 (GPR43) and FFAR3 (GPR41), Galphai/q-coupled receptors on L-cell basolateral membranes, triggering GLP-1 secretion. Bile acids generated during fat digestion activate TGR5 (a Galphas-coupled receptor on L-cells), also stimulating GLP-1 secretion through a cAMP-dependent mechanism. In parallel, butyrate serves as the primary energy substrate for colonocytes and directly upregulates proglucagon gene expression and L-cell differentiation. This explains why high-fiber diets consistently produce the strongest evidence for natural GLP-1 enhancement: fiber generates SCFAs through fermentation, SCFAs stimulate GLP-1 acutely through FFAR2/3, and butyrate increases L-cell numbers and function chronically through epigenetic mechanisms. R
More Research
- GLP-1R agonists are now indicated for weight management (semaglutide, tirzepatide), type 2 diabetes (all class members), cardiovascular risk reduction in obesity without diabetes (semaglutide 2.4 mg, SELECT trial), and heart failure with preserved ejection fraction (semaglutide, STEP-HFpEF trial); the indication list is expanding rapidly and will likely include MASH, chronic kidney disease, and obstructive sleep apnea within the next several years. R
- The SURMOUNT-5 head-to-head trial (tirzepatide vs. semaglutide 2.4 mg) established tirzepatide's superiority for weight loss (20.2% vs. 13.7% body weight reduction at 72 weeks); tirzepatide's dual GLP-1R/GIPR agonism appears to drive greater weight loss than GLP-1R agonism alone, supporting the hypothesis that GIPR co-agonism is not simply additive. R
- Retatrutide's Phase 2 data (~24% weight loss at 48 weeks) suggests the triple agonist approach may achieve near-bariatric-surgery weight outcomes pharmacologically; Phase 3 data will determine whether this efficacy holds at scale with acceptable tolerability. R
- The lean mass preservation problem with GLP-1R agonists is now acknowledged in guidelines but remains poorly addressed in clinical practice; resistance training and protein adequacy are not optional add-ons during GLP-1R agonist therapy, they are essential to prevent the sarcopenia that otherwise accompanies rapid weight loss in this context.
- Berberine's GLP-1-mediated metabolic effects, while real, are mechanistically rooted in L-cell mitochondrial protection and SCFA-producing microbiome restoration; these are physiological rather than pharmacological effects and should be framed as such; berberine is a meaningful metabolic support agent, not a natural substitute for pharmaceutical agonists. R
- For GLP-1R agonist testing, serum calcitonin provides a functional biomarker for C-cell activity that would be the first signal of thyroid C-cell concern; measuring at baseline and periodically during therapy is appropriate in patients with thyroid risk factors even though large population studies have not confirmed a clinically meaningful thyroid cancer signal in the general population. R
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Electrolyte Complex
1 scoop/day
CoQ10
200mg/day
Magnesium Glycinate
400mg at bedtime