Short Chain Fatty Acids: Acetate, Propionate, Butyrate, And The Minor SCFAs Your Gut Makes Every Day
By Jacob Gordon, INHC, FMT-CThis article contains affiliate links. As an Amazon Associate, MyBioHack earns from qualifying purchases at no extra cost to you. We only link products we research and stand behind.

Short chain fatty acids (SCFAs) are the primary metabolic currency your gut microbiome uses to communicate with your body.
In this post, we will cover the full family of SCFAs, where each one comes from, which bacteria produce them, how they are absorbed and transported, what each one does at the molecular level through its specific receptors and metabolic fates, the minor and branched-chain SCFAs that are underappreciated, how SCFA profiles change in disease, and what raising them actually requires.
What SCFAs Are: Structure And The Full Family
Short chain fatty acids are organic monocarboxylic acids with an aliphatic chain of 1 to 6 carbon atoms.
They are named "short chain" to distinguish them from medium chain fatty acids (6-12 carbons) and long chain fatty acids (above 12 carbons).
The full SCFA family by carbon number:
- Formate (C1) - formic acid, methanoic acid
- Acetate (C2) - acetic acid, ethanoic acid
- Propionate (C3) - propionic acid, propanoic acid
- Isobutyrate (C4, branched) - isobutyric acid, 2-methylpropanoic acid
- Butyrate (C4, straight) - butyric acid, butanoic acid
- 2-Methylbutyrate (C5, branched) - no common name
- Isovalerate (C5, branched) - isovaleric acid, 3-methylbutanoic acid
- Valerate (C5, straight) - valeric acid, pentanoic acid
- Caproate (C6) - caproic acid, hexanoic acid
Acetate, propionate, and butyrate account for approximately 95% of all SCFAs produced in the human gut. R
The approximate molar ratio in colonic contents is 60:20:20 (acetate:propionate:butyrate), though this varies substantially with diet, microbiome composition, and transit time.
The human colon produces approximately 500-600 mmol of SCFAs per day under normal dietary conditions.
How SCFAs Are Made: Fermentation Pathways
All three major SCFAs begin with the same raw material: dietary fiber and resistant starch that escape small intestinal digestion and arrive in the colon intact.
This material is fermented anaerobically by specific gut bacteria.
Acetate biosynthesis:
Two major routes:
- Acetyl-CoA pathway: The dominant route. Pyruvate from glycolysis is converted to acetyl-CoA, which is then converted to acetate via acetate kinase or phosphotransacetylase.
Most enteric bacteria can produce acetate via this pathway.
- Wood-Ljungdahl pathway: Used by acetogenic bacteria (primarily Blautia and other acetogens).
CO2 and H2 generated by other fermentation reactions are captured and reduced to acetate.
This pathway is responsible for approximately one third of total colonic acetate.
It is important for H2 disposal: accumulation of H2 inhibits other fermentations, so acetogens serve as H2 sinks that maintain the efficiency of the entire community. R
Propionate biosynthesis:
Three routes:
- Succinate pathway: The dominant route.
Hexoses and pentoses are converted through the TCA cycle to succinyl-CoA, which is converted to propionate via a vitamin B12-dependent methylmalonyl-CoA mutase.
Used by Bacteroidetes (Prevotella spp., Bacteroides spp.) and Negativicutes (Phascolarctobacterium succinatutens, Veillonella spp.).
- Acrylate pathway: Lactate is reduced to propionate via lactoyl-CoA, acryloyl-CoA, and propionyl-CoA.
Used primarily by Coprococcus spp. (Lachnospiraceae).
- Propanediol pathway: Deoxy sugars (fucose, rhamnose) from host glycans and dietary sources are fermented via 1,2-propanediol to propionate.
Used by Roseburia inulinivorans and some Blautia species.
Butyrate biosynthesis:
Two major routes:
- Butyryl-CoA:acetate CoA transferase pathway: The dominant route.
Acetate from other bacteria is converted to acetyl-CoA, condensed through multiple steps to butyryl-CoA, then the CoA is transferred to acetate to release butyrate and regenerate acetyl-CoA.
Requires an exogenous acetate supply (hence the cross-feeding relationship with acetate producers).
Used by Faecalibacterium prausnitzii, Roseburia spp., Eubacterium hallii.
- Butyrate kinase pathway:
Phosphobutyrate is converted directly to butyrate.
Used by Clostridium butyricum and some other clostridia.
Less dominant in the human gut than the transferase pathway. R
Cross-Feeding: How Bacteria Cooperate To Produce SCFAs
One of the most important concepts in gut SCFA production is cross-feeding: the cooperative metabolic relationship where the waste product of one species becomes the essential substrate for another.
The central cross-feeding loop in butyrate production:
Step 1: Primary fermenters (Bacteroides, Ruminococcus, Bifidobacterium) break down complex polysaccharides and produce acetate plus hydrogen (H2) and CO2.
Step 2: Acetogenic bacteria (Blautia, Ruminococcus hydrogenotrophicus) use H2 and CO2 via the Wood-Ljungdahl pathway to produce more acetate.
This is critical because H2 accumulation would inhibit the primary fermenters; acetogens are H2 sinks that keep the entire system running.
Step 3: Butyrate producers (Roseburia intestinalis, Faecalibacterium prausnitzii, Eubacterium hallii) consume the acetate produced in steps 1 and 2 as the CoA donor for butyrate synthesis via the butyryl-CoA:acetate CoA transferase pathway.
This means that butyrate production depends on acetate production, and acetate production depends in part on H2-consuming acetogens, and the whole system depends on primary fiber degraders.
Disrupting any node in this network (by antibiotics, low fiber diet, or dysbiosis of any primary producer) reduces butyrate output even if butyrate-producing species are still present.
A specific example: Akkermansia muciniphila degrades mucus glycans, releasing oligosaccharides and acetate into the intestinal microenvironment.
Eubacterium hallii then captures that acetate and uses it to produce propionate, butyrate, and vitamin B12. R
How SCFAs Are Absorbed And Transported
The dynamics of SCFA absorption determine which organs actually see each SCFA.
In the colon:
Most SCFAs are produced and immediately absorbed in the proximal colon (cecum and ascending colon) where fermentation is most active and concentrations are highest (cecal pH approximately 5.5-6.0, the most acidic point in the colon).
Absorption occurs via three mechanisms: R
- Simple diffusion of the protonated (undissociated) acid form across the membrane (predominantly in the distal colon where higher pH raises the proportion of the ionized form, limiting simple diffusion)
- MCT1 (monocarboxylate transporter 1/SLC16A1): proton-coupled transporter, the major route under normal conditions
- SMCT1 (SLC5A8): sodium-coupled transporter, high affinity, important under low-SCFA conditions
- Bicarbonate exchange (butyrate/HCO3- counter-transport) at the basolateral membrane
Gradient from gut to periphery:
Portal blood SCFA concentrations (approximately 375 µmol/L) are approximately 5 times higher than peripheral venous blood (approximately 79 µmol/L), reflecting massive first-pass extraction by colonocytes and the liver. R
Hepatic vein SCFA concentrations (approximately 148 µmol/L) are approximately 39% of portal concentrations, showing significant hepatic extraction.
The tissue-specific fate hierarchy:
- Butyrate: mostly oxidized by colonocytes; very little reaches portal circulation or the liver; peripheral blood butyrate is negligible under normal conditions
- Propionate: largely cleared by the liver (first-pass extraction); provides approximately 50% of the substrate for hepatic gluconeogenesis; minimal reaches peripheral circulation
- Acetate: least extracted by colonocytes and liver; the dominant circulating SCFA in peripheral blood; the primary SCFA reaching peripheral tissues and the brain
The peripheral blood molar ratio of acetate:propionate:butyrate is approximately 91:5:4, nearly the inverse of the colon lumen profile, reflecting differential extraction. R
SCFA Receptors: GPR41, GPR43, GPR109A, And OR51E2
SCFAs signal through a specific family of G-protein coupled receptors (GPCRs), each with distinct SCFA preferences, tissue distributions, and downstream effects: R
GPR43 (FFAR2, Free Fatty Acid Receptor 2):
Primary ligands: acetate (high affinity), propionate (moderate)
Coupled to Gi and Gq proteins
Expressed on: immune cells (neutrophils, macrophages, dendritic cells), intestinal epithelium, adipocytes, enteroendocrine cells, pancreatic beta cells
Primary functions: inflammatory cell recruitment and activation; GLP-1 and PYY secretion from enteroendocrine L-cells; adipose tissue lipolysis regulation; insulin secretion modulation
Important in neutrophil recruitment to infection sites (GPR43 on neutrophils responds to bacterial acetate as a signal of infection)
GPR41 (FFAR3, Free Fatty Acid Receptor 3):
Primary ligands: propionate (highest affinity), butyrate, valerate
Coupled to Gi protein
Expressed on: enteroendocrine L-cells, sympathetic ganglion neurons, adipocytes, immune cells
Primary functions: GLP-1 and PYY secretion; sympathetic nervous system activation (heart rate regulation, blood pressure); leptin production from adipocytes; intestinal motility via the enteric nervous system
GPR109A (HCAR2, Hydroxycarboxylic Acid Receptor 2):
Primary ligands: butyrate (highest affinity), beta-hydroxybutyrate (the ketone body); niacin (pharmacological doses)
Coupled to Gi protein
Expressed on: colonocytes, macrophages, dendritic cells, Langerhans cells in skin, adipocytes
Primary functions: anti-inflammatory polarization in macrophages; Treg induction; tumor suppression in colon; flushing reaction (skin Langerhans cells responding to pharmacological niacin doses)
OR51E2 (Olfactory Receptor 51E2):
A recently characterized vascular smooth muscle receptor activated by acetate and propionate.
OR51E2 stimulation causes vascular smooth muscle relaxation, linking SCFA production to vasodilation and blood pressure regulation.
Expressed in arterial smooth muscle throughout the vasculature. R
HDAC inhibition (non-receptor mechanism):
All SCFAs can inhibit histone deacetylase (HDAC) enzymes at sufficient intracellular concentrations, though potency varies substantially.
Butyrate is the most potent HDAC inhibitor of the three major SCFAs.
Propionate has moderate HDAC inhibitory activity.
Acetate is a weak HDAC inhibitor but contributes to nuclear acetyl-CoA pools (since acetate can be converted to acetyl-CoA, the substrate for histone acetyltransferases).
HDAC inhibition causes histone hyperacetylation, opening chromatin and altering gene expression in ways that suppress inflammation and support cellular differentiation. R
Acetate: The Dominant SCFA
Acetate (CH3COO-) is the most abundant SCFA in the human gut and the dominant SCFA in peripheral circulation.
It comprises approximately 60% of total fecal SCFAs.
Primary producers:
- Bacteroides spp. (the dominant acetate producers in the healthy human colon)
- Faecalibacterium prausnitzii
- Bifidobacterium spp. (especially important in infants)
- Blautia spp. and other acetogens via the Wood-Ljungdahl pathway
- Most enteric bacteria produce acetate as a fermentation end product
Metabolic fates:
Unlike butyrate and propionate, acetate is not heavily extracted by colonocytes or the liver at normal concentrations.
It enters the bloodstream and reaches peripheral tissues.
In the liver, acetate is converted to acetyl-CoA and can be incorporated into fatty acid synthesis, cholesterol synthesis, and the TCA cycle.
In the brain, acetate crosses the blood-brain barrier and is converted to acetyl-CoA, contributing to neuronal energy metabolism and acetylcholine synthesis.
In muscle, acetate contributes to fatty acid oxidation and mitochondrial function.
Key roles of acetate:
Energy substrate for peripheral tissues:
Acetate provides a direct oxidative fuel for many tissues beyond the colon, particularly relevant during fasting when gut-derived acetate contributes to systemic energy balance.
Substrate for butyrate production:
Via cross-feeding, colonic acetate is the primary CoA donor for butyrate synthesis in Firmicutes butyrate producers.
Raising acetate availability through Bacteroides-supporting dietary patterns indirectly supports butyrate production downstream.
GLP-1 and PYY secretion:
Colonic acetate signals through GPR43 on enteroendocrine L-cells to stimulate glucagon-like peptide 1 (GLP-1) and peptide YY (PYY) secretion.
GLP-1 stimulates insulin secretion and suppresses glucagon.
PYY slows gastric emptying and reduces appetite.
This gut hormone axis links gut fermentation to appetite regulation, glucose homeostasis, and satiety. R
Immune modulation:
Acetate is the primary SCFA detected at infection sites as a damage-associated signal.
GPR43 on neutrophils responds to acetate as a chemotactic and activating signal.
At the same time, acetate contributes to systemic anti-inflammatory tone via GPR43-mediated regulatory T cell (Treg) induction.
Peripheral acetate (reaching the brain via circulation) activates hypothalamic neurons through FFAR3 receptors, reducing appetite and modifying neuroinflammatory status.
In Alzheimer's disease models, acetate upregulation of FFAR3 inhibits ERK/JNK/NF-kB signaling, reducing neuroinflammation.
Vascular function:
Acetate activates OR51E2 receptors on vascular smooth muscle, driving vasodilation and contributing to blood pressure reduction.
Propionate: The Liver's SCFA
Propionate (CH3CH2COO-) is the three-carbon SCFA with the most direct and mechanistically defined effects on hepatic metabolism.
It comprises approximately 20% of total fecal SCFAs but is present at proportionally very low levels in peripheral blood due to near-complete first-pass hepatic extraction.
Primary producers:
- Bacteroides spp. (succinate pathway, dominant route)
- Prevotella spp. (succinate pathway)
- Phascolarctobacterium succinatutens (succinate pathway, converts succinate to propionate)
- Veillonella spp. (converts lactate to propionate)
- Coprococcus catus (acrylate pathway)
- Roseburia inulinivorans (propanediol pathway from fucose/rhamnose)
- Dialister spp.
Metabolic fate:
Propionate absorbed from the colon travels to the liver via the portal vein, where it is almost entirely extracted.
In the liver, propionate is converted to propionyl-CoA, then to methylmalonyl-CoA (requiring vitamin B12 as cofactor), then to succinyl-CoA, which enters the TCA cycle.
Succinyl-CoA is a gluconeogenic substrate: it can be converted to oxaloacetate and then to glucose via phosphoenolpyruvate carboxykinase (PEPCK) and other gluconeogenic enzymes. R
Approximately 50% of hepatic propionate is used as a gluconeogenic substrate in humans.
Key roles of propionate:
Hepatic gluconeogenesis regulation:
Propionate both supplies substrate for gluconeogenesis and simultaneously suppresses excessive gluconeogenesis through GPR43/AMPK signaling.
When propionate binds hepatic GPR43, it activates CaMKKβ (calcium/calmodulin-dependent protein kinase kinase beta), which phosphorylates and activates AMPK (AMP-activated protein kinase).
AMPK activation downregulates G6Pase (glucose-6-phosphatase) and PEPCK, the rate-limiting enzymes of gluconeogenesis, reducing hepatic glucose output. R
This dual role (gluconeogenic substrate + gluconeogenesis suppressor) makes propionate a self-limiting hepatic glucose regulator.
Cholesterol and lipid metabolism:
Propionate competitively inhibits acetate uptake by liver cells, reducing acetyl-CoA availability for cholesterol and fatty acid synthesis.
Propionate also directly inhibits HMG-CoA synthase (HMGCS) and HMG-CoA reductase (HMGCR), the rate-limiting enzymes of the cholesterol synthesis pathway.
Both in vitro and animal studies show reduced hepatic cholesterol synthesis with propionate supplementation.
Intestinal gluconeogenesis (IGN) and satiety:
Propionate is a substrate for intestinal gluconeogenesis (IGN), the synthesis of glucose by enterocytes in the small intestinal wall.
IGN-derived glucose is detected by portal vein glucose sensors that signal the brain via FFAR3 (GPR41) neural circuits.
This portal glucose signaling reduces appetite, improves insulin sensitivity, and lowers food intake, representing a gut-brain neural circuit that connects bacterial propionate production to metabolic regulation. R
The inulin-propionate ester (a colon-targeted propionate delivery system) given to overweight humans significantly increased post-meal GLP-1 and PYY, reduced calorie intake at a buffet meal, and over 24 weeks reduced weight gain.
GLP-1 and PYY secretion:
Like acetate, propionate signals through GPR41 and GPR43 on enteroendocrine L-cells to trigger GLP-1 and PYY secretion, contributing to satiety and improved glucose tolerance.
Anti-inflammatory effects:
Propionate reduces NF-kB activation in immune cells via GPR43-Gi signaling.
It stimulates neutrophil, macrophage, and dendritic cell responses at infection sites while dampening systemic inflammatory tone.
In the CNS, propionate reduces stress behavior in mice at low doses, but causes neurotoxic effects at high doses (relevant to propionic acidemia, a rare metabolic disorder discussed below).
Blood pressure:
Propionate activates OR51E2 on vascular smooth muscle alongside acetate, contributing to vasodilation.
Butyrate: The Colonocyte's Primary Fuel
Butyrate (CH3CH2CH2COO-) is the four-carbon straight-chain SCFA that has received by far the most research attention for its profound effects on colonocyte health, intestinal immunity, and epithelial barrier integrity.
It comprises approximately 15-20% of total fecal SCFAs but is present at negligible levels in peripheral blood due to near-complete colonocyte oxidation.
This section provides a high-level overview; the dedicated post on butyrate goes into the full molecular detail.
Primary producers:
- Faecalibacterium prausnitzii (most abundant butyrate producer in healthy human colon)
- Roseburia intestinalis, Roseburia hominis
- Eubacterium hallii, Eubacterium rectale
- Anaerostipes spp.
- Coprococcus catus, Coprococcus comes
- Clostridium butyricum
Metabolic fate:
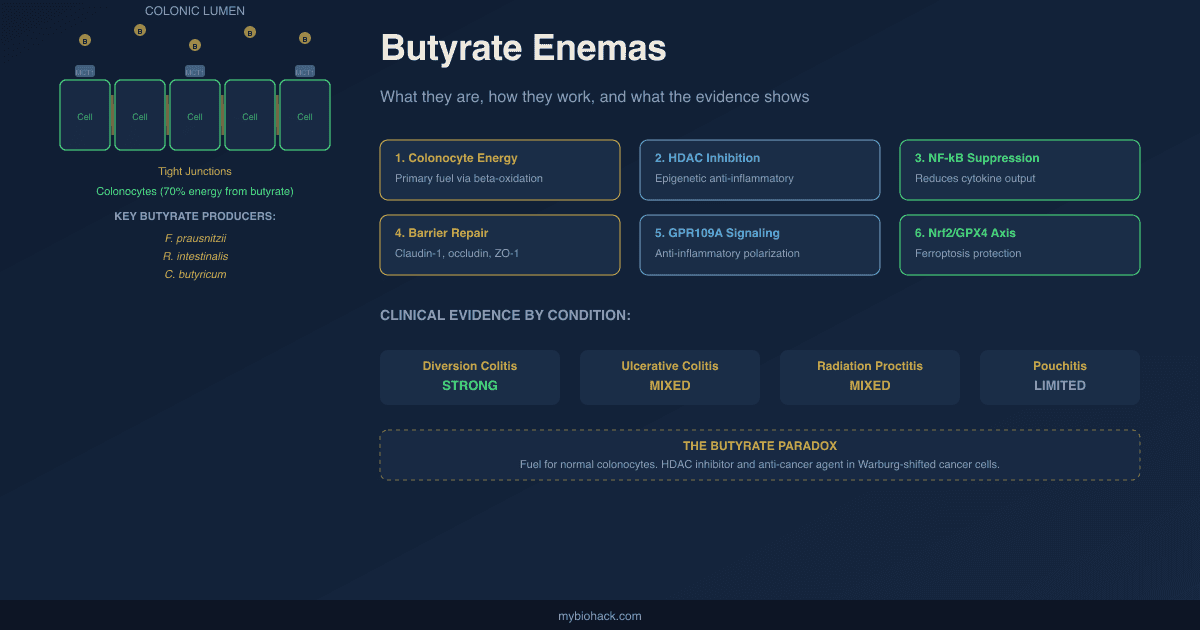
Approximately 70% of colonocyte energy requirements are met by butyrate oxidation.
Butyrate enters colonocytes via MCT1 and SMCT1, enters the mitochondria, and is oxidized to acetyl-CoA via beta-oxidation, which enters the TCA cycle to produce ATP. R
This near-complete oxidation maintains physiological colonic hypoxia, stabilizing HIF-1alpha and driving tight junction protein expression.
Very little butyrate reaches the liver or systemic circulation.
Key roles of butyrate:
- Colonocyte energy supply (70% of colonocyte ATP needs)
- HDAC inhibition at elevated intracellular concentrations (notably in inflamed or cancer cells)
- NF-kB suppression via GPR109A and HDAC inhibition
- Tight junction protein induction (claudin-1, occludin, ZO-1) via IL-10RA upregulation
- Regulatory T cell (Treg) induction via HDAC inhibition at FOXP3 loci
- Ferroptosis protection via Nrf2/GPX4 upregulation
- GPR109A-mediated anti-inflammatory polarization of colonic macrophages and dendritic cells
- HIF-1alpha stabilization via oxygen consumption, maintaining colonic anaerobiosis
- Tumor suppression via HDAC inhibition in colorectal cancer cells (the "butyrate paradox")
Valerate And Caproate: The Minor Straight-Chain SCFAs
Valerate (C5, pentanoic acid) is the five-carbon straight-chain SCFA produced in small amounts by gut bacteria.
It is less than 5% of total fecal SCFAs under normal conditions.
Valerate producers:
Valerate is produced from valine (a branched-chain amino acid) via amino acid fermentation by:
- Prevotella stercorea
- Megasphaera elsdenii
- Prevotella copri
Valerate can also be produced from butyrate extension pathways in some bacteria.
What valerate does:
Valerate inhibits C. difficile growth in chemostat models, contributing to colonization resistance alongside butyrate and secondary bile acids.
It activates GPR41 and GPR43, similar to the other straight-chain SCFAs, contributing to GLP-1 and PYY secretion.
Valerate is an HDAC inhibitor, structurally similar enough to butyrate to compete at the active site.
Valproate (valproic acid), a pharmaceutical HDAC inhibitor and anticonvulsant used for epilepsy, bipolar disorder, and migraine prophylaxis, is the sodium salt of 2-propylvaleric acid, a valerate derivative.
The pharmacological use of valproate as an epigenetic modifier mirrors the biology of gut-derived valerate at much lower concentrations.
Caproate (C6, hexanoic acid) is produced from lactate via cross-feeding in specific bacterial communities.
Some Clostridium species and Megasphaera elsdenii can extend fatty acid chains to caproate from butyrate via reverse beta-oxidation.
Caproate has demonstrated antifungal activity, particularly against Candida species, making it a candidate for gut-based antifungal defense.
Its levels are very low under normal conditions and its physiological roles are less defined than the C2-C5 SCFAs. R
Branched-Chain SCFAs: Isobutyrate, Isovalerate, 2-Methylbutyrate
The branched-chain short chain fatty acids (BCFAs) are a structurally distinct group produced primarily from the fermentation of amino acids rather than carbohydrates.
This metabolic distinction makes them fundamentally different signals from the straight-chain SCFAs: while acetate, propionate, and butyrate are markers of fiber fermentation and microbial health, BCFAs are markers of protein fermentation and potentially of microbial dysbiosis or high-protein, low-fiber diet patterns. R
The three BCFAs:
Isobutyrate (C4, branched, 2-methylpropanoic acid):
Produced from fermentation of valine by Clostridium spp., Bacteroides spp., and others.
A small amount is produced by HSD3B2 from amino acid precursors.
Isovalerate (C5, branched, 3-methylbutanoic acid):
Produced from fermentation of leucine.
Leucine is transaminated to alpha-ketoisocaproate, then oxidatively decarboxylated via branched-chain alpha-keto acid dehydrogenase (BCKDH) to isovaleryl-CoA, then hydrolyzed to isovalerate.
Producers include: Prevotella spp., Clostridium spp., Bacteroides spp.
A recently proposed alternative pathway via a novel enzyme carrying iron-sulfur clusters has been identified in gut commensals including Prevotella, Blautia, Christensenella, and Ruminococcus species. R
2-Methylbutyrate (C5, branched):
Produced from fermentation of isoleucine.
Produced by some Clostridium and Bacteroides species.
BCFAs as markers:
The ratio of straight-chain SCFAs to BCFAs in feces serves as an index of carbohydrate fermentation versus protein fermentation.
A low SCFA/BCFA ratio indicates that bacteria have run out of fermentable carbohydrate and have shifted to amino acid catabolism.
BCFAs increase with aging (relative to straight-chain SCFAs), consistent with the reduction in fiber intake and butyrate-producing bacteria in older adults.
BCFAs are elevated in high-protein, low-fiber dietary patterns.
Isovalerate and isobutyrate increase in feces after bariatric surgery, possibly reflecting altered protein digestion and microbiome changes post-operatively.
Biological effects of BCFAs:
BCFAs are largely considered less beneficial than straight-chain SCFAs at high concentrations, for several reasons:
They are weaker HDAC inhibitors than butyrate.
They are markers of a fermentation environment that produces co-metabolites (phenolic compounds, indoles, amines, ammonia) that can damage the colonic epithelium at high concentrations.
However, isovalerate at physiological concentrations (3-5 mM) enhances intestinal epithelial barrier function, as demonstrated in recent work showing similar mechanisms to butyrate (tight junction protein upregulation, potentially via HDAC inhibition).
The effects are dose-dependent: low physiological concentrations appear beneficial; high concentrations from excessive protein fermentation shift the balance toward pro-inflammatory and cytotoxic outputs.
Isovalerate, isobutyrate, and 2-methylbutyrate all activate GPR41 (FFAR3), contributing to the signaling effects associated with this receptor (GLP-1/PYY secretion, enteric nervous system stimulation) though with lower potency than the straight-chain SCFAs. R
Formate And Lactate: Upstream Precursors
Formate (C1, formic acid) is produced in the gut by several pathways:
- As a byproduct of Bifidobacterium metabolism of human milk oligosaccharides (HMOs) in infants, particularly when HMO degradation is incomplete
- By Eubacterium hallii from 1,2-propanediol (yielding formate plus propionate and butyrate)
- As an intermediate in the Wood-Ljungdahl pathway before reduction to acetyl-CoA
Formate specifically decreases phagocytic activity of macrophage-like cells in vitro, suggesting an immunomodulatory role, though its systemic significance in humans is less established than the C2-C4 SCFAs.
Lactate is not technically an SCFA (it is a hydroxy acid) but functions as a critical upstream precursor in the SCFA network.
Lactate-producing bacteria (Bifidobacterium, Lactobacillus, Streptococcus, Staphylococcus) are especially dominant in infancy and in the proximal colon.
Lactate is then consumed by:
- Secondary lactate utilizers that convert it to propionate (via the acrylate pathway: Coprococcus catus, Megasphaera elsdenii)
- Butyrate producers (Eubacterium hallii, Anaerostipes spp.) that use lactate plus acetate to produce butyrate
This lactate-to-SCFA conversion is why probiotic Lactobacillus strains, despite not producing butyrate directly, can support butyrate production by providing lactate substrate to butyrate-producing commensals.
Lactate accumulation (when secondary utilizers are absent) is associated with lactic acidosis in the colon and is a feature of some dysbiosis states, especially post-antibiotic disruption. R
SCFA Profiles In Disease
SCFA production is not static; it reflects the health of the fiber-microbiome-metabolism axis and shifts detectably in most chronic conditions.
Inflammatory bowel disease (IBD):
Fecal butyrate, acetate, and propionate are all reduced in active UC and Crohn's disease, with butyrate-producing bacteria (Faecalibacterium prausnitzii, Roseburia hominis) specifically depleted.
Both species show inverse correlation with disease activity score.
Fecal calprotectin in UC patients (a marker of mucosal inflammation) correlates with SCFA levels, suggesting that inflammation and SCFA depletion are co-occurring rather than one strictly causing the other. R
Type 2 diabetes and metabolic syndrome:
Fecal SCFA profiles in metabolic disease are complex: some studies show reduced fecal SCFAs (consistent with dysbiosis), while others show elevated fecal SCFAs (consistent with malabsorption and reduced colonic uptake).
Plasma propionate is reduced in insulin-resistant states, consistent with the role of propionate in hepatic glucose regulation.
Gut microbiota transplants from metabolically healthy donors to metabolically compromised recipients improve insulin sensitivity partly through SCFA mechanisms, particularly propionate-mediated effects on hepatic gluconeogenesis.
MASLD/NAFLD:
Elevated plasma propionate, formate, valerate, and alpha-methylbutyrate are observed in MASLD patients compared to healthy controls.
Butyrate supplementation in MASLD models enhances GLP-1 receptor expression by inhibiting HDAC-2, promotes fatty acid oxidation by activating AMPK, and reduces hepatic fat deposition.
Colorectal cancer:
Fecal SCFAs (particularly butyrate) are reduced in colorectal cancer patients, consistent with the depletion of butyrate-producing bacteria and the loss of MCT1 and SMCT1 transporters in cancer cells.
The BCFAs (isobutyrate, isovalerate) are relatively elevated compared to straight-chain SCFAs in CRC, consistent with protein fermentation replacing fiber fermentation in a dysbiotic colon.
Aging:
Total fecal SCFA concentrations decrease with age, particularly acetate and propionate.
BCFAs increase proportionally with aging, indicating a shift from carbohydrate fermentation to protein fermentation.
This shift correlates with reduced fiber intake, loss of butyrate-producing Firmicutes, and increased inflammatory tone (inflammaging). R
Propionic acidemia:
This rare inborn error of metabolism involves a deficiency of propionyl-CoA carboxylase, causing systemic propionate accumulation.
At pathologically high concentrations, propionate is neurotoxic, causing mitochondrial dysfunction, disruption of TCA cycle function (propionic acid competes with acetate for CoA), and neurological damage.
This disease illustrates the dose-dependency of propionate biology: physiological gut-derived concentrations are beneficial; systemic accumulation from enzyme deficiency is catastrophic.
It also illustrates that the route of delivery (portal vein propionate from gut vs. systemic accumulation from enzyme deficiency) matters as much as the amount.
The Fiber-SCFA-Microbiome Triangle
SCFA production depends entirely on delivering fermentable substrate to the colon.
The primary determinants of colonic SCFA production:
1. Dietary fiber intake and type:
Different fiber types preferentially produce different SCFA profiles:
- Inulin and fructooligosaccharides (FOS): increase Bifidobacterium and Lactobacillus, primarily increase acetate
- Arabinoxylan: increases Bacteroides and Prevotella, primarily increases propionate
- Resistant starch: primarily feeds Ruminococcus bromii (a keystone degrader) and subsequently supports all three major SCFAs; strongly increases butyrate
- Pectin: fermented rapidly, primarily produces acetate and propionate
The modern Western diet averages 15-20 g of fiber per day; traditional forager diets average 100+ g per day.
This fiber gap is probably the single most important factor in the low SCFA production seen in industrialized populations.
2. Gut transit time:
Slower transit allows more complete fermentation and higher SCFA extraction.
Faster transit reduces SCFA production and increases the proportion of unfermented fiber delivered to the distal colon.
3. Microbiome composition:
Without the specific bacterial communities required for each fermentation pathway, even adequate fiber intake fails to produce normal SCFA output.
Antibiotic-driven depletion of Faecalibacterium prausnitzii and Roseburia spp. reduces butyrate even on a high-fiber diet.
4. When the fiber supply runs out:
When fermentable carbohydrate is exhausted, bacteria shift to amino acid catabolism.
This increases BCFAs, phenols, indoles, and ammonia.
This shift is why high-protein, low-fiber diets are associated with colonic dysbiosis even when protein quality is adequate: the protein that reaches the colon becomes substrate for putrefactive rather than fermentative microbiota.
What To Stay Away From
- Broad-spectrum antibiotics without concurrent prebiotic or probiotic support: every course of antibiotics preferentially depletes anaerobic butyrate producers (Firmicutes) over aerobic bacteria; a single course can reduce Faecalibacterium prausnitzii by orders of magnitude and butyrate output for months; this is not an argument against antibiotics when genuinely needed, but it is an argument for strategic dietary fiber intake before, during, and after
- Chronic low-fiber diet below 20g/day in adults: the most reliable way to chronically reduce SCFA production, promote BCFA production from protein fermentation, and deplete butyrate-producing bacteria; the threshold is not binary, but the evidence for SCFA production improvements scales with fiber intake from approximately 20g upward
- Assuming protein fermentation is benign: elevated BCFAs (isobutyrate, isovalerate, 2-methylbutyrate) in feces signal that bacteria have run out of fermentable carbohydrate and have shifted to protein catabolism; the co-metabolites of protein fermentation (branched-chain fatty acids, phenols, indoles, ammonia) are not neutral at high concentrations; high BCFA/SCFA ratios are consistently associated with aging, dysbiosis, and chronic disease, not with health
- Using oral sodium butyrate at standard supplement doses and expecting significant colonic effects: standard oral sodium butyrate capsules (150-600 mg/day) are absorbed largely in the upper GI tract and do not meaningfully raise colonic butyrate concentrations; colon-targeted microencapsulated formulations improve but do not fully solve this; raising colonic butyrate through diet (fiber, resistant starch) or via rectal administration is more reliably effective for conditions where the target tissue is the distal colon
- Conflating fecal SCFA levels with portal or peripheral SCFA levels: these are fundamentally different pools reflecting different physiological processes; high fecal SCFAs in some disease states may reflect impaired colonic absorption, not increased production; low fecal SCFAs may reflect increased colonic extraction (which would be metabolically beneficial); fecal SCFA measurement without the broader context of the GI map and clinical picture can be misleading
Testing
Comprehensive Stool Analysis (GI-MAP or equivalent):
Quantifies levels of the major butyrate-producing bacteria (Faecalibacterium prausnitzii, Roseburia, Eubacterium, Clostridium butyrate producers) and propionate producers (Bacteroides, Prevotella).
Some versions directly measure fecal acetate, propionate, and butyrate concentrations.
Low levels of butyrate-producing Firmicutes with proportionally elevated Proteobacteria is the dysbiosis pattern most strongly linked to SCFA deficiency.
Organic Acids Test (OAT):
Urine organic acids reflect the metabolic outputs of gut bacteria.
Elevated indican (from tryptophan) and para-hydroxyphenylacetate indicate protein fermentation dominating over carbohydrate fermentation.
Elevated D-arabinitol can suggest yeast overgrowth secondary to SCFA-deficient dysbiosis.
These markers indirectly reflect a shift from straight-chain SCFA to BCFA production.
Fecal calprotectin:
Fecal calprotectin correlates with active mucosal inflammation.
In IBD patients, calprotectin correlates with SCFA profiles, making it a useful indirect marker of the inflammatory consequences of SCFA depletion.
Normal: less than 50 µg/g; borderline: 50-200 µg/g; elevated: above 200 µg/g.
Comprehensive blood panel including fasting glucose, insulin, HbA1c, triglycerides, lipid panel:
Propionate and butyrate both modulate hepatic gluconeogenesis, triglyceride synthesis, and insulin sensitivity.
These metabolic markers are the clinical readout of chronic SCFA biology in the liver.
Elevated fasting glucose and insulin resistance in the absence of other explanation should prompt assessment of the gut microbiome as a contributing factor.
Mechanisms Of Action
Simple:
- SCFAs are the chemical messages your gut bacteria send to your body after they eat the fiber in your food; there are three big ones (acetate, propionate, butyrate) that each do different things: acetate circulates in your blood and reaches your brain and fat tissue, propionate mostly goes to your liver where it regulates blood sugar, and butyrate mostly fuels the cells lining your colon.
- The gut-brain connection that regulates appetite runs partly on propionate: it stimulates the small intestinal cells to make glucose in the gut wall, portal vein sensors detect that glucose, signal the brain through nerves, and you feel less hungry; this is a direct neural pathway from what your bacteria eat to how full you feel.
- Branched-chain SCFAs (isobutyrate, isovalerate, 2-methylbutyrate) are a sign that something has gone wrong: they form when your gut bacteria run out of fiber to ferment and switch to fermenting protein instead; unlike the regular SCFAs from fiber fermentation, protein fermentation also produces ammonia, phenols, and other compounds that can damage the colon lining, which is why a low-fiber high-protein diet over time is hard on your gut even if the protein is high quality.
- Your microbiome produces SCFAs through an assembly line involving many species cooperating: some bacteria break down fiber into acetate and hydrogen gas, other bacteria consume the hydrogen and turn it into more acetate (preventing H2 from building up and stopping fermentation), and butyrate producers use that acetate as raw material to make butyrate; this is why antibiotics can drop your butyrate output even if you eat plenty of fiber, because they remove key links in the chain.
- Most cells sense SCFAs through specific receptors on their surface (GPR41, GPR43, GPR109A), each with its own preferred SCFA and its own job; GPR43 is on immune cells and responds to acetate and propionate to regulate inflammation; GPR41 is on the cells that secrete GLP-1 and on the neurons of the gut and responds to propionate; GPR109A is on colon cells and macrophages and responds specifically to butyrate to suppress inflammation and support barrier function.
Advanced:
- The Wood-Ljungdahl pathway and H2 homeostasis as a community regulatory mechanism: Colonic fermentation generates substantial H2 gas as a byproduct of NADH reoxidation during anaerobic fermentation. H2 accumulation inhibits fermentation thermodynamically by making the NADH/NAD+ ratio unfavorable. Acetogenic bacteria (primarily Blautia hydrogentrophicus and related species) use the Wood-Ljungdahl pathway to reduce two molecules of CO2 to acetate using 4 H2 as electron donor, functioning as H2 sinks that maintain the thermodynamic favorability of the entire fermentation network. This means that depletion of acetogens (by antibiotics or dietary changes) indirectly reduces total butyrate output by allowing H2 to accumulate and inhibit butyrate-producing Firmicutes upstream. The degree of H2 quenching also determines whether archaea (Methanobrevibacter smithii, via methanogenesis: 4 H2 + CO2 → CH4 + 2 H2O) or acetogens dominate this niche, which influences the acetate pool available for cross-feeding to butyrate producers. High methane producers have less acetate available for butyrate synthesis, potentially explaining some of the association between high methanogen abundance and constipation-type IBS phenotypes where butyrate production is reduced. R
- Propionate's dual role as both gluconeogenic substrate and gluconeogenesis suppressor via GPR43/AMPK: Propionate is converted to propionyl-CoA → methylmalonyl-CoA (requiring vitamin B12) → succinyl-CoA → malate/OAA → phosphoenolpyruvate (PEP) → glucose, contributing approximately 50% of the substrate for hepatic gluconeogenesis. Simultaneously, propionate binding to GPR43 on hepatocytes triggers Gαq-mediated Ca2+ release, activating CaMKKβ, which phosphorylates and activates AMPK. Phosphorylated AMPK inhibits G6Pase and PEPCK transcription via CREB and other transcription factors, reducing gluconeogenic gene expression. The net hepatic effect is therefore determined by the balance between propionate's role as a gluconeogenic substrate (promoting glucose production) and its GPR43/AMPK signaling (suppressing gluconeogenic enzyme expression). At physiological portal propionate concentrations, the signaling effect appears to dominate, producing net gluconeogenesis suppression and improved hepatic insulin sensitivity. This is mechanistically distinct from the action of metformin (which also activates AMPK) but uses the same downstream pathway, explaining why gut microbiome-based strategies that increase propionate can mimic some metabolic effects of biguanide drugs. R R
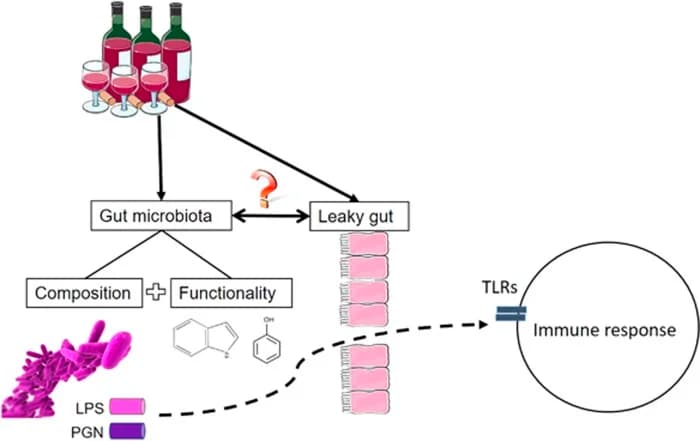
- BCFA production as a proxy for distal colonic protein fermentation and proteolytic dysbiosis: When fermentable carbohydrate is exhausted in the distal colon, bacteria ferment amino acids via the Stickland reaction and related pathways. Leucine → alpha-ketoisocaproate → isovaleryl-CoA → isovalerate; valine → isobutyrate; isoleucine → 2-methylbutyrate. The fecal SCFA/BCFA ratio (total straight-chain SCFAs divided by total BCFAs) serves as a semi-quantitative index of carbohydrate versus protein fermentation. High total fecal SCFA concentrations strongly correlate with high butyrate proportions and low BCFA proportions, consistent with active fiber fermentation. Low total SCFA concentrations correlate with high BCFA proportions, consistent with proteolytic fermentation. The co-fermentation products of protein catabolism beyond BCFAs include: phenol (from tyrosine and phenylalanine), p-cresol (from tyrosine), indole and skatole (from tryptophan), hydrogen sulfide (from cysteine and methionine), and ammonia (from all amino acids). At high concentrations, these compounds damage colonocyte DNA, compromise tight junctions, and activate TLR4 signaling via LPS amplification. The BCFAs themselves serve as the most clinically accessible marker of this pathological shift because they are measurable in stool analysis and BCFA elevation is therefore a surrogate for the full proteolytic dysbiosis output. R
More Research
- Acetate, propionate, and butyrate collectively account for approximately 95% of all SCFAs produced in the human colon; the molar ratio is approximately 60:20:20 in fecal content but shifts dramatically in portal blood (propionate is nearly depleted by first-pass hepatic extraction) and peripheral blood (acetate dominates at 91:5:4 molar ratio), reflecting the completely different tissue exposures to each SCFA despite sharing a colonic origin. R
- SCFA receptor pharmacology distinguishes the three major SCFAs: acetate preferentially activates GPR43; propionate activates both GPR43 and GPR41 with the highest receptor affinity of any natural SCFA; butyrate preferentially activates GPR109A and shows greatest HDAC inhibitory potency; valerate and BCFAs activate GPR41 with lower potency; these differential receptor affinities explain why the three SCFAs produce distinct rather than redundant physiological effects despite being structurally related. R
- Propionate suppresses hepatic gluconeogenesis via GPR43/CaMKKβ/AMPK signaling, downregulating G6Pase and PEPCK transcription; siRNA knockdown of GPR43 in HepG2 hepatocytes prevents propionate's AMPK phosphorylation and abrogates its gluconeogenesis-suppressive effect, establishing the mechanistic necessity of this receptor; this propionate-AMPK axis suggests that gut microbiome-based strategies for metabolic disease may work partly through the same pathway as biguanide drugs like metformin. R
- Branched-chain SCFAs (isobutyrate, isovalerate, 2-methylbutyrate) are produced from fermentation of branched-chain amino acids (valine, leucine, isoleucine) rather than dietary fiber; elevated fecal BCFAs indicate that bacteria have exhausted fermentable carbohydrate and switched to protein fermentation; the fecal SCFA/BCFA ratio increases with higher fiber intake and decreases with aging, high-protein diets, and intestinal dysbiosis; BCFAs and their co-metabolites (phenols, indoles, ammonia) damage colonic epithelium at high concentrations, making the BCFA proportion a clinically relevant marker of fermentation quality. R
- Isovalerate at physiological concentrations (3-5 mM) enhances intestinal epithelial barrier function through mechanisms similar to butyrate, including tight junction upregulation, possibly via HDAC inhibition; this finding challenges the view that all BCFAs are uniformly detrimental and suggests dose-dependent and context-dependent effects that parallel the "butyrate paradox" (beneficial at low concentrations in normal tissue, potentially harmful at high concentrations from dysbiotic protein fermentation).
- Valproate (valproic acid), the pharmaceutical anticonvulsant and mood stabilizer, is a short-chain fatty acid derivative of valerate (2-propylvaleric acid) whose therapeutic mechanism depends substantially on HDAC inhibition; this pharmacological use of an SCFA-related molecule as an HDAC inhibitor for neurological and psychiatric conditions reflects the broader biology of SCFAs as endogenous epigenetic modulators, with the pharmaceutical version providing sustained HDAC inhibition at doses far exceeding what gut fermentation produces.
- The cross-feeding network required for butyrate synthesis requires multiple species working in sequence: primary fiber degraders (Bacteroides, Ruminococcus) produce acetate and H2; acetogens (Blautia, Ruminococcus hydrogenotrophicus) quench H2 and produce more acetate; butyrate producers (Roseburia, Faecalibacterium) use acetate as the CoA donor for butyrate synthesis via butyryl-CoA:acetate CoA transferase; disrupting any node reduces butyrate output even if butyrate-producing species are still present, which explains why a high-fiber diet alone may not fully restore butyrate production after antibiotic-induced dysbiosis has depleted the acetate producers and H2 utilizers as well. R
- The inulin-propionate ester, a colon-targeted propionate delivery system given to overweight human subjects, significantly increased postprandial GLP-1 and PYY concentrations, reduced calorie intake at an ad libitum buffet meal, and after 24 weeks of supplementation reduced weight gain versus control; this human clinical evidence for propionate's satiety and metabolic effects through intestinal gluconeogenesis and gut hormone signaling provides the strongest direct evidence that the propionate-appetite axis operates in humans, not just rodents. R
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Spore-Based Probiotics
1 cap with food
L-Glutamine
5g 2x/day on empty stomach
Butyrate
300mg 2x/day with meals