Acne And Rosacea Are Stress Diseases: The Sebaceous Gland's Own Cortisol Axis
By Jacob Gordon, INHC, FMT-CThis article contains affiliate links. As an Amazon Associate, MyBioHack earns from qualifying purchases at no extra cost to you. We only link products we research and stand behind.
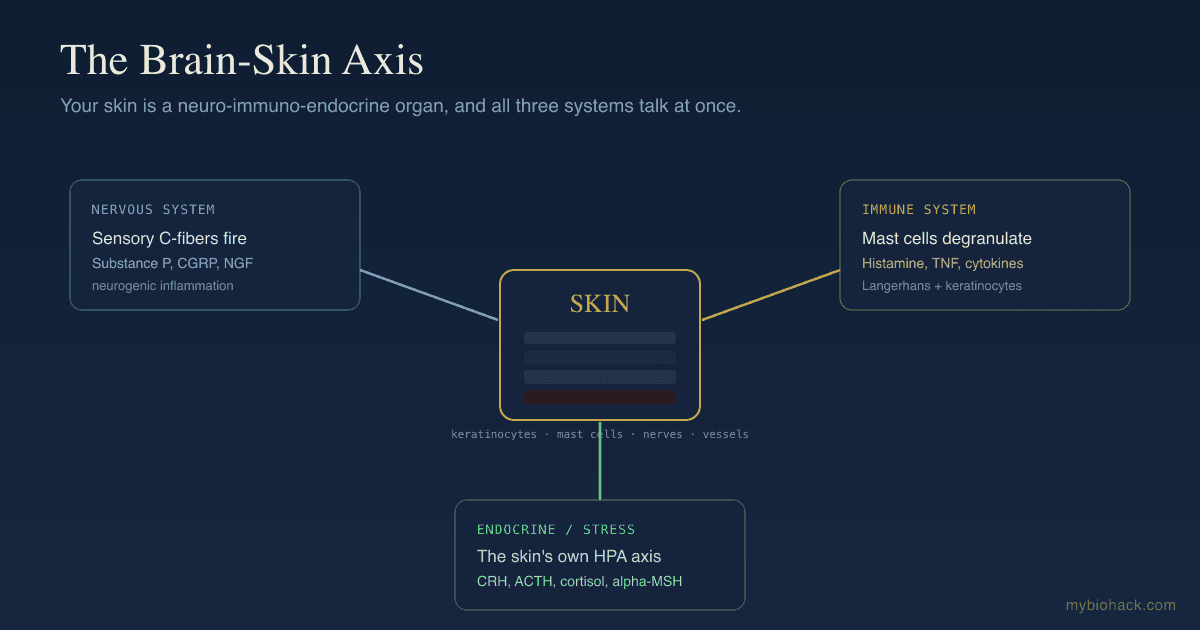
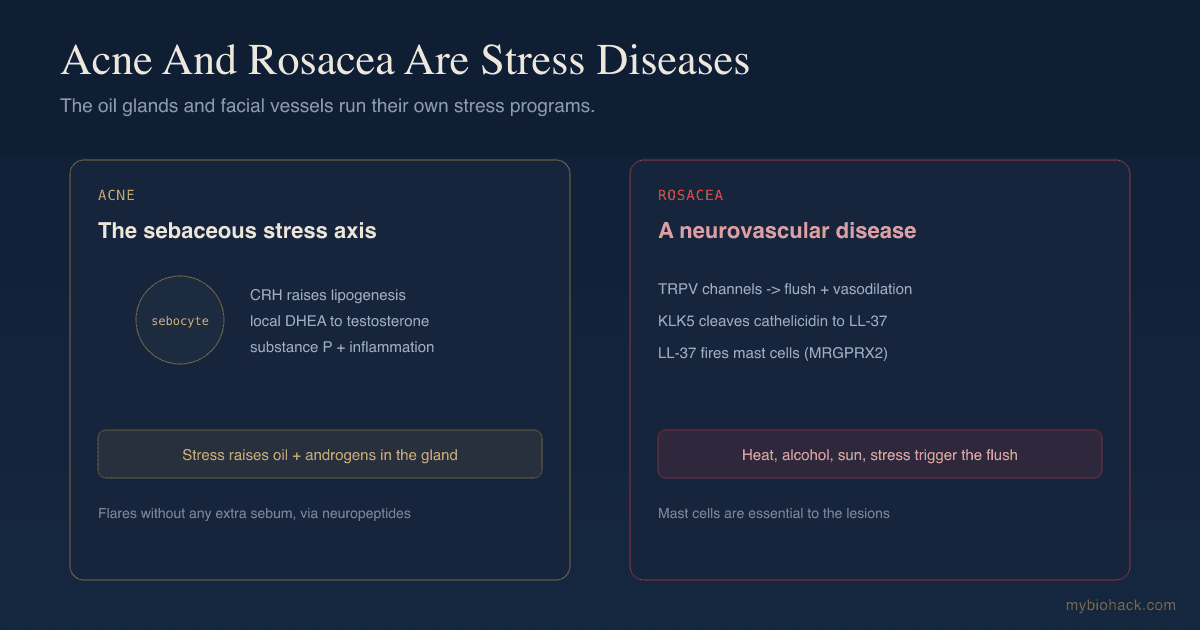
Acne and rosacea both flare with stress, and that is not psychological, it is because the skin's oil glands and facial blood vessels run their own stress hormone programs.
In this post, we will discuss the sebaceous gland's local stress axis, why CRH and substance P drive acne, how rosacea is fundamentally a neurovascular disease, and what actually calms both.

Acne And Rosacea Are Stress-Reactive
Almost everyone with acne or rosacea notices the connection to stress.
The science backs it up.
A study of adolescents found that acne severity worsened significantly with stress, and importantly, this happened without a meaningful increase in sebum quantity, which pointed straight at neuropeptides rather than oil production. R
That single finding reframes acne.
If stress worsens acne but does not increase oil, then the stress effect is running through the nerves and the inflammatory signaling, not just the grease.
Rosacea is even more obviously stress- and trigger-reactive, since flushing is triggered by heat, emotion, alcohol, spicy food, and sun, all of which act on nerves and blood vessels.
Both conditions sit on the brain-skin axis, and both are best understood as the facial skin running its own neuro-endocrine stress programs.
The Sebaceous Gland Has Its Own Stress Axis

The oil gland is not a passive grease factory.
The sebaceous gland is a fully equipped neuroendocrine organ that runs a local copy of the body's stress axis, sometimes called the seboglandular HPA axis.
Sebocytes (the cells of the oil gland) express corticotropin-releasing hormone (CRH), its binding protein, and its receptors, along with the proopiomelanocortin (POMC) peptides including ACTH, alpha-melanocyte-stimulating hormone, and beta-endorphin. R
This means the gland can mount its own stress response, locally, in your face, without any signal from your brain. R
The same machinery that runs the systemic stress response is built into the structure that produces acne.
So when you feel stressed, the gland feels it too, through its own CRH.
CRH Is The Master Switch In Acne
CRH is the most proximal element of any stress axis, and in the sebaceous gland it is a master regulator.
CRH directly induces lipid synthesis in human sebocytes and enhances the enzyme that converts dehydroepiandrosterone (DHEA) into testosterone right in the gland. R
That second point is important, because it means stress can locally raise the androgen signal that drives acne, inside the oil gland itself.
CRH is also pro-inflammatory in the gland and is upregulated in acne-involved sebaceous glands. R
It promotes the inflammatory signaling and altered lipid composition that turn a normal follicle into an acne lesion. R
So the stress hormone CRH increases oil, raises local androgens, changes the lipid composition, and adds inflammation.
That is most of the acne cascade, driven by a single stress signal.
Substance P: The Nerve's Role In Acne
The other half of the stress story is the nerve.
In acne patients, the dermal nerves around the sebaceous glands express high levels of substance P (SP). R
Substance P promotes both the proliferation and the differentiation of sebaceous glands, increases inflammatory signaling, and stimulates lipogenesis. R
It also induces the enzyme neutral endopeptidase (NEP) in the gland, which is itself elevated in acne, and it activates perifollicular mast cells. R
This is the mechanism behind the stress-without-extra-sebum finding.
Stress releases substance P from the nerves around the gland, and substance P drives proliferation, inflammation, and mast cell activation directly, no extra oil required. R
It is the same substance P and mast cell loop seen across the skin, focused on the oil gland.
Alpha-MSH And The Melanocortins
The melanocortin peptides add another layer.
Alpha-melanocyte-stimulating hormone (alpha-MSH) acts on sebocytes through melanocortin receptors, where it functions partly as a sebotropin (influencing sebum and lipid production) and partly as an anti-inflammatory signal. R
Sebocytes express two melanocortin receptors with a useful division of labor.
The melanocortin-5 receptor is more involved in sebum production, while the melanocortin-1 receptor is more involved in the anti-inflammatory, immunoregulatory role, including suppressing the inflammatory chemokine IL-8. R
This is why the melanocortin system cuts both ways in acne.
It can support oil production through one receptor and calm inflammation through another.
The net effect depends on the balance, which is part of why acne is so individual.
Rosacea Is A Neurovascular Disease
Rosacea looks like acne to many people, but mechanistically it is a different beast.
Rosacea is fundamentally a neurovascular and neuro-immune disease, centered on dysregulated blood vessels and nerves in the central face. R
The triggers tell the story.
Heat, emotional stress, alcohol, spicy food, and sun all activate transient receptor potential (TRP) channels (TRPV1 and TRPV4) on sensory nerves, driving neurogenic vasodilation and the flushing that defines rosacea. R
There is also an antimicrobial peptide problem.
In rosacea, an excess of the enzyme kallikrein-5 (KLK5) cleaves the antimicrobial peptide cathelicidin into an abnormal, highly inflammatory fragment called LL-37, which drives inflammation, blood vessel growth, and the visible redness. R
And the mast cell sits at the center.
LL-37 activates mast cells through MRGPRX2, and in mast-cell-deficient animals, LL-37 fails to produce rosacea-like lesions, which establishes the mast cell as essential to rosacea. R
So rosacea is nerves, vessels, mast cells, and a broken antimicrobial peptide, all amplifying each other.
The Stress And Mast Cell Thread
Step back and the two conditions share a spine.
In both acne and rosacea, the through-line is stress signaling (CRH and substance P) converging on the mast cell and the local inflammatory machinery. R
CRH activates mast cells.
Substance P activates mast cells.
LL-37 activates mast cells.
The mast cell is the common amplifier that turns a stress or trigger signal into visible facial inflammation, which is why both conditions respond to the same upstream levers even though their downstream pictures differ.
This is also why both flare during stressful periods regardless of skincare.
The trigger is partly internal, coming from your own stress axis and nerves.
The Brain-Skin And Junction Dysfunction Connection
Both conditions are textbook brain-skin axis diseases.
The neurogenic vasodilation and increased vascular permeability of a rosacea flush is, in Jacob's Junction Dysfunction framing, a visible burst of the same microvascular leak he calls Transient Capillary Leak Syndrome. R
And acne has a strong gut connection, since systemic endotoxin and inflammation feed the sebaceous inflammatory response, which is the subject of the post on acne and intestinal permeability.
The recurring pattern is the same as the rest of this series.
Stress and inflammation drive neuropeptides, neuropeptides drive mast cells, mast cells open vessels and amplify inflammation, and the visible skin disease follows.
Treat the upstream drivers and the downstream skin calms.
What Helps
Because both conditions are stress- and inflammation-driven, the strategy combines calming the nervous system, reducing inflammation, and addressing the specific downstream features.
1. Lower the stress signal
Since CRH and substance P are central, nervous-system work is mechanistically core, covered in the stress and skin post and the JD chapter on limbic retraining.
2. Fix the gut (especially for acne)
Endotoxin and dysbiosis amplify sebaceous inflammation, so addressing the gut barrier matters, as detailed in the acne and intestinal permeability post.
3. Calm inflammation and mast cells
Niacinamide (topical and oral) reduces inflammation in both acne and rosacea, zinc is anti-inflammatory and mildly anti-androgenic, and green tea (EGCG) reduces sebaceous inflammation.
Mast cell stabilizers like quercetin help the mast cell component shared by both.
4. Address the hormonal driver in acne
Because stress locally raises androgens in the gland, supporting healthy androgen metabolism with DIM and spearmint can help hormonally driven acne.
5. Reduce TRP triggers in rosacea
Identify and reduce the flush triggers (heat, alcohol, spicy food, sun exposure) that fire TRPV channels, and use a broad-spectrum mineral sunscreen since UV is a primary rosacea driver.
6. Support the antimicrobial peptide balance in rosacea
Azelaic acid and topical ivermectin (which addresses Demodex) target the KLK5 and LL-37 pathway and are evidence-based rosacea treatments worth discussing with a dermatologist.
What To Stay Away From
For acne, the highest-yield things to reduce are high-glycemic foods and skim dairy, both of which raise insulin and IGF-1 and worsen sebaceous activity.
For rosacea, the main triggers to avoid are the flush inducers: hot drinks, alcohol (especially red wine), spicy food, extreme heat, and unprotected sun.
For both, harsh over-cleansing and barrier-stripping actives backfire by driving more inflammation.
Testing
Testing targets the hormonal, metabolic, and inflammatory drivers.
Blood And Urine Markers
For acne, fasting insulin, androgens (testosterone, DHEA-S), and inflammatory markers are the highest-yield.
For both, a multi-point cortisol rhythm reflects the stress axis driving the sebaceous and vascular programs.
I use the Hormone Zoomer (Vibrant Wellness) or DUTCH Complete (Precision Analytical) for androgens and the cortisol curve, and the Cardio Zoomer (Vibrant Wellness) for fasting insulin and metabolic markers.
Functional Lab Panels
Because the gut drives sebaceous inflammation, I use the Gut Zoomer (Vibrant Wellness) to assess dysbiosis, permeability, and endotoxin load.
Mechanisms Of Action
Simple:
- Your oil glands and facial blood vessels make their own stress hormones, so stress can trigger acne and rosacea directly in the skin, even without extra oil.
- In both conditions, stress chemicals set off mast cells, which is the common spark that turns a trigger into visible inflammation.
Advanced:
- Seboglandular HPA axis. Sebocytes express CRH, CRH-R1, POMC and its products; CRH directly induces sebaceous lipogenesis, upregulates Δ5-3β-HSD (DHEA to testosterone conversion), and is pro-inflammatory and upregulated in acne lesions. R
- Neuropeptide drive on the gland. Substance P from periglandular nerves (elevated in acne) promotes sebocyte proliferation, differentiation, and lipogenesis, induces neutral endopeptidase, and degranulates perifollicular mast cells. R
- Melanocortin signaling. Alpha-MSH acts on sebocyte MC5R (sebogenesis) and MC1R (anti-inflammatory, IL-8 suppression), giving melanocortins a dual role in sebaceous biology. R
- Rosacea cathelicidin cascade. TRP channel activation and TLR2 signaling drive KLK5-mediated cleavage of cathelicidin into LL-37, which activates mast cells via MRGPRX2 to produce cytokines and MMP-9, with mast cells essential to lesion formation. R
- Neurogenic vasodilation. TRPV1/TRPV4 on facial sensory nerves trigger CGRP and other neuropeptide release, producing the vasodilation, flushing, and increased permeability characteristic of rosacea. R
Genetics
Several genes set susceptibility to these conditions.
CRHR1
CRHR1 encodes the dominant CRH receptor in sebocytes, the entry point for the stress signal that drives lipogenesis and inflammation in the gland.
MC1R And MC5R
These melanocortin receptors split the melanocortin response in the gland, with MC5R favoring sebum production and MC1R favoring anti-inflammatory signaling.
TACR1
TACR1 encodes the NK-1 receptor for substance P, the neuropeptide elevated around acne sebaceous glands.
HLA (Rosacea)
Rosacea has been linked to specific HLA class II variants, consistent with its immune and neuro-immune component, and clusters with other inflammatory conditions.
More Research
A few additional threads are worth following.
Acne is increasingly understood as an inflammatory disease from the very first lesion, with inflammation preceding the visible comedone, which is why anti-inflammatory and neuro-immune approaches matter alongside the classic focus on oil and bacteria. R
Rosacea's LL-37 and KLK5 cascade creates a self-amplifying loop, since the MMP-9 released by mast cells further activates KLK5, which is why rosacea tends to become more reactive over time without intervention. R
The shared mast cell mechanism in both conditions suggests that mast-cell-directed therapy is an underused common lever, an active area of investigation. R
For the gut driver of acne, see acne and intestinal permeability, and for the broader framework, the brain-skin axis pillar.
For biomarker testing I use the Hormone Zoomer and the Gut Zoomer to assess the hormonal and gut drivers together.
If you have stubborn acne or rosacea that tracks with stress, reach out for a consultation.
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Quercetin
500mg 2x/day
SPM Active (Pro-resolving Mediators)
2 softgels/day
Curcumin (Liposomal)
500mg 2x/day