The Gut-Skin Axis: How Postbiotics And SCFAs Reach The Follicle
By Jacob Gordon, INHC, FMT-CThis article contains affiliate links. As an Amazon Associate, MyBioHack earns from qualifying purchases at no extra cost to you. We only link products we research and stand behind.
The gut-skin axis is the bidirectional signaling network that links what happens inside your intestines to what shows up on your face.
In this post, we will discuss what the gut-skin axis actually is, how short-chain fatty acids and postbiotics signal to the skin, the immune and barrier mechanisms that carry the message, how those mechanisms drive acne, eczema, psoriasis, and rosacea, and what you can do about it.

Basics Of The Gut-Skin Axis
The gut-skin axis describes the constant chemical conversation between the gut microbiome and the skin. R
The two organs have more in common than most people realize.
Both are barrier organs that face the outside world.
Both are colonized by their own microbiome.
Both are heavily immune, with dense populations of resident immune cells sitting just under the surface.
The gut wins this relationship because it sets the tone for systemic immunity.
Roughly 70 percent of the body's immune tissue lives in the gut wall, so the microbes fermenting your food are effectively training the immune system that later patrols your skin. R
The conversation happens through metabolites, not nerves.
When gut bacteria ferment fiber and polyphenols, they release small molecules that enter the bloodstream and reach distant tissues, including the dermis and the hair follicle. R
The most important of these molecules are the Short-Chain Fatty Acids (SCFAs): acetate, propionate, and butyrate.
You can read the full breakdown of how each one is made in the post on short-chain fatty acids.
The second class of messengers are postbiotics, which are the non-living bacterial fragments, enzymes, cell-wall components, and metabolites that a microbiome leaves behind even after the bacteria themselves are gone.
Postbiotics include SCFAs, but also tryptophan-derived indoles, bacteriocins, exopolysaccharides, and structural pieces like peptidoglycan.
The clinical point is simple.
A healthy, diverse gut microbiome produces a stream of anti-inflammatory postbiotics that keep the skin calm.
A disrupted microbiome produces fewer of those calming signals and more inflammatory ones, and the skin is one of the first places that shift becomes visible. R
What Drives Gut-Skin Axis Dysfunction
The axis breaks down when the gut barrier and the gut microbiome stop working together.
Drivers of gut-skin axis dysfunction (not an exclusive list):
- Antibiotic and medication exposure (broad-spectrum antibiotics, chronic acid blockers, and repeated NSAID use that strips the gut lining) R
- Dysbiosis (loss of microbial diversity and depletion of SCFA-producing species) R
- High-glycemic, low-fiber Western diet (starves the bacteria that make butyrate and feeds the ones that make endotoxin) R
- Intestinal permeability (a leaky barrier that lets bacterial fragments cross into circulation)
- Small intestinal bacterial overgrowth (SIBO) (bacteria colonizing a part of the gut that should stay relatively sterile) R
The common endpoint of all of these is the same.
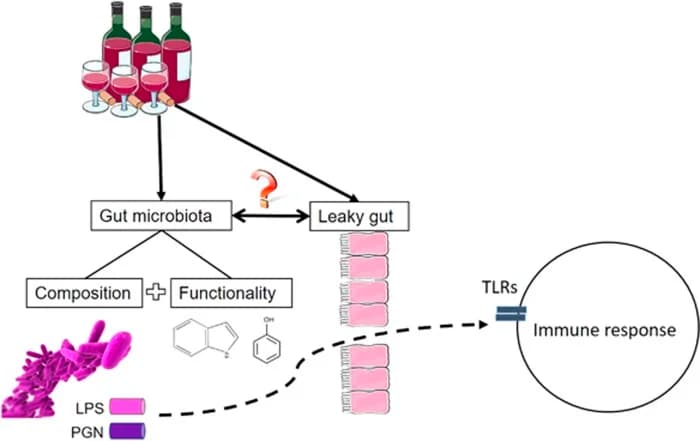
The intestinal barrier loosens, and bacterial products that should stay inside the gut start leaking into the portal circulation.
The most studied of these products is Lipopolysaccharide (LPS), the endotoxin shed from the outer wall of gram-negative bacteria.
When LPS crosses a permeable gut wall in small chronic amounts, it produces a state called metabolic endotoxemia, a low-grade systemic inflammation that Cani and colleagues first defined as a 2 to 3 fold rise in circulating LPS. R
LPS activates Toll-Like Receptor 4 (TLR4) on immune cells throughout the body, switching on NF-kB and a cascade of inflammatory cytokines that travel everywhere the blood goes, including the skin. R
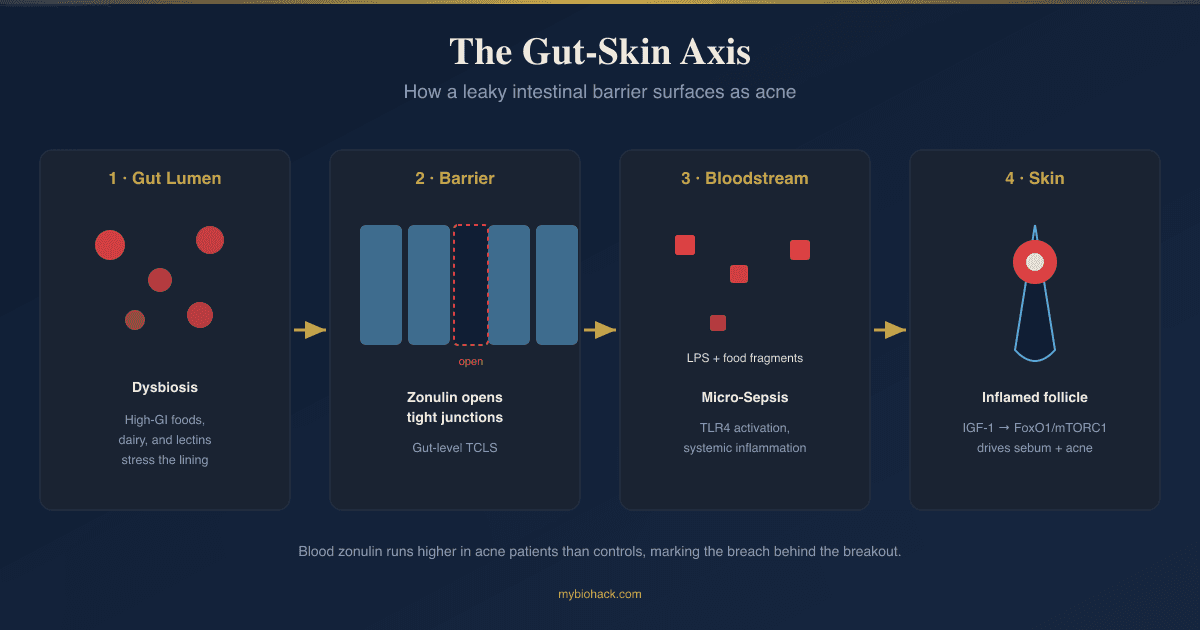
This is where the gut-skin axis connects directly to Junction Dysfunction.
In Jacob's framework, the gut epithelium is lined by the same glycocalyx that protects blood vessels, and when that layer degrades, the tight junctions underneath open.
Jacob calls the micro-level version of this leak Transient Capillary Leak Syndrome (TCLS), a term he coined for the transient, focal capillary and barrier leak that drives chronic illness.
TCLS of the gut epithelium leads to dysbiosis and to what Jacob calls Endotoxin Looping, where LPS recirculates through the portal vein and keeps the liver and systemic immune system in a state of low-grade activation.
That chronic sub-lethal activation is what Jacob calls Micro-Sepsis (MSS), his term for sub-lethal sepsis operating as a constant background process rather than an acute emergency.
You do not need to accept the full framework to use the practical takeaway.
Fixing the gut barrier lowers the endotoxin load reaching the skin, and lowering that load is one of the most reliable ways to calm inflammatory skin disease.
If the gut barrier piece is new to you, start with the posts on dysbiosis, intestinal permeability and acne, and how LPS causes endotoxemia.
How Postbiotics And SCFAs Reach The Skin
There are four main routes by which a gut metabolite ends up changing what happens at the follicle.

1. Direct circulation to the skin
SCFAs produced in the colon are absorbed into the portal blood and a fraction reaches the systemic circulation.
Butyrate that survives first-pass liver metabolism, along with acetate and propionate, can be measured in peripheral blood and reaches the dermis and sebaceous gland directly. R
Once there, SCFAs alter keratinocyte metabolism and differentiation, strengthening the skin barrier from the inside by changing mitochondrial energy production in the epidermis. R
2. SCFA receptor signaling
SCFAs are not just fuel, they are signaling molecules that bind specific G-protein coupled receptors.
Acetate and propionate preferentially activate GPR43 (FFAR2), while butyrate is the main ligand for GPR109A (the niacin receptor, also called HCA2). R
These receptors sit on neutrophils, macrophages, dendritic cells, and mast cells, which is exactly the population of immune cells that drives skin inflammation.
When SCFAs engage these receptors, they push immune cells toward a tolerant, anti-inflammatory phenotype instead of an aggressive one. R
3. Regulatory T cell induction
This is the single most important arm of the gut-skin axis.
Butyrate inhibits histone deacetylase, which increases acetylation at the Foxp3 promoter and drives naive T cells to become Regulatory T Cells (Tregs). R
Tregs are the immune system's brakes.
Tregs induced in the gut by butyrate do not stay in the gut.
They traffic out through the lymphatics and circulation and home to the skin, where they suppress the local inflammation behind eczema and psoriasis lesions. R

This is the mechanism in one sentence.
Fiber goes in, butyrate comes out, Tregs are born in the gut, and those Tregs migrate to the skin and turn down the fire.
You can read more about the T cell families involved in the post on T helper cell subsets and Tregs.
4. Aryl hydrocarbon receptor activation
The fourth route runs through tryptophan, not fiber.
Gut and skin bacteria metabolize the amino acid tryptophan into indole compounds, and those indoles are ligands for the Aryl Hydrocarbon Receptor (AhR). R
AhR is a transcription factor expressed in keratinocytes that controls epidermal differentiation, barrier-protein production, and the local immune set point.
When microbial indoles activate AhR in the skin, the barrier gets stronger and inflammation drops.
Indole-3-aldehyde, a tryptophan metabolite, is significantly lower in the skin of atopic dermatitis patients, and supplying it attenuates atopic-dermatitis-like inflammation through AhR. R
This same tryptophan-to-AhR pathway is disrupted in acne, where gut microbial handling of tryptophan shifts away from the protective indoles. R
The kynurenine side of tryptophan metabolism, driven by IDO1 during chronic inflammation, is covered in depth in the post on tryptophan, the kynurenine pathway, and the vagus nerve.
The Gut-Skin Axis And Overlapping Skin Conditions
Each of the four big inflammatory skin diseases maps onto a specific failure of the gut-skin axis.
Acne
Acne patients have a measurably distinct gut microbiome, with lower microbial diversity and depletion of beneficial Lactobacillus and Bifidobacterium. R
Gut dysbiosis reduces SCFA output and increases intestinal permeability, which lets LPS into circulation and activates the mTOR pathway that drives sebum production, lipogenesis, and keratinocyte proliferation inside the follicle. R
The follicle is where the gut-skin axis literally reaches the sebaceous gland, and the mechanistic chain from zonulin and bacterial fragments to breakouts is laid out in the post on acne and intestinal permeability.
The local cortisol axis inside the sebaceous gland that compounds this is covered in acne and rosacea as stress diseases.
Eczema (Atopic Dermatitis)
Atopic dermatitis is the cleanest example of the gut-skin axis in action.
Infants who later develop eczema show altered gut microbiomes and reduced SCFA production before the skin disease appears, and restoring SCFA and Treg signaling reduces lesion severity. R
The deficiency of indole-3-aldehyde and weakened AhR signaling in atopic skin is a direct postbiotic failure. R
The barrier and nerve drivers that sit downstream of this are covered in eczema beyond the barrier.
Psoriasis
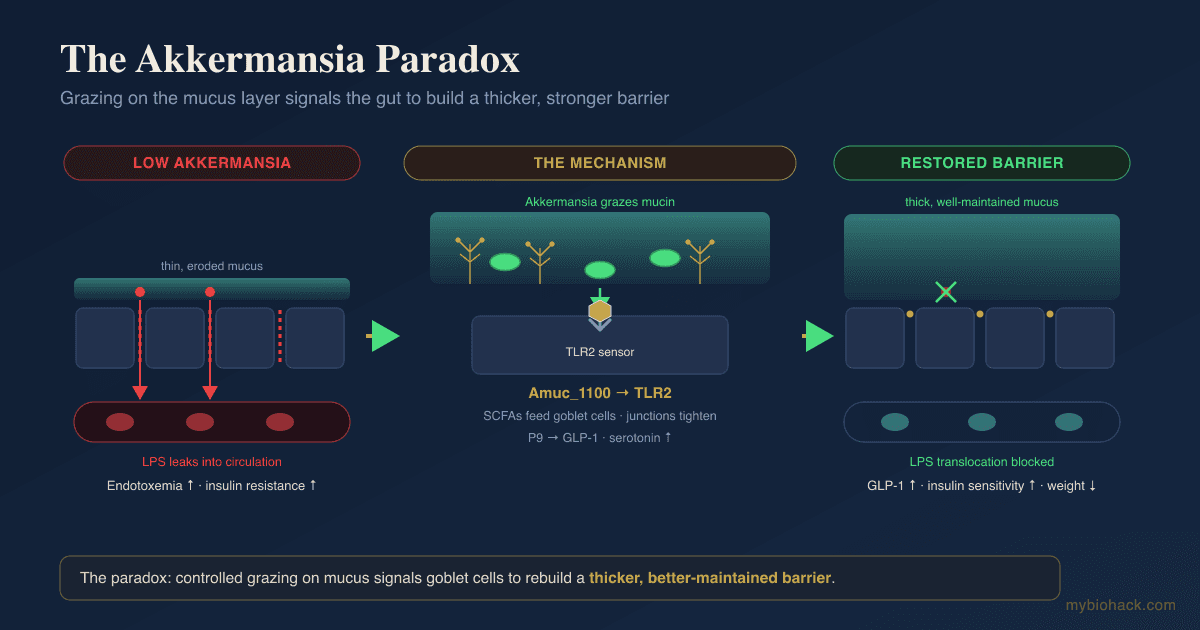
Psoriasis patients show a perturbed Firmicutes-to-Bacteroidetes ratio, depletion of SCFA producers, and a marked reduction in Akkermansia muciniphila and Faecalibacterium prausnitzii. R
Losing those SCFA producers removes the butyrate that would normally generate Tregs, which tips the immune balance toward the Th17 polarization that drives the psoriatic plaque. R
The neuroimmune side of plaque formation is covered in psoriasis as a neuroimmune disease, and a protocol-focused treatment is in how to naturally reverse psoriasis.
Rosacea
Rosacea has the strongest direct gut link of any skin condition.
SIBO is found 2 to 20 times more often in rosacea patients than in healthy controls, and in the landmark Parodi trial, eradicating SIBO with rifaximin cleared cutaneous lesions in 20 of 28 patients while placebo patients stayed the same or got worse. R
Most of those patients stayed clear for at least 9 months after eradication, which is a remarkable durability for a skin condition treated through the gut. R
Other overlaps
The gut-skin axis also overlaps with mast cell and histamine conditions, since SCFAs and Tregs both restrain mast cell reactivity.
Readers dealing with that layer should see the posts on mast cells, histamine intolerance, and the brain-skin axis.
How To Improve The Gut-Skin Axis
The logic of the protocol is to rebuild the microbes that make postbiotics, feed them the substrate they need, and patch the barrier so the postbiotics stay in and the endotoxin stays out.
1. Feed the SCFA producers with prebiotic fiber
You cannot make butyrate without substrate, so fermentable fiber comes first.
Resistant Starch: This is the most reliable butyrate-generating fiber, and the differences between the types matter, as covered in the post on resistant starch.
Partially Hydrolyzed Guar Gum: A gentle soluble fiber that raises butyrate without the bloating that inulin can cause in sensitive guts.
Inulin: A classic bifidogenic prebiotic, though start low if you have SIBO or histamine issues.
2. Add polyphenols as a second prebiotic class
Polyphenols are not just antioxidants, they act as prebiotics that favor SCFA producers and feed Akkermansia. R
Pomegranate Extract: The ellagitannins feed Akkermansia muciniphila, the species most depleted in psoriasis.
Green Tea Extract: EGCG shifts the microbiome toward SCFA producers and lowers gut inflammation.
Quercetin: A polyphenol that doubles as a mast cell stabilizer, useful when skin disease overlaps with histamine reactivity.
3. Repopulate with targeted probiotic strains
Strain specificity matters more than total count.
Lactobacillus rhamnosus GG: The most studied strain for atopic dermatitis, with the ProPAD trial showing reduced SCORAD severity in children. R
Lactobacillus paracasei: Shown to reduce skin inflammation and useful in acne, with the broader species guide in the Lactobacillus strains guide.
Bifidobacterium longum and Bifidobacterium breve: Core anti-inflammatory species depleted in acne and eczema, detailed in the Bifidobacteria strains guide.
4. Supplement the postbiotic directly
When the microbiome is too damaged to make enough butyrate, you can give the postbiotic itself.
Tributyrin or Sodium Butyrate: Oral butyrate raises colonic and systemic butyrate, and for distal disease the rationale for direct delivery is covered in butyrate enemas.
5. Patch the barrier
Lowering endotoxin translocation is what stops the systemic signal from reaching the skin.
L-Glutamine: The primary fuel for enterocytes and a tight-junction supporter.
Zinc Carnosine: Supports the gut lining and is separately important for skin, with the balance considerations in zinc, copper, and ceruloplasmin.
Vitamin D: Supports gut barrier integrity, Treg function, and skin immunity, with the cofactors that make it work in vitamin D is not one thing.
Omega-3 (DHA/EPA): Lowers systemic inflammatory tone and supports both gut and skin barriers.
6. Address SIBO and sluggish bile if present
If rosacea or bloating points to SIBO, the overgrowth has to be cleared before repopulation will hold. R
TUDCA: Supports bile flow, and sluggish bile is one of Jacob's mechanistic links between a congested liver and downstream gut overgrowth.
Digestive Bitters: Stimulate bile and stomach acid, both of which keep the upper gut from being colonized.
For practitioner-grade antimicrobial and biofilm protocols, a personalized plan through a consultation is the better route than guessing.
What To Stay Away From
These are the inputs that actively degrade the gut-skin axis.
What to avoid (not an exclusive list):
- Chronic broad-spectrum antibiotics when not clearly necessary, since they wipe out the SCFA producers you are trying to rebuild R
- Dietary emulsifiers (polysorbate-80 and carboxymethylcellulose in processed food, which thin the protective gut mucus layer)
- Excess alcohol (raises gut permeability and endotoxin translocation)
- High-glycemic and high-dairy diets (drive the mTOR and IGF-1 signaling that worsens acne) R
- NSAIDs used routinely (open the gut barrier and create new sensitivities, as covered in the post on NSAIDs and leaky gut)
- Over-sanitizing the skin (harsh surfactants and constant antibacterial washing strip the skin microbiome that makes its own protective AhR ligands) R
One caveat on resveratrol.
It is often recommended as a longevity polyphenol, but in Jacob's framework it induces IDO1, which shunts tryptophan away from the protective indole and AhR pathway, so it is not a first choice when the goal is repairing the gut-skin axis in a post-viral or chronically inflamed person.
Testing
The goal of testing is to confirm dysbiosis, measure barrier integrity, and quantify the inflammatory load reaching the skin.
Stool And Microbiome Panels
I use the Gut Zoomer (Vibrant Wellness) to assess microbial diversity, SCFA-producing species, zonulin, intestinal permeability markers, and SIBO indicators in one panel.
A PCR-based alternative is the GI-MAP (Diagnostic Solutions), which quantifies pathogens and commensals with strong reproducibility.
For a culture-and-microscopy approach, the Comprehensive Stool Analysis with Parasitology (Doctor's Data) is useful when parasites are suspected.
Microbial Metabolites
I use the Organic Acids Test (Mosaic Diagnostics) to assess bacterial and yeast metabolites in urine, which reflects how the gut microbiome is actually behaving rather than just who is present.
The Vibrant equivalent is the Cellular Zoomer, which covers organic acids, mitochondrial markers, and oxidative stress.
Inflammation And Immune Markers
I use the Immune Zoomer to assess systemic autoantibodies and immune reactivity when the skin disease has an autoimmune component such as psoriasis.
For the inflammatory load itself, the Cardio Zoomer includes hsCRP and metabolic inflammation markers, and elevated hsCRP above roughly 1 mg/L signals systemic inflammation worth chasing upstream. R
Food Reactivity
I use the Food Zoomer to assess IgG and IgA reactivity across 200-plus foods when an eczema or acne pattern tracks with diet.
Baseline And Nutrients
For a general baseline including liver function, CBC, and thyroid, I use the Foundation Zoomer, and for vitamin D, zinc, and copper status the Nutrient Zoomer.
Mechanisms Of Action
Simple:
- Gut bacteria turn fiber into butyrate, and butyrate trains immune cells in the gut to become calming Treg cells that then travel to the skin and switch off inflammation.
- When the gut barrier leaks, bacterial endotoxin gets into the blood and keeps the whole body, including the skin, in a low-grade state of inflammation.
- Skin bacteria turn tryptophan into indole signals that strengthen the skin barrier, and losing those signals weakens the skin.
Advanced:
- Butyrate-driven Treg induction via HDAC inhibition. Butyrate is a histone deacetylase inhibitor that increases histone H3 acetylation at the Foxp3 promoter and conserved non-coding sequence regions, driving extrathymic differentiation of Foxp3-positive Tregs in the colon. R These gut-induced Tregs traffic via the lymphatics and systemic circulation and home to peripheral tissue including skin, where they suppress effector T cell responses behind eczema and psoriasis. R
- SCFA receptor signaling on innate immune cells. SCFAs signal through GPR43 (FFAR2) and the butyrate-selective GPR109A (HCA2) on neutrophils, macrophages, dendritic cells, and mast cells, biasing them toward anti-inflammatory and tolerogenic phenotypes and dampening NF-kB-driven cytokine output. R
- Keratinocyte metabolic reprogramming. Gut-derived SCFAs reach the epidermis and modulate keratinocyte mitochondrial metabolism and differentiation, increasing production of structural barrier components and improving barrier integrity directly. R
- AhR activation by microbial tryptophan metabolites. Indole derivatives of microbial tryptophan catabolism act as AhR ligands in keratinocytes, upregulating barrier-protein expression and suppressing thymic stromal lymphopoietin and other pro-inflammatory mediators, with indole-3-aldehyde deficiency documented in atopic skin. R R
- Metabolic endotoxemia and TLR4. A permeable gut wall allows chronic low-level LPS translocation into portal and systemic circulation, where LPS engages TLR4 to activate NF-kB and the inflammasome, producing the sustained systemic cytokine tone that reaches the dermis and sebaceous gland. R R In Jacob's Junction Dysfunction framing, this is TCLS of the gut epithelium feeding Endotoxin Looping and Micro-Sepsis, which is his hypothesis for how barrier failure becomes a self-sustaining systemic process.
Genetics
FUT2
FUT2 encodes the alpha-1,2-fucosyltransferase that decorates the gut mucus layer with fucosylated sugars, which are food for Bifidobacteria.
Loss-of-function variants make a person a non-secretor, which is roughly 20 percent of the population.
rs601338 (and the linked rs602662) determine secretor status, and non-secretors carry significantly lower Bifidobacterium diversity, richness, and abundance, plus higher rates of inflammatory bowel disease. R
This matters for the gut-skin axis because fewer Bifidobacteria means a weaker postbiotic output reaching the skin.
FLG
FLG encodes filaggrin, the protein that aligns keratin filaments and generates the natural moisturizing factor that keeps the skin barrier sealed.
Loss-of-function mutations cause ichthyosis vulgaris and are the single strongest genetic predisposing factor for atopic dermatitis. R
R501X and 2282del4 are the two most common European loss-of-function variants, and carrying two of them is associated with eczema onset by age 2. R
A weak filaggrin barrier is exactly the situation where postbiotic AhR support matters most, because the skin needs all the barrier reinforcement it can get.
AHR
AHR encodes the aryl hydrocarbon receptor, the keratinocyte sensor for microbial tryptophan metabolites.
Variants and altered expression of AHR change how strongly the skin responds to its own protective indole ligands. R
People with weaker AhR signaling get less barrier benefit from the same microbial input, which is one reason identical diets produce different skin outcomes.
More Research
Akkermansia muciniphila sits at the center of several skin conditions because it both feeds on and feeds the mucus layer, and its depletion in psoriasis may be as important as the loss of butyrate producers. R
Fecal microbiota transplantation is the most aggressive way to reset a dysbiotic gut, and while skin-specific evidence is still early, the rationale and current data are in the post on fecal microbiota transplantation.
Postbiotic skincare is an emerging category where bacterial lysates and SCFAs are applied topically rather than taken orally, which bypasses the gut entirely but only addresses the local skin microbiome.
The skin has its own gut-independent tryptophan-AhR loop, since skin commensals also make indole ligands, so oral and topical strategies can be complementary rather than redundant. R
Timing of probiotic benefit appears delayed, since Treg induction and barrier remodeling take weeks, so the inflammatory skin trials that ran 8 to 12 weeks likely understate the ceiling of benefit. R
For biomarker tracking over time I use the Gut Zoomer to follow zonulin and SCFA-producer abundance, and the Cardio Zoomer to watch hsCRP fall as the barrier heals.
For readers who want the deeper mechanistic layer on how barrier and glycocalyx failure becomes systemic, see the posts on the glycocalyx and rebuilding the glycocalyx.
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Spore-Based Probiotics
1 cap with food
L-Glutamine
5g 2x/day on empty stomach
Butyrate
300mg 2x/day with meals