Butyrate Enemas: What They Are, How They Work, And What The Evidence Actually Shows
By Jacob Gordon, INHC, FMT-CThis article contains affiliate links. As an Amazon Associate, MyBioHack earns from qualifying purchases at no extra cost to you. We only link products we research and stand behind.
Butyrate is a four-carbon short-chain fatty acid that serves as the primary fuel for colonocytes and one of the most important signaling molecules in the lower gut.
In this post, we will discuss what butyrate is and where it comes from, why the colon needs it topically when oral delivery fails to reach the distal bowel, what the mechanistic evidence says, what the clinical trial evidence actually shows for ulcerative colitis, diversion colitis, radiation proctitis, and pouchitis, how to prepare and administer a butyrate enema, and what the honest limitations of this approach are.

What Butyrate Is And Where It Comes From
Butyrate (butyric acid, C4H8O2) is a four-carbon short-chain fatty acid (SCFA) produced almost exclusively by bacterial fermentation of dietary fiber in the colon.
It is not meaningfully absorbed from food in intact form.
The butyrate you eat in butter or cheese is absorbed in the small intestine long before it reaches the colon.
The butyrate your colon actually uses is made on-site by specific anaerobic bacteria that ferment fiber residue that survived the small intestine.
The primary butyrate-producing bacteria are from the Firmicutes phylum, specifically genera within Clostridia class IV and XIVa: R
- Faecalibacterium prausnitzii (the most abundant single butyrate producer in a healthy human colon)
- Roseburia intestinalis
- Butyrivibrio fibrisolvens
- Eubacterium hallii
- Clostridium butyricum
Acetate and propionate (the other two major SCFAs) are produced more broadly, but butyrate production is concentrated in these specific anaerobic species that are also the most vulnerable to depletion by antibiotics, inflammation, low-fiber diets, and dysbiosis.
Both Faecalibacterium prausnitzii and Roseburia hominis are consistently and significantly reduced in active ulcerative colitis compared to healthy controls, with both species showing an inverse correlation with disease activity score. R
The human colon normally contains butyrate at luminal concentrations of approximately 10-20 mM in the proximal colon and lower concentrations in the distal colon, where fermentation is less active. R
Why The Colon Depends On Luminal Butyrate
Colonocytes are unusual cells: they prefer to burn butyrate over glucose.
Butyrate provides approximately 70% of the energy requirements of colonocytes, with the remainder coming from glutamine and glucose. R
This energy comes through a specific pathway: butyrate enters colonocytes via monocarboxylate transporter 1 (MCT1/SLC16A1) and sodium-coupled monocarboxylate transporter 1 (SMCT1/SLC5A8) at the apical (luminal) membrane, enters the mitochondria, is oxidized to acetyl-CoA via beta-oxidation, and enters the Krebs cycle producing NADH and ultimately ATP. R
MCT1 is a proton-coupled transporter and the major route under normal dietary conditions when luminal butyrate concentrations are high.
SMCT1 is a sodium-coupled high-affinity transporter that plays a critical role when luminal butyrate concentrations are low, such as during dysbiosis or low-fiber intake.
Both MCT1 and SMCT1 are downregulated in active ulcerative colitis and in colorectal cancer, which creates a vicious circle: inflammation reduces the very transporters needed to import the fuel that would resolve it. R
This dependency has a structural consequence: colonocytes consume most of the butyrate delivered luminally, leaving very little to enter portal circulation.
The liver sees almost none of it under normal conditions.
This is why measuring serum butyrate tells you almost nothing about colonic butyrate availability.
The near-complete oxidation of butyrate by colonocytes also serves a second function: it depletes local oxygen in the colonic epithelium, stabilizing HIF-1alpha (hypoxia inducible factor 1-alpha), which in turn drives expression of tight junction proteins and epithelial barrier genes.
The colon operates at a level of physiological hypoxia maintained partly by the metabolic activity of butyrate oxidation.
When butyrate is depleted (by dysbiosis, antibiotics, or diversion of the fecal stream), colonocytes shift toward glucose as their energy source.
This shifts the redox environment, reduces HIF-1alpha-driven barrier gene expression, compromises tight junctions, and allows the luminal environment to become more oxygenated, which further disrupts the anaerobic microbiome that was producing the butyrate in the first place.
This feedback spiral is mechanistically central to understanding why diversion colitis, chronic UC, and radiation proctitis all share a butyrate-deficient phenotype despite different etiologies. R
The Warburg-Like Paradox In Cancer Cells vs. Normal Colonocytes
Butyrate behaves differently in normal colonocytes versus cancer cells, a phenomenon called the butyrate paradox. R
In normal colonocytes, butyrate is rapidly oxidized as a fuel.
It does not accumulate intracellularly.
Because it is metabolized, it does not reach nuclear concentrations high enough to significantly inhibit histone deacetylase (HDAC) enzymes.
Normal colonocytes are therefore stimulated, not inhibited, by butyrate.
In cancer cells, glucose replaces butyrate as the primary energy source (the Warburg effect).
Butyrate is taken up but not efficiently burned.
It accumulates in the cytoplasm and nucleus.
At high intranuclear concentrations, butyrate becomes a potent HDAC inhibitor, causing histone hyperacetylation, altered gene expression, reduced proliferation, and apoptosis.
This is why butyrate exerts apparently opposite effects in the same tissue depending on the metabolic state of the cell receiving it.
It is also why butyrate has attracted interest as an epigenetic anticancer agent while simultaneously being the primary survival fuel for normal colonocytes. R
Understanding this paradox matters for the clinical context of butyrate enemas: the doses used in colitis enemas (40-100 mM) are physiological replacement doses aimed at restoring the energy and signaling environment of normal colonocytes, not pharmacological HDAC inhibition.
Why Oral Butyrate Often Doesn't Reach The Distal Colon
Oral butyrate, even in encapsulated or microencapsulated form, faces a significant challenge: the small intestine absorbs much of it before it reaches the colon.
Plain sodium butyrate capsules or sachets are absorbed rapidly in the upper GI tract.
They never reach the descending colon or rectum in meaningful concentrations.
Microencapsulated sodium butyrate (lipid matrix, pH-sensitive, or time-release coatings) was developed specifically to deliver butyrate to the colon.
These formulations improve but do not fully solve the problem of ensuring meaningful distal colonic concentrations.
The rectum and sigmoid colon, which are the primary sites of distal ulcerative colitis (proctitis, proctosigmoiditis), are paradoxically the hardest to reach with oral formulations because they are farthest from where absorption occurs and because fermentation is lowest in the left colon.
This is the mechanistic rationale for rectal administration: bypass the small intestine entirely, deliver butyrate directly to the inflamed distal mucosa at physiological or supraphysiological concentrations, and allow colonocytes to take it up immediately via their apical transporters. R
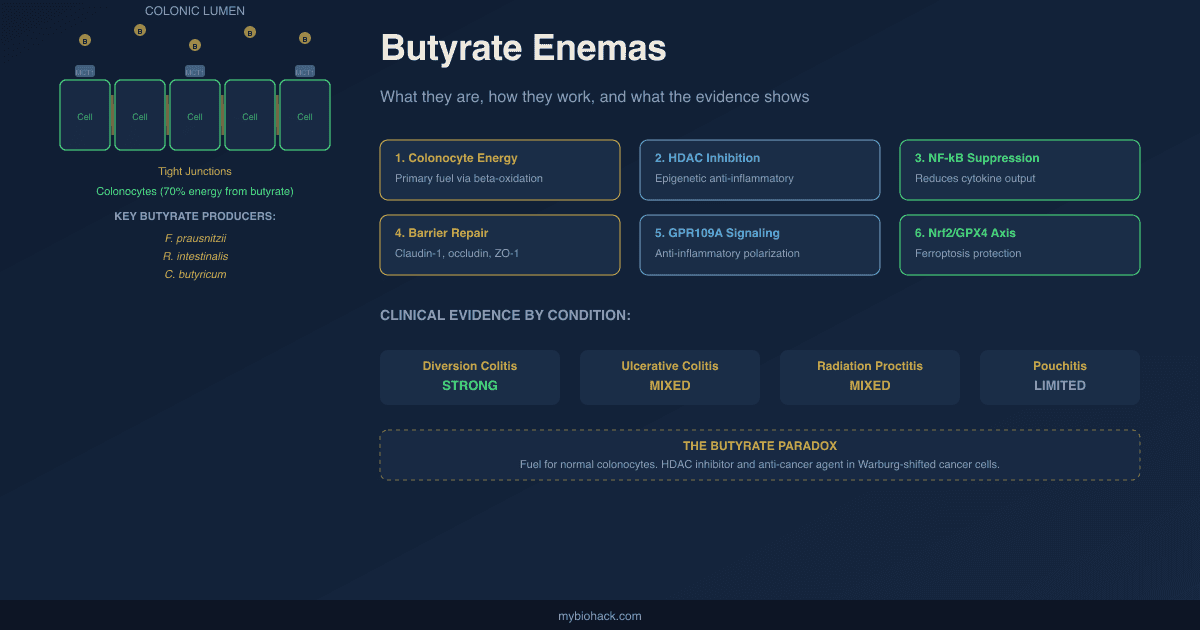
The Mechanisms Of Rectal Butyrate: More Than Just Energy
Delivered rectally, butyrate acts through at least five distinct mechanisms:
1. Colonocyte energy supply:
The most direct and most mechanistically clear function.
Inflamed colonocytes in UC and diversion colitis show impaired butyrate oxidation, contributing to a cellular energy deficit.
Restoring luminal butyrate supplies the substrate for mitochondrial oxidative phosphorylation, supporting epithelial repair and tight junction maintenance.
2. HDAC inhibition and gene expression modulation:
When colonocytes are inflamed or damaged, their mitochondrial oxidative capacity is reduced.
Butyrate that is not fully oxidized accumulates and inhibits nuclear HDACs.
This shifts the chromatin state toward greater histone acetylation, upregulating anti-inflammatory genes.
HDAC inhibition suppresses the transcription of pro-inflammatory cytokines (IL-6, TNF-alpha, IFN-gamma, IL-8) and upregulates anti-inflammatory mediators including IL-10. R R
3. NF-kB suppression:
Butyrate directly reduces nuclear factor kappa B (NF-kB) activation in colonocytes and in lamina propria macrophages. R
NF-kB is the master transcription factor driving inflammatory cytokine production in IBD.
This suppression occurs through multiple mechanisms: HDAC inhibition preventing p65 nuclear translocation, GPR109A signaling, and direct inhibition of IKK (IkB kinase) activity.
4. Tight junction restoration and epithelial barrier repair:
Butyrate induces expression of tight junction proteins including claudin-1, occludin, and ZO-1. R
One key mechanism is HDAC inhibition at the IL-10RA (IL-10 receptor alpha) gene promoter, increasing IL-10 receptor expression on colonocytes.
This enables endogenous IL-10 to signal more effectively, which represses the permeability-promoting tight junction protein claudin-2 and restores barrier function. R
5. GPR109A and GPR41 signaling:
Butyrate is a ligand for GPR109A (also the niacin receptor, HCAR2), expressed on colonocytes, macrophages, and dendritic cells. R
GPR109A activation in immune cells promotes anti-inflammatory polarization, Treg induction, and IL-10 production.
GPR41 (FFAR3) activation promotes IgA secretion in the large intestine, supporting mucosal immune homeostasis. R
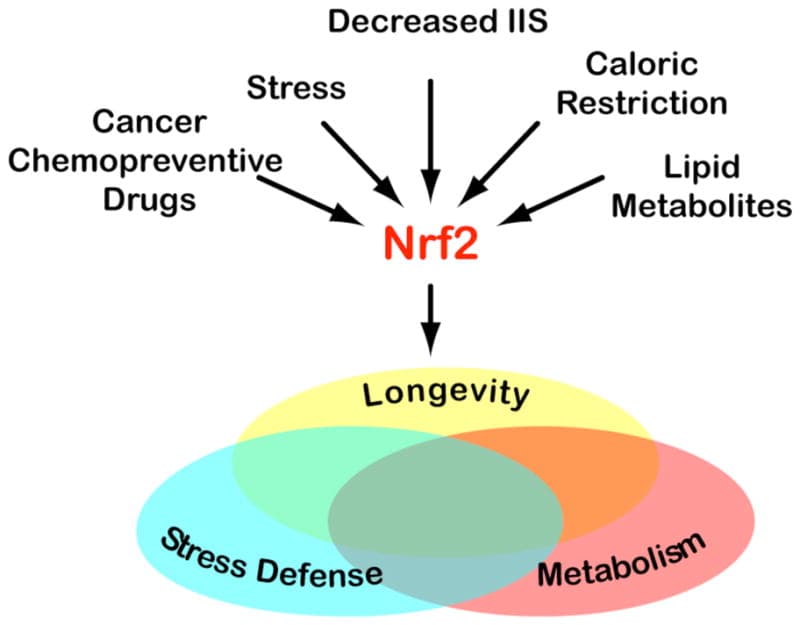
6. Nrf2/GPX4 pathway and ferroptosis protection:
Emerging research shows that butyrate activates Nrf2 (nuclear factor erythroid 2-related factor 2) and upregulates GPX4 (glutathione peroxidase 4), the master regulator of ferroptosis resistance.
In UC, ferroptosis (iron-mediated lipid peroxide-driven cell death) is a contributor to colonocyte death.
Butyrate's activation of the Nrf2/GPX4 axis inhibits ferroptosis in inflamed colonocytes and reduces mitochondrial damage. R
What Conditions Have Been Studied
Butyrate enemas have been formally studied in:
- Distal ulcerative colitis (proctitis, proctosigmoiditis, left-sided UC)
- Diversion colitis (inflammation of the bypassed colon after colostomy or ileostomy)
- Radiation proctitis (acute and chronic)
- Chronic pouchitis after ileal pouch-anal anastomosis (IPAA)
Most trials are small, use varied concentrations and volumes, and have inconsistent blinding, which makes pooling data difficult.
The 2021 systematic review published in Digestion searched PubMed, Scopus, Web of Science, and Cochrane databases, identified eight RCTs involving 227 UC patients, and concluded that the current evidence does not support the application of butyrate enemas in UC as a standalone therapy. R
This is the honest clinical summary: promising mechanistic rationale, mixed clinical evidence.
The post proceeds condition by condition because the evidence profile is genuinely different across these indications.
Ulcerative Colitis: What The Clinical Evidence Shows
The most-cited early positive trial is from Scheppach et al. (1992), published in Gastroenterology.
Ten patients with distal UC who were unresponsive to or intolerant of standard therapy received sodium butyrate enemas at 100 mM for 2 weeks.
Stool frequency dropped from 4.7 to 2.1 per day, rectal bleeding stopped in 9 of 10 patients, and endoscopic and histological scores improved significantly. R
This was a positive single-blind crossover trial in a very small, treatment-refractory population.
Subsequent controlled trials have been less consistently positive.
A 1997 trial by Steinhart et al. in 38 patients with distal UC used 80 mM butyrate enemas nightly and found no significant difference from placebo: clinical improvement in 37% of butyrate patients versus 47% in the placebo group. R
The 2021 systematic review (8 RCTs, 227 UC patients) found only one study reporting significant differences in disease activity index between groups, with the majority of studies showing no significant difference in endoscopic or histological scores between butyrate and placebo.
Why the inconsistency?
Several factors explain the mixed results:
Dose and concentration have varied widely across trials (40-100 mM), and the optimal concentration is not established.
Volume has varied (60-200 mL), which determines how far proximally material reaches; 60 mL reaches the sigmoid, while 200 mL can reach the descending colon.
Frequency has varied (once nightly versus twice daily).
Some trials co-administered butyrate with other SCFAs (acetate and propionate), producing a mixed SCFA enema that mimics the natural luminal environment more closely than butyrate alone.
The SCFA mixture trials (butyrate 40 mM + propionate 30 mM + acetate 60 mM) have shown more consistent positive results in radiation proctitis than butyrate-only trials.
Treatment duration (2-6 weeks) may be insufficient to induce meaningful mucosal healing in established UC.
The patient populations studied have varied between active disease, remission maintenance, and refractory disease.
Current honest summary for UC:
Butyrate enemas show a mechanistic rationale and some clinical signal in treatment-refractory distal UC, particularly in small uncontrolled trials.
They appear safe and have no meaningful adverse event profile.
As monotherapy, the controlled evidence does not support their use as a primary or standalone treatment for active UC.
The most reasonable interpretation is that they may have a role as an adjunct to standard therapy (mesalazine enemas, corticosteroid enemas) in distal UC, particularly in patients with treatment-refractory disease or who cannot tolerate standard topical therapies.
Diversion Colitis: The Most Mechanistically Clear Indication
Diversion colitis is inflammation in the segment of colon or rectum that has been excluded from the fecal stream after a colostomy or ileostomy.
It is arguably the most mechanistically compelling indication for butyrate enemas because the pathogenesis is essentially a pure butyrate (and SCFA) deficiency state.
When the fecal stream is diverted, the excluded segment no longer receives fermentation products including butyrate from the microbiome.
The diverted mucosa becomes butyrate-starved.
Colonocytes shift toward glucose dependence, tight junctions weaken, oxygen levels rise in the excluded segment, and mucosal atrophy and inflammation follow.
Case series and small trials from the 1980s and 1990s (Harig et al., NEJM 1989) demonstrated that SCFA irrigation of the excluded segment reliably ameliorates diversion colitis, with mucosal healing observed both clinically and histologically.
These results have been replicated consistently, making diversion colitis the one indication where the mechanistic and clinical evidence most strongly align. R
The clinical approach is straightforward: sodium butyrate solution (typically 80-100 mM in normal saline) is instilled as a retention enema into the excluded bowel segment daily or twice daily.
Response is typically seen within 2-4 weeks.
Diversion colitis resolves after restoration of the fecal stream (surgical takedown), confirming that luminal nutrient deprivation is the primary driver.
Radiation Proctitis
Radiation proctitis is inflammation and mucosal injury of the rectum and distal colon caused by pelvic radiation, most commonly from prostate, cervical, or rectal cancer treatment.
Acute radiation proctitis occurs during or immediately after radiation and is characterized by mucosal inflammation, edema, rectal bleeding, urgency, and diarrhea.
Chronic radiation proctitis occurs months to years after radiation from progressive vascular injury, fibrosis, and mucosal atrophy with telangiectasia.
The rationale for butyrate enemas in radiation proctitis is the same as for diversion colitis: radiation destroys the mucosal microenvironment, depletes butyrate-producing bacteria, impairs colonocyte energy metabolism, and compromises the barrier.
SCFA mixture for radiation proctitis:
A 1999 randomized controlled trial (Vernia et al.) of 19 patients with chronic radiation proctitis compared mixed SCFA enemas (60 mM acetate, 30 mM propionate, 40 mM butyrate) versus placebo for 5 weeks.
SCFA-treated patients showed significantly fewer days of rectal bleeding, improved endoscopic score, and higher hemoglobin levels versus placebo. R
Butyrate-alone enemas for radiation proctitis:
A 1999 randomized double-blind crossover trial by Talley et al. in 12 patients with chronic radiation proctitis used butyrate alone (40 mM) twice daily for 2 weeks.
Symptom score improved from 5.5 to 3.5, but the change compared to placebo (4.5) was not statistically significant.
Histology was abnormal in 82% of placebo patients versus 55% of butyrate patients, but the difference was not significant.
Prevention of acute radiation proctitis:
A multicenter randomized trial (NABUREN study) of 166 prostate cancer patients allocated to rectal sodium butyrate 1g, 2g, or 4g daily or placebo during radiotherapy found no evidence of benefit for preventing acute radiation proctitis in any butyrate dose group. R
Honest summary for radiation proctitis:
The SCFA mixture enemas show more consistent positive results than butyrate-alone enemas, suggesting that the full physiological cocktail of SCFAs may be needed for meaningful mucosal restoration.
Butyrate-alone enemas show a histological trend toward benefit in chronic radiation proctitis but have not reached statistical significance in controlled trials.
Prevention of acute radiation proctitis with butyrate has not been demonstrated.
Pouchitis
Pouchitis is inflammation of the ileal pouch constructed after total proctocolectomy for UC or familial adenomatous polyposis.
Chronic pouchitis is difficult to treat and represents a significant source of morbidity for patients who have undergone J-pouch construction.
Diversion pouchitis (pouchitis in a pouch excluded from the fecal stream) closely mirrors diversion colitis in its pathogenesis and also responds to SCFA irrigation.
For conventional pouchitis (pouch in continuity with the fecal stream), the evidence for butyrate enemas is limited to small case series and a Mayo Clinic pilot study (Wischmeyer et al., 1993) showing modest symptomatic improvement with butyrate and glutamine suppositories.
Pouchitis management has largely moved toward manipulation of the microbiome (probiotics including VSL#3, antibiotics including ciprofloxacin and metronidazole, and FMT in research settings), with butyrate playing a minor adjunctive role if any.
How To Prepare And Administer A Butyrate Enema
This section addresses the practical "how" for those pursuing butyrate enemas therapeutically under appropriate clinical guidance.
Sodium butyrate source:
Sodium butyrate powder is available from supplement suppliers.
Use pharmaceutical or food-grade sodium butyrate, not industrial grade.
Most suppliers offer sodium butyrate in bulk powder or premeasured capsules.
Verify purity and source.
Concentration used in clinical trials:
Most positive trials used 80-100 mM (millimolar) solutions.
100 mM sodium butyrate = 11 g/L = approximately 1.1 g per 100 mL.
For a 60-100 mL enema, this translates to approximately 0.66-1.1 g of sodium butyrate per dose.
The dosage review literature supports 40-100 mM as the effective range with no toxicity at any tested dose. R
Preparation:
Dissolve sodium butyrate powder in sterile or distilled water, or physiological saline (0.9% NaCl).
The target pH should be approximately 7.0 (buffered saline provides this; plain water may require pH adjustment).
Butyrate in solution has a characteristic odor resembling rancid butter or parmesan cheese.
This is normal and harmless.
Use within 24 hours of preparation (or store refrigerated for up to 3 days; longer storage is not recommended for home preparations without preservatives).
Commercial premixed sodium butyrate enema solutions are available in Europe (particularly Italy, Poland) but are not widely sold as pharmacy products in the US, which is why most people prepare them from powder.
Volume:
60 mL delivers material to the sigmoid colon and rectum.
100-150 mL reaches the descending colon.
200 mL can potentially reach the splenic flexure (left-sided disease benefit).
Start with 60 mL if tolerance is unknown; the rectum is more sensitive in active inflammation and may not tolerate higher volumes.
Administration:
Administer at night, in the left lateral decumbent (Sims) position.
Use an enema bag or bulb syringe.
Insert the tip gently into the rectum (approximately 10 cm) and instill slowly over 1-2 minutes.
Remain lying down and retain the solution for as long as possible, ideally 30-60 minutes minimum.
Many people fall asleep and retain all night, which is fine.
Administer after a bowel movement to maximize retention time.
Duration:
Most positive clinical evidence used 2-6 weeks of nightly treatment.
For diversion colitis, treatment continues until surgical takedown (restoration of the fecal stream).
For UC adjunctive use, 4-8 weeks is a reasonable initial trial before reassessing.
For radiation proctitis, 3-5 weeks is consistent with the published protocols.
Mixed SCFA option:
For radiation proctitis and conditions where the full SCFA spectrum is desired, a mixed solution replicating the Vernia et al. protocol can be prepared:
- Sodium acetate: 60 mM (4.9 g/L)
- Sodium propionate: 30 mM (3.1 g/L)
- Sodium butyrate: 40 mM (4.4 g/L)
Dissolve in saline and administer as above.
What To Stay Away From
- Using butyrate enemas as monotherapy for active moderate-to-severe ulcerative colitis: the controlled clinical evidence does not support this; active UC should be managed with established therapies (5-ASA enemas/suppositories, topical corticosteroids, systemic therapy for more severe disease); butyrate enemas may have a role as an adjunct in treatment-refractory distal UC but replacing mesalazine or steroids with butyrate enemas for established disease is not evidence-based
- Assuming oral sodium butyrate supplementation at standard supplement doses (150-600 mg/day) delivers meaningful colonic concentrations: standard oral butyrate supplement doses are absorbed almost entirely in the small intestine and do not provide meaningful distal colonic delivery; the only forms of oral butyrate with evidence for colonic delivery are microencapsulated or lipid-matrix formulations specifically designed for colon targeting; if the goal is distal colonic effect, rectal administration is the only reliable route
- Expecting results within 24-48 hours: butyrate enemas work through metabolic and gene expression mechanisms that require days to weeks to produce meaningful mucosal changes; the positive clinical trials used 2-6 weeks of treatment; a single administration or a few days of treatment does not assess whether the approach will work
- Using butyrate enemas during an acute active flare without concurrent medical management in IBD: severely inflamed mucosa may have impaired butyrate uptake (MCT1 is downregulated in severe acute inflammation), reducing the effectiveness of luminal delivery; during a moderate-to-severe flare, systemic anti-inflammatory treatment takes priority and butyrate enemas serve as adjuncts at best
- Confusing butyrate enemas with coffee enemas or other non-evidence-based enema practices: butyrate enemas have a mechanistic rationale and some clinical evidence in specific conditions; they are not the same category as coffee enemas or hydrogen peroxide enemas, which have no evidence base and carry active harm risk; being specific about the distinction matters when discussing this with healthcare providers
Testing
Comprehensive Stool Analysis (GI-MAP or equivalent):
The most relevant upstream test.
Quantifies levels of butyrate-producing bacteria including Faecalibacterium prausnitzii, Roseburia, and Clostridium species.
Low levels of these organisms suggest inadequate endogenous butyrate production capacity.
Also quantifies fecal SCFA (some versions include butyrate, acetate, and propionate measurement directly), which can confirm whether luminal butyrate deficiency is present before proceeding with enema therapy.
Fecal Calprotectin:
Quantitative marker of intestinal inflammation.
Elevated in active UC, Crohn's, radiation proctitis, and pouchitis.
Used to document baseline disease activity and track response to therapy.
A falling calprotectin over a 4-6 week treatment course is an objective indicator of mucosal inflammation reduction.
Values above 150-200 µg/g indicate active inflammation; above 500 µg/g indicates severe mucosal inflammation.
Organic Acids Test (OAT):
Indirectly reflects microbial metabolite production including SCFAs.
Elevated indican, specific bacterial metabolites, and altered organic acid profiles suggest colonic dysbiosis and impaired butyrate production.
Not a direct measurement of colonic butyrate, but useful for characterizing the metabolic state of the gut ecosystem.
Colonoscopy with biopsy (if indicated):
Required for formal assessment of UC disease activity, diversion colitis severity, or radiation proctitis histology.
Not a test you order independently, but the clinical decision-making context for when butyrate enemas are being considered in diagnosed IBD should include a baseline endoscopic assessment of disease severity and distribution.
Disease limited to the rectum and sigmoid (distal disease) has the strongest rationale for rectal butyrate delivery.
More proximal disease requires oral or combined approaches.
Symptom tracking:
For self-monitored adjunctive use, a simple symptom diary tracking stool frequency, rectal bleeding (present/absent, mild/moderate/severe), urgency, and abdominal pain before and during a 4-6 week course provides a practical personal efficacy assessment.
Clinical trials use formal disease activity indices (Mayo Score for UC, PCDAI for Crohn's, RAD score for radiation proctitis); the relevant items from these scales can be self-tracked.
Mechanisms Of Action
Simple:
- The lining of your colon is almost entirely dependent on butyrate as its fuel; butyrate is made by gut bacteria that ferment fiber, and when those bacteria are wiped out by antibiotics, suppressed by dysbiosis, or excluded by surgical diversion, the colonic lining slowly starves and becomes inflamed; butyrate enemas deliver this fuel directly to the mucosa, bypassing the bacteria that would normally make it.
- In normal colon cells butyrate is burned as energy so fast that almost none of it reaches the nucleus; in inflamed or damaged cells that have impaired mitochondria, butyrate doesn't get burned and instead inhibits enzymes (HDACs) that would normally silence anti-inflammatory genes; this shifts gene expression toward healing and away from inflammation, which is why the same molecule acts as fuel in healthy tissue and as an anti-inflammatory epigenetic signal in damaged tissue.
- Butyrate also directly tightens the junctions between colon cells, making the barrier more intact, and signals macrophages and immune cells in the colon to be less inflammatory; this happens through receptors on the cell surface (GPR109A and GPR41) that recognize butyrate as a chemical message that the gut microbiome is functioning normally.
- Oral butyrate supplements don't reach the lower colon because they are absorbed in the small intestine; enemas bypass this problem by delivering butyrate directly to the rectum and sigmoid where distal UC and radiation proctitis occur.
- The evidence is honest here: butyrate enemas work well in diversion colitis (where the problem is clearly a fuel supply failure) and have shown benefit in some but not all trials for UC and radiation proctitis; they are adjuncts to standard care, not replacements for it.
Advanced:
- The HIF-1alpha-butyrate-anaerobiosis loop and colonocyte biology: Colonocytes maintain a state of physiological hypoxia at the mucosal surface through an oxygen-consuming metabolic process driven by butyrate. Butyrate enters via MCT1 and SMCT1, undergoes beta-oxidation to acetyl-CoA, enters the TCA cycle, and drives NADH production through OXPHOS, consuming local oxygen. This oxygen consumption stabilizes HIF-1alpha, which in normoxia is rapidly degraded by prolyl hydroxylase domain enzymes (PHDs). HIF-1alpha in colonocytes drives transcription of barrier-protective genes including occludin, CLDN1, and genes supporting the tight junction complex. When butyrate is absent (dysbiosis, diversion), colonocytes shift to aerobic glycolysis, oxygen consumption decreases, tissue oxygen rises, anaerobiosis in the lumen is lost, Enterobacteriaceae expand into the oxygen-enriched niche, and barrier genes dependent on HIF lose their transcriptional driver. This creates a mechanistically coherent chain from butyrate depletion to mucosal oxygen dysregulation to barrier failure to dysbiosis expansion. The therapeutic goal of butyrate enemas is partly to restart this physiological oxygen-consuming cycle at the mucosal surface. R
- HDAC inhibition, NF-kB, and the epigenetic basis of anti-inflammatory signaling: When inflamed colonocytes receive excess butyrate that cannot be fully oxidized (due to mitochondrial dysfunction in the inflammatory state), unmetabolized butyrate accumulates and inhibits class I and class II HDACs. HDAC inhibition at the IL-10RA promoter increases IL-10 receptor alpha expression, amplifying the cell's responsiveness to endogenous IL-10. IL-10 signaling through IL-10RA activates STAT3, which drives expression of barrier-forming tight junction proteins and directly represses claudin-2, the permeability-promoting tight junction isoform that is pathologically upregulated in IBD. Simultaneously, HDAC inhibition prevents deacetylation of histone H3 at NF-kB target gene promoters, impairing p65 access and reducing transcription of TNF-alpha, IL-6, IL-1beta, and IL-8. The net effect is a shift in colonocyte and macrophage gene expression from an inflammatory to a tolerogenic profile, driven epigenetically by excess butyrate that the cell could not metabolize. This context-dependence (beneficial in inflammation, neutral in health) makes butyrate unusual as a therapeutic molecule: its anti-inflammatory potency is highest precisely where inflammation has impaired the mitochondrial oxidation that would otherwise consume it. R
More Research
- Butyrate provides approximately 70% of colonocyte energy needs via mitochondrial beta-oxidation; its near-complete local consumption by normal colonocytes explains why systemic butyrate levels do not reflect colonic availability and why oral supplementation at standard doses fails to provide meaningful distal colonic delivery; this is validated by germ-free mice studies showing marked decreases in colonocyte NADH/NAD+ and ATP levels that are fully rescued by colonization with a butyrate-producing strain. R
- MCT1 (SLC16A1) and SMCT1 (SLC5A8) are the two apical-membrane transporters responsible for butyrate entry into colonocytes; both are downregulated in active ulcerative colitis and in colorectal cancer, creating a pathological feedback loop where inflammation reduces the import machinery for the very fuel that would suppress that inflammation; SMCT1 silencing by aberrant DNA hypermethylation is recognized as an early event in colon carcinogenesis. R R
- Roseburia hominis and Faecalibacterium prausnitzii, the two primary butyrate-producing bacteria of the Firmicutes phylum, are significantly reduced in UC patients compared to healthy controls (both p<0.0001), and both show an inverse correlation with disease activity score; fecal SCFAs are also significantly lower in active UC (p=0.014); this microbial depletion profile confirms the biological rationale for butyrate replacement therapy in UC dysbiosis. R
- A meta-analysis and systematic review of 11 studies (N=1180) confirmed that F. prausnitzii bacterial counts are significantly lower in IBD patients versus healthy controls (standardized mean difference -0.94, 95% CI -1.07 to -0.80), further validating butyrate-producing bacterial depletion as a consistent feature of IBD pathology. R
- GPR109A, the primary butyrate-sensing GPCR on colonocytes and macrophages, also binds niacin and beta-hydroxybutyrate; it was identified as functioning as a tumor suppressor in colon because its SLC5A8-mediated transport of butyrate into colonocytes drives HDAC inhibition and cell cycle arrest in cancer cells; GPR109A expression is silenced in many colorectal cancers, linking butyrate signaling deficiency to carcinogenesis alongside the metabolic Warburg shift. R
- The 2021 systematic review of 8 RCTs (227 UC patients) using butyrate enemas concludes that current evidence does not support their standalone application in UC; the most important methodological limitations are small sample sizes, heterogeneous concentrations (40-100 mM) and volumes (60-200 mL), and short treatment durations (2-6 weeks), making it impossible to determine whether specific dosing protocols might show consistent benefit. R
- The early positive Scheppach 1992 Gastroenterology trial (10 patients, 100 mM sodium butyrate, 2 weeks, crossover design) found stool frequency fell from 4.7 to 2.1/day, rectal bleeding stopped in 9/10 patients, endoscopic score fell from 6.5 to 3.8, and histological inflammation decreased; the subsequent Steinhart 1997 controlled trial (38 patients, 80 mM, nightly, 6 weeks) found no significant difference from placebo (37% vs 47% improved); this divergence illustrates the dose, volume, and design-sensitivity of the literature. R R
- Diversion colitis is the clearest indication for butyrate enemas: the pathogenesis is essentially pure luminal SCFA deprivation from exclusion of the fecal stream, and SCFA irrigation reliably ameliorates the histological and clinical picture; this indication makes the physiological model of butyrate deficiency driving colitis most explicit, and its response to butyrate replacement is the strongest mechanistic validation of the broader hypothesis. R
- Mixed SCFA enemas (butyrate + propionate + acetate) have outperformed butyrate-alone enemas in radiation proctitis trials, suggesting that the natural luminal SCFA mixture is more effective than any single SCFA; the Vernia et al. 1999 RCT (19 patients) showed significant reduction in rectal bleeding days, improved endoscopic score, and higher hemoglobin with SCFA mixture versus placebo, while butyrate-alone trials in radiation proctitis have generally not reached statistical significance. R
- The multicenter NABUREN dose-finding phase 2 RCT (166 prostate cancer patients, four arms: sodium butyrate 1g, 2g, 4g daily or placebo during and 2 weeks after radiotherapy) found no evidence of efficacy for preventing acute radiation proctitis at any butyrate dose, contrasting with positive results from SCFA mixture studies in established chronic radiation proctitis; this suggests butyrate enemas may be insufficient for prophylaxis but may have a role in established post-radiation mucosal injury. R
- Butyrate's protection against ferroptosis in inflamed colonocytes via Nrf2/GPX4 upregulation is a recently characterized mechanism that links SCFA depletion in IBD to a specific cell death pathway; ferroptosis, characterized by iron accumulation and lipid peroxidation, is documented in UC mucosal biopsies, and butyrate's ability to inhibit this process by upregulating the Nrf2/GPX4 axis represents a mechanism distinct from its energy-supplying and HDAC-inhibiting functions. R
- A 2025 multi-center double-blind RCT (98 adults, mild-to-moderate active UC) tested microencapsulated sodium butyrate (MSB, 2×300 mg/day) as add-on to standard therapy for 8 weeks; primary endpoints included clinical improvement (≥3-point Total Mayo Score reduction), endoscopic improvement, and biochemical remission (fecal calprotectin ≤250 µg/g); this represents the most recent controlled trial of a colon-targeted oral butyrate formulation, with results demonstrating that colon-targeted oral delivery overcomes the bioavailability limitations of conventional oral butyrate at standard supplement doses. R
- No safety concerns have been identified with butyrate enemas at any concentration studied (40-100 mM); all adverse events reported are minor GI symptoms that also occur with placebo; dosing literature confirms that doses as high as 4400 mg/enema have been used with very good clinical outcomes and no side effects; the primary limitation is odor tolerance, not toxicity; this favorable safety profile makes butyrate enemas a reasonable adjunct to standard therapy in treatment-refractory distal colitis even in the absence of definitive efficacy evidence. R
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Spore-Based Probiotics
1 cap with food
L-Glutamine
5g 2x/day on empty stomach
Butyrate
300mg 2x/day with meals