Stress And Your Skin: Why Acute Stress Protects And Chronic Stress Destroys
By Jacob Gordon, INHC, FMT-CThis article contains affiliate links. As an Amazon Associate, MyBioHack earns from qualifying purchases at no extra cost to you. We only link products we research and stand behind.
Stress changes your skin through the same hormones your brain uses, and whether that helps or harms depends almost entirely on how long the stress lasts.
In this post, we will discuss the difference between acute and chronic stress on skin immunity, the two hormonal highways that carry stress to the skin, why short stress can actually strengthen skin defense, and why ongoing stress drives flares, slow healing, and a broken barrier.

Stress Is Not One Thing
The single most important fact about stress and the skin is that the effect flips depending on duration.
Stress has bidirectional effects on immune function, where acute stress is immunoenhancing and chronic stress is immunosuppressive or dysregulating. R
Acute stress lasts minutes to hours, like a confrontation, a hard workout, or a fright.
Chronic stress persists for weeks to months, like caregiving, financial strain, or unresolved trauma.
The body evolved the acute response as a survival tool, a way to pre-position immune defenses before a likely wound or infection. R
The chronic response is what happens when that emergency system never gets to stand down.
This is the lens for the entire post.
Short bursts of stress are not the problem.
The problem is a stress response that runs continuously for months on end.
The Two Stress Highways

Stress reaches the skin through two main pathways.
The first is the hypothalamic-pituitary-adrenal (HPA) axis, which releases corticotropin-releasing hormone (CRH), then adrenocorticotropic hormone (ACTH), and finally cortisol from the adrenal glands.
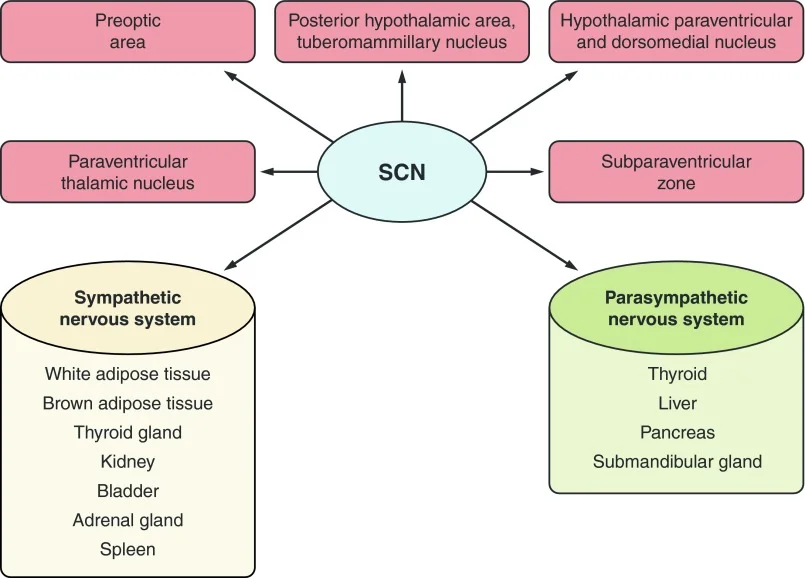
The second is the sympathetic nervous system (SNS), which releases the catecholamines epinephrine (adrenaline) and norepinephrine (noradrenaline).
Both pathways end at the skin, where keratinocytes, mast cells, Langerhans cells, and immune cells all carry receptors for these hormones. R
The magnitude and duration of cortisol and catecholamine exposure is what determines whether the net effect on the skin is protective or destructive. R
This is also why the dose matters so much.
Endogenous stress hormones at physiological concentrations can enhance immunity, while the same hormones at high or sustained concentrations, and synthetic steroids, suppress it. R
That single distinction explains a lot of the confusion around cortisol.
Acute Stress Actually Boosts Skin Immunity
This surprises most people.
A brief stressor delivered right before an immune challenge significantly enhances skin cell-mediated immunity, not suppresses it. R
The mechanism is leukocyte trafficking.
Acute stress causes immune cells to leave the blood and redeploy into the skin, the tissue most likely to be wounded in a fight-or-flight scenario, where they amplify the local immune response. R
This stress-induced enhancement of the skin response depends on the stress hormones themselves and on interferon-gamma (IFN-gamma) signaling. R
Low doses of corticosterone or epinephrine given acutely enhance the skin immune response, while high doses or synthetic steroids suppress it. R
There is a useful takeaway here.
This is part of why vaccines, surgery recovery, and acute infections can benefit from a body that mounts a sharp, time-limited stress response.
The acute stress response is not a malfunction.
It is the body loading its immune cells into the tissue before the expected hit.
Chronic Stress Breaks It Down
Now run that same system for months.
Chronic stress suppresses and dysregulates immunity by reducing circulating immune cell numbers, blunting cytokine signaling, and shifting the balance between cell types. R
In the skin specifically, chronic stress suppresses the cell-mediated immune response, the opposite of what acute stress does. R
Chronic stress also skews the immune system away from a balanced response and toward patterns that favor allergy and persistent inflammation.
Sustained catecholamine exposure suppresses Th1 (cell-mediated) immunity and pushes the system toward Th2 (allergic, antibody-driven) responses. R
This is the immunological setup for atopic, allergic, and chronically inflamed skin.
It is also why chronically stressed people get more infections, heal slower, and flare more easily.
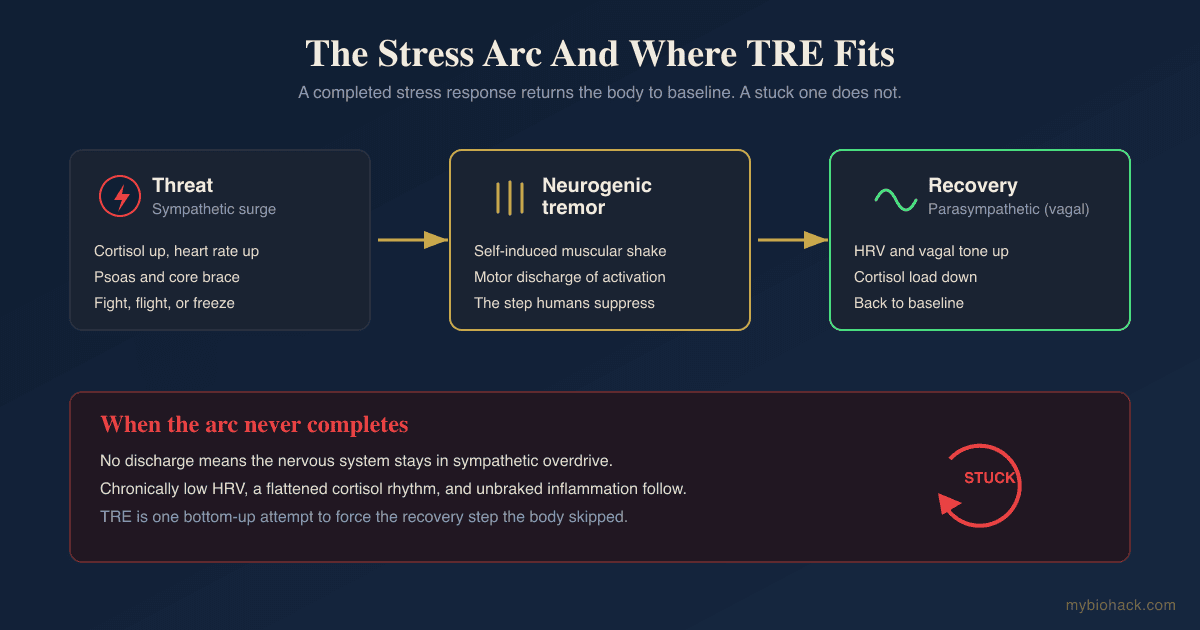
The emergency system that was supposed to protect them is now running them down.
In Jacob's Junction Dysfunction framework, this is the familiar pattern of acute immune activation collapsing into chronic immune suppression, the same "stuck" state that shows up across post-viral and chronic illness.
How Stress Hormones Reach The Skin
Here is the part that makes stress feel so physical in the skin.
The skin does not just receive stress signals from the brain.
It runs its own local copy of the stress axis, producing CRH, ACTH, cortisol, and related peptides directly in skin cells. R
When CRH is released in the skin, it activates dermal mast cells and makes blood vessels leaky, which is the molecular bridge between a stressful moment and a visible skin reaction. R
Acute psychological stress does exactly this, raising skin CRH, degranulating mast cells, and increasing vascular permeability, an effect partly blocked by antihistamines. R
The catecholamine arm hits a different target.
Epinephrine and norepinephrine suppress the antigen-presenting function of Langerhans cells through the beta-2 adrenergic receptor, dampening the skin's ability to mount a coordinated immune response. R
So stress reaches your skin two ways at once.
CRH and cortisol act on mast cells and barrier function, while catecholamines act on the dendritic cells that orchestrate immunity.
The mast cell side of this is the cleanest visible example of what Jacob calls Transient Capillary Leak Syndrome (TCLS), neuropeptide and stress-hormone signaling opening the microvasculature.
Stress And The Skin Barrier
Stress does not only change immunity.
It physically weakens the skin barrier.
Psychological stress perturbs epidermal permeability barrier homeostasis, slowing the recovery of the skin's protective barrier after it is disrupted. R
This matters because a slower barrier recovery means more water loss, more irritant and allergen penetration, and more inflammation.
It is a direct mechanistic link between feeling stressed and a flare of eczema or psoriasis.
In the original work, the stress-induced barrier defect could be blocked by sedatives that reduced the stress response, confirming the brain was driving the skin change. R
A broken barrier then feeds neurogenic inflammation, because irritants and microbes that get through activate the same sensory nerves and mast cells.
The loop closes on itself.
Stress And Wound Healing
The clearest demonstration of chronic stress harming the skin came from a wound healing study.
Caregivers under chronic stress took significantly longer to heal a standardized skin wound than matched controls, 48.7 days versus 39.3 days, a 24 percent slowdown. R
Their immune cells also produced less interleukin-1 beta (IL-1 beta) in response to a bacterial challenge, pointing to a blunted early inflammatory phase. R
This is important because the early inflammatory phase is not optional.
It is the first step of the wound healing cycle, and suppressing it stalls everything downstream.
Cortisol is the main culprit, since glucocorticoids reduce the inflammatory signaling, immune cell recruitment, and growth factor expression that early healing depends on.
This is the same reason surgical recovery, athletic recovery, and skin repair all suffer under chronic stress.
The Stress-Driven Skin Conditions
Once you see the mechanisms, the list of stress-reactive skin conditions makes sense.
The conditions most clearly worsened or triggered by stress include the following (not an exclusive list):
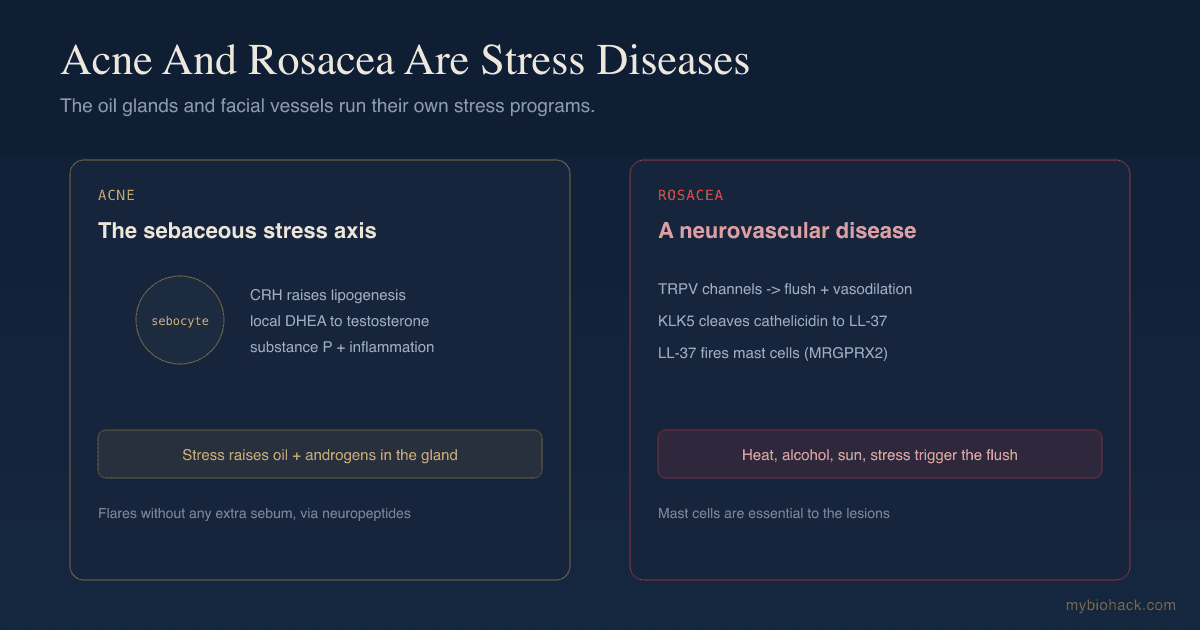
- Acne and rosacea, where the sebaceous gland runs its own CRH-driven stress program
- Alopecia areata and telogen effluvium, where stress neuropeptides drive the follicle into shedding
- Atopic dermatitis (eczema), where stress shifts immunity toward Th2 and weakens the barrier
- Chronic urticaria (hives), where CRH and catecholamines degranulate mast cells from stress alone
- Psoriasis, a Th1-driven disease that flares with sympathetic activation
- Vitiligo, where stress signaling damages the pigment-protecting melanocortin system
Adrenergic urticaria deserves a special mention because it is the purest example.
In adrenergic urticaria, hives appear specifically at times of stress, each surrounded by a white halo of vasoconstriction, and can be reproduced by injecting noradrenaline and prevented by the beta-blocker propranolol. R90905-5/fulltext)
It is stress, written directly onto the skin in the form of a rash.
What To Do About It
Because the skin is downstream of the nervous system, calming the nervous system is part of the dermatology, not separate from it.
1. Treat limbic and stress retraining as foundational, not optional
In Jacob's clinical experience, people rarely recover from stress-driven skin conditions through supplements alone.
The highest-leverage work is retraining the stressed limbic system, the subject of the JD chapter on overcoming trauma's effect on the limbic system.
Approaches include meditation, breathwork, NLP, and structured programs like DNRS and the Gupta Programme.
2. Fix the circadian rhythm that runs cortisol
Cortisol is a circadian hormone, and a flipped or flattened rhythm dysregulates the entire skin stress response.
Morning sunlight, consistent meal timing, and dark cool nights anchor the rhythm, covered in the JD chapter on circadian biology.
3. Use adaptogens to blunt the stress hormone surge
Several adaptogens reduce cortisol reactivity and support a healthier stress curve.
Useful options include ashwagandha, rhodiola, holy basil, and phosphatidylserine (which can lower the cortisol response to stress).
4. Support the calming neurotransmitters
Theanine raises alpha brain waves and takes the edge off acute stress without sedation.
Magnesium (glycinate form) supports the stress response and sleep.
5. Protect sleep
Sleep deprivation is itself a chronic stressor that dysregulates cortisol and pro-inflammatory cytokines.
Melatonin and the broader sleep stack matter here because poor sleep undoes everything else.
Testing
Stress leaves measurable fingerprints, but only if you test at the right times.
Blood And Urine Markers
A single morning cortisol tells you almost nothing, because the meaningful signal is the shape of the curve across the day.
DHEA-S is the counter-regulatory adrenal hormone, and a low DHEA-S (or a low DHEA-S to cortisol ratio) tracks with psychological distress in chronic skin conditions like urticaria. R
Functional Lab Panels
I use the DUTCH Complete (Precision Analytical) or the Hormone Zoomer (Vibrant Wellness) to map the full cortisol rhythm, cortisol metabolites, and DHEA across the day.
For the downstream inflammatory and mast cell picture, the Immune Zoomer (Vibrant Wellness) adds mast cell and autoimmune markers.
If your skin tracks with your stress, the cortisol curve is the first thing to see objectively.
Mechanisms Of Action
Simple:
- A short burst of stress sends immune cells into your skin and strengthens its defenses, which is protective.
- Months of stress floods the skin with cortisol and adrenaline, which suppresses immunity, weakens the barrier, slows healing, and triggers flares.
Advanced:
- Leukocyte redeployment. Acute stress, via catecholamines and a transient glucocorticoid pulse, mobilizes leukocytes out of the blood and into peripheral compartments including skin, enhancing local cell-mediated immunity and DTH responses; this is glucocorticoid- and IFN-gamma-dependent. R
- Dose-dependent glucocorticoid effects. Low physiological glucocorticoid and catecholamine levels are immunoenhancing, while high or sustained levels (and synthetic steroids) are immunosuppressive, explaining the opposite outcomes of acute versus chronic stress. R
- Catecholamine suppression of antigen presentation. Epinephrine and norepinephrine act on beta-2 adrenergic receptors on Langerhans cells to inhibit antigen presentation and skew priming toward Th2, suppressing contact hypersensitivity. R
- CRH-mast cell-vascular permeability axis. Skin CRH activates CRHR1 on dermal mast cells, triggering degranulation and increased vascular permeability, the local effector arm of the cutaneous stress response. R
- Barrier homeostasis. Glucocorticoids inhibit epidermal lipid synthesis and lamellar body production, slowing permeability barrier recovery and increasing susceptibility to irritants, allergens, and infection. R
Genetics
Stress reactivity in the skin is partly heritable.
NR3C1
NR3C1 encodes the glucocorticoid receptor, which sets cortisol sensitivity throughout the body.
Variants that change receptor sensitivity alter how strongly cortisol suppresses skin immunity and barrier repair.
The BclI variant (rs41423247) is associated with altered glucocorticoid sensitivity.
FKBP5
FKBP5 regulates glucocorticoid receptor sensitivity and the shut-off of the stress response.
The rs1360780 variant is associated with altered cortisol regulation and stress-related conditions.
ADRB2
ADRB2 encodes the beta-2 adrenergic receptor, the catecholamine receptor on Langerhans cells, keratinocytes, and immune cells.
The Arg16Gly (rs1042713) and Gln27Glu (rs1042714) variants of the beta-2 receptor have been linked to psoriasis and atopic dermatitis reactivity.
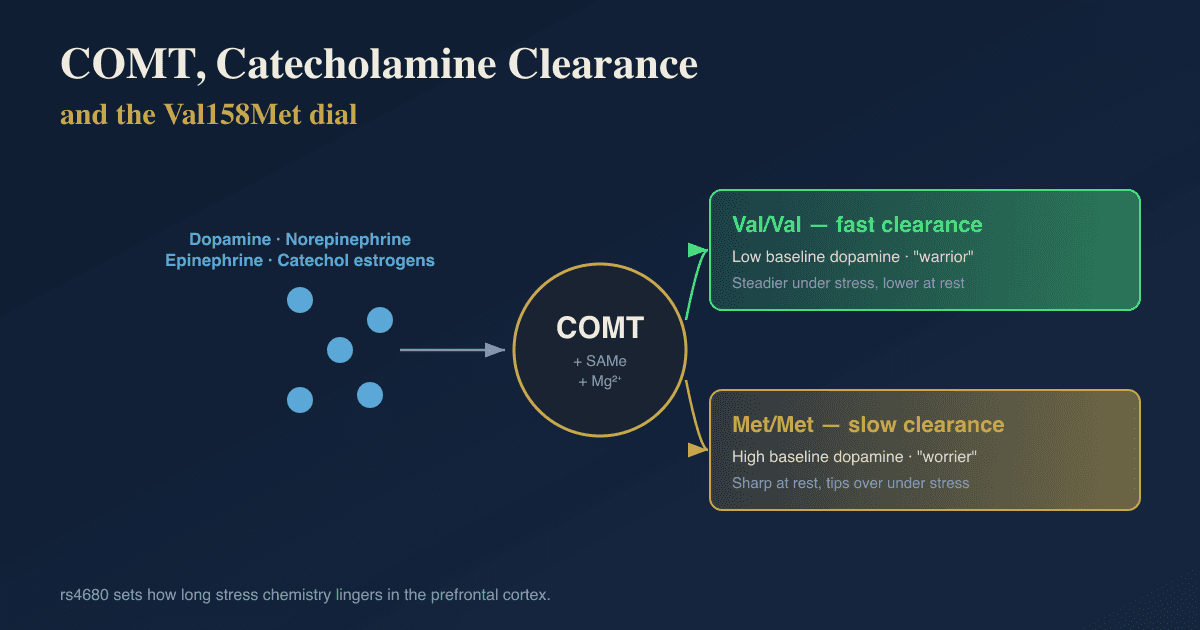
COMT
COMT breaks down catecholamines, so the slow Val158Met variant (rs4680) prolongs adrenaline and noradrenaline signaling at the skin.
See the dedicated post on COMT genetics and catecholamine metabolism for the full breakdown.
More Research
A few additional threads are worth following.
Adrenergic urticaria and cholinergic urticaria can coexist, and both are autonomic-nervous-system-dependent rather than allergen-dependent, which is why standard allergy testing so often comes back clean. R90905-5/fulltext)
Chronic stress increases susceptibility to skin cancer in animal models by suppressing protective Type 1 cytokines and tumor-fighting T cells while increasing suppressor cell function, which is the same immunosuppressive pattern seen with chronic glucocorticoid exposure. R
DHEA-S is worth tracking over time, since its decline in chronic skin conditions may be both a marker of distress and a contributor to the loss of immune balance. R
For the deeper mechanism behind why the skin stress axis matters at all, start with the pillar post on the brain-skin axis.
For biomarker testing I use the DUTCH Complete and the Hormone Zoomer to assess the cortisol rhythm and adrenal reserve together.
If your skin flares with stress and you want help mapping it, reach out for a consultation.
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Quercetin
500mg 2x/day
SPM Active (Pro-resolving Mediators)
2 softgels/day
Curcumin (Liposomal)
500mg 2x/day