What Is Vitiligo? Mechanisms and 25+ Ways To Improve It
By Jacob Gordon, INHC, FMT-CThis article contains affiliate links. As an Amazon Associate, MyBioHack earns from qualifying purchases at no extra cost to you. We only link products we research and stand behind.
Vitiligo is a long term skin condition characterized by patches of the skin losing their pigment. R
In this post, I will break down the mechanism behind vitiligo, as well as provide science-based biomarkers and proven treatments that help with this autoimmune condition.

Basics
Vitiligo is when patches of skin affected become white and usually have sharp margins. The hair from the skin may also become white. R
This happens because the cells (melanocytes) that make pigment (color) in the skin are destroyed. R
It affects 1-3% of the population. R
Symptoms
Some of the common symptoms of vitiligo are patchy depigmented skin (esp. on the extremities). R R
They can also be around body orifices (mouth, eyes, nostrils, genitalia, umbiicus, etc). R R
These patches can grow and change in shape. R R
Lesions may occur and depigmentation can happen around them. R
Unfortunately, some may feel ashamed (since it can be visual) and develop mood disorders. R
Here are some resources, if you are having trouble living with vitiligo ---> R R R R
Auto-Immunity
Vitiligo is an autoimmune disease that is initiated by melanocyte stress, which can be worsened by exposure to chemicals. R
Vitiligo has been associated with other autoimmune and inflammatory diseases:
Mechanism of Action

Recent evidence suggests that oxidative stress, auto-immunity and melanocyte apoptosis are involved vitiligo. R
Essentially what happens in vitiligo is hyperactive T cells decide to target and kill melanocytes: R
Melanocytes have abnormally high levels of cellular stress, which can be caused by inherited factors, genetic factors, or both.
Stressed melanocytes produce signals that activate innate immune cells to initiate inflammation that leads to autoimmunity.
Innate immune signals recruit adaptive immune cells (primarily CD8+ T Cells) into the skin, which then find melanocytes and kill them, resulting in white spots, or depigmentation.
Innate Immunity
The innate immunity is the first line of "defense" against pathogens and immune problems. R
It can identify infectious agents through pattern recognition receptors (PRRs). R
PRRs responde to tissue injury by recognizing damage associated molecular patterns (DAMPs). R
Abnormal melanocytes release DAMPs that activate the innate immunity. R
Adaptive Immunity
The adaptive immunity involves T and/or B cells. R
They target specific proteins. R
In vitiligo, CD8+ T cells infiltrate the epidermis and kill melanocytes. R
IP-10 (The Master Switch)
IFN-g (Interferon gamma) is a cytokine that is important for the development of vitiligo. R
Many genes are turned on by IFN-g, so IFN-g may be a master switch for vitiligo. R
We need IFN-g for survival or we will die, since it helps with infection. R
IFN-g induces IP-10 (CXCL10). R
CXCL10 binds with CXCR3, which is found on melanocyte-specific CD8+ T cells, which cause vitiligo. R
IL-8
TH1 cells increase the expression of VEGF, by TH1 cells and mast cells. R
Mast cells then release inflammatory cytokines IL-6 and TNF-a.
NLP1 can also activate IL-1b. R
IL-1, IL-6 and TNF-a can stimulate IL-8 release. R
IL-8 is produced by monocytes, mast cells, fibroblasts, endothelial cells, dendritic cells and keratinocytes. It is chemotactic to neutrophils, T-cells, basophils and keratinocytes. R
IL-8 induces oxidative stress in the skin. R
IL-1 and TNF-a, released from mast cells, can also increase vitiligo lesions. R R
Things like phenols can induce the production of IL-8 (and IL-6), making vitiligo worse. R
Oxidative Stress
Melanocytes in vitiligo patients are abnormal. R
They get damaged by reactive oxygen species (ROS) and activate of the unfolded protein response. R
HSP70, a heat shock protein, and exosomes, secretes cell-derived nanoparticles, as potentially important signals that promote inflammation in vitiligo. R
Systemic oxidative stress in vitiligo patients may develop due to an imbalance in enzymatic and non-enzymatic antioxidant systems. R
This problem may be caused by low glutathione peroxidase and reduced glutathione, which may prolong hydrogen peroxide exposure. R
Also, in vitiligo patients, there has been shown decreased recycling levels of tetrahydrobiopterns. R
ROS can trigger the loss of dendrites of melanocytes, thus affecting melanosome transfer to surrounding keratinocytes. R
Oxidative stress can induce apoptosis in melanocytes by releasing caspase-activating cytochrome c from mitochondria. R
Neurotransmitters
Neurochemical mediators that are secreted by cutaneous axon terminals, such as norepinephrine (NE) and acetylcholine (Ach) are toxic to melanocytes. R
Melanocytes seem to have less acetylcholine esterase, the enzyme to break down acetylcholine. R
NE has direct melanocytotoxic effects by interfering with cellular sulfhydryl groups, impairing mitochondrial calcium uptake and inhibiting melanogenesis. R
Elevated levels of the NE degrading enzyme monoamine oxidase (MAO) in both melanocytes and keratinocytes can kill melanocytes. R
CD49a
Vitiligo is characterised by the accumulation of a subgroup of T cells called CD49a+, which recognise and are ready to kill pigment cells. R
In psoriasis, another kind of T cell, CD49a- accumulates in the afflicted skin and produces the inflammation-causing protein IL-17. R
In healthy skin, CD49a+ and CD49a cells are dormant, but quickly respond with inflammatory and cytotoxic effects when stimulated by IL-15, a protein secreted from skin cells as a rapid-response defence against microbial attack. R
More Inflammatory Pathways
Haptens can cause sensitization of skin cells, priming the immune system to react to chemicals.
Histamine can cause itching and stimulated the proliferation and migration of melanocytes and the vitiliginous keratinocyte survival. R R
IL-33 augments substance P (SP)-induced VEGF release from human mast cells. R
SP can stimulate TNF secretion from mast cells and a good correlation has been recently reported between serum TNF and the extent of vitiligo. R
Corticotropin releasing hormone (CRH) secreted under stress, can activate local mast cells to release pro-inflammatory mediators. R
This could potentially trigger the release of melanin degrading and pro-apoptotic molecules, rendering the stressed skin vulnerable to hypopigmentation. R
Melanocytes have been reported to express corticotropin releasing hormone receptor-1. R
CRH in the skin upregulates the synthesis and secretion of proopiomelanocortin (POMe) and its peptides, with POMC being an important regulator ofmelanogenesis. R
mRNA expression of POMC and its receptors, melanocortin receptor-1 (MC1R) and -4 (MC4R), is significantly decreased in lesional vitiligo skin, but increased in non-lesional vitiligo skin compared to healthy controls. R
Biomarkers and Tests
IL-1b R
IL-9 R
IL-33 R
IFN-g R
Neurotensin R
Serum CXCL10 R
TNF-a R
TSLP R
You can order these blood tests here.
What Is Effective For Vitiligo?
Actions to Take:
Before taking any actions, always consult with a qualified health professional.
In all forms, it looks like more sun would help. Fixing the underlying factors below are going to help significantly. Luteolin is a great natural way to tackle most of these problems.
Decrease Acetylcholine (vagus nerve stimulation should be fine and help regulate this) R
Decrease IL-1b
Decrease IL-8
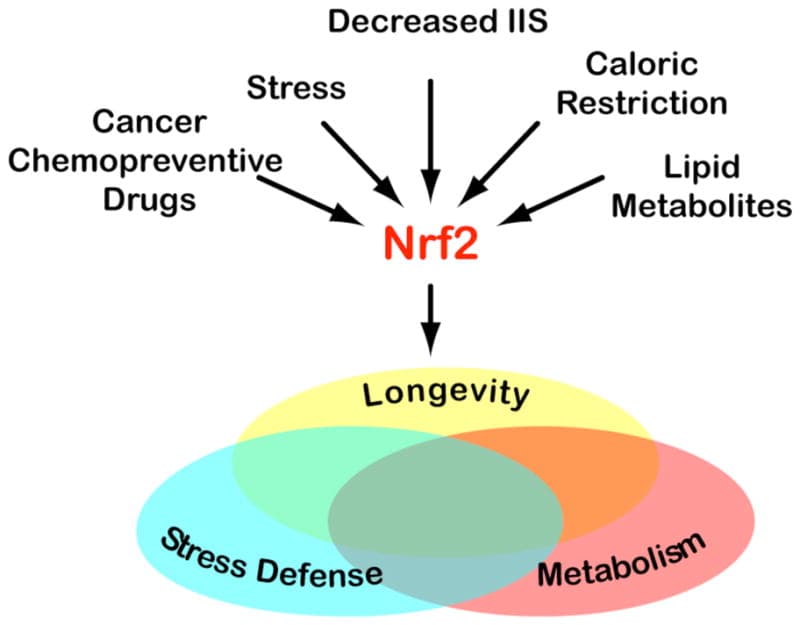
Decrease NRF2
Decrease TNF-a
Decrease CXCL10
Decrease VEGF R
Increase Tregs and TGFb1 R
Remove gluten and other inflammatory lectins
Reduce Hapten Exposure
Reduce Stress R
Reduce ROS R
Stabilize Mast Cells
Stay away from Estrogenics (like benzenes and phenols, which includes lotions, sunscreens, etc) R R R
Stay away from Proton Pump Inhibitors R R R
Treat underlying Dysbiosis and Histamine Intolerance
Supplements:

Glutathione (helps against ROS) R
Luteolin (blocking TNFa, IL-1b, and IL-8 release from melanocytes) R
Drugs:
Afamelanotide (such as Melanotan) R
CXCR3 Depleting Antibodies R
Metharmon-F (a sex steroid-thyroid hormone - increased MSH) R
Monobenzone (FDA approved but damages cells so may make vitiligo worse) R
Ruxolitinib R
Simvastatin (Inhibits STAT1 activation) R
Tofacitinib (treats RA and Vitilgo effectively, but inhibits JAK2/STAT3 pathway) R R R
Topical Steroids R
Topical Tacrolimus R
Treatments and Devices:
Genetics

NLRP1
NLP1 can activate IL-1b. R
TYR
TYR encodes tyrosinase, an enzyme of the melanocyte that catalyzes melanin biosynthesis, and a major autoantigen in generalized vitiligo. R
rs1393350
The A allele is protective, with each A associated with 0.65 times lower odds R
rs1847134
rs1018528
rs10765198
rs1847134
rs1393350
rs1126809
rs1806319
HLA-DRB1
rs532098
each A allele is associated with about 1.6 times higher odds) R
HLA-A
rs12206499 R
rs3823355
the HLA-A*02 MHC Class I allele R
rs3823355
Each T allele is associated with 1.5 times higher odds R
TSLP
TSLP is a cytokine structurally and functionally similar to interleukin-7 (IL-7) and has been implicated in conditions like asthma, allergic rhinitis and atopic dermatitis based on its ability to maintain immune homeostasis. R
LPP
rs1464510 R
GZMB
rs8192917
Each C allele is associated with 1.3 times higher odds R
UBASH3A
rs11203203
Each A allele is associated with 1.3 times higher odds R
C1QTNF6
rs229527
Each A allele is associated with 1.4 times higher odds R
PTPN22
rs2476601
Each A allele is associated with 1.54 times higher odds R
CTLA4
rs231775 R
XBP1
rs2269577 R
SLC1A2
SMOC2
rs13208776 R
RERE
rs4908760
Each G allele is associated with 1.4 times higher odds R
LRP
rs13076312
Each T allele is associated with 1.3 times higher odds R
IL2RA
rs706779
Each T allele is associated with 1.3 times higher odds R
RNASET2
rs2236313
Each T allele is associated with 1.2 times higher odds in a Han Chinese population R
WASF5P
rs9468925
The A allele appears to be protective in people of Han Chinese descent; the AA genotype is associated with 0.74 times lower odds than AG, and GG individuals have 1.35 times higher odds R
More Research
We reported decrease in acetylcholine esterase activity in vitiligo patients as compared to controls suggesting the involvement of neural factors in pathogenesis of vitiligo. R
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Quercetin
500mg 2x/day
Vitamin D3 + K2
5000 IU + 200mcg/day
DAO Enzyme
1 cap before meals