Psoriasis As A Neuroimmune Disease: Neurogenic Inflammation, NGF, And Why Cutting A Nerve Can Clear A Plaque
By Jacob Gordon, INHC, FMT-CThis article contains affiliate links. As an Amazon Associate, MyBioHack earns from qualifying purchases at no extra cost to you. We only link products we research and stand behind.
Psoriasis is treated as an immune disease, but the nerves in the skin are not bystanders, they are drivers, and the proof is that cutting the nerve to a plaque can clear it.
In this post, we will discuss the immune engine of psoriasis, the neurogenic layer that the immune story leaves out, why nerve growth factor sits at the center, and what the denervation evidence means for treatment.

Psoriasis Is More Than An Immune Disease
The modern understanding of psoriasis is built around the immune system, specifically the IL-23/IL-17 axis, and that understanding is correct.
But it is incomplete.
Psoriasis lesions are distributed symmetrically, follow nerve patterns, flare with stress, appear at sites of trauma, and can clear when the nerve supplying them is damaged. R
None of those features are explained by immunology alone.
They are explained by the nervous system.
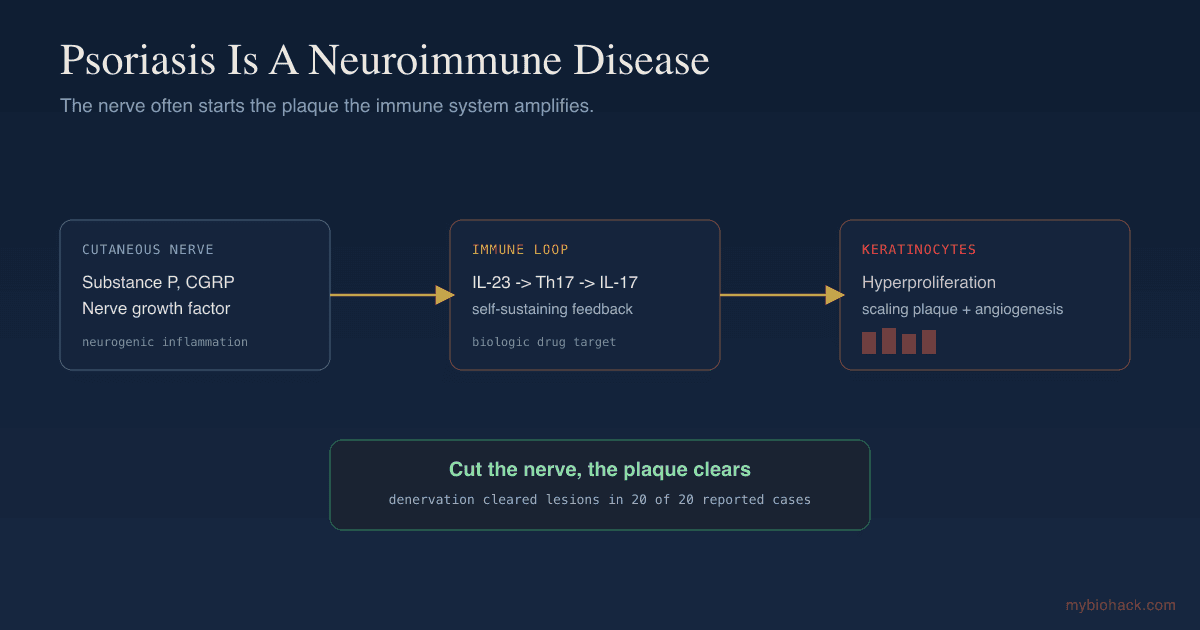
Psoriasis is best understood as a neuroimmune disease, where cutaneous nerves and the immune system drive each other, and the nerve is often the trigger that the immune system amplifies. R
This is a more complete model, and it opens up treatment angles that pure immunosuppression misses.
We already have a full protocol for naturally reversing psoriasis, so this post focuses on the neuroimmune mechanism that explains why those approaches work.
The IL-23/IL-17 Immune Engine
Start with the immune engine, because it is real and it is the target of the best modern drugs.
Activated dendritic cells in the skin produce interleukin-23 (IL-23), which drives Th17 cells to produce interleukin-17 (IL-17). R
IL-17 then acts on keratinocytes, which respond by proliferating abnormally and pumping out antimicrobial peptides and chemokines like CCL20, which recruits even more Th17 cells and dendritic cells. R
That is a self-sustaining inflammatory feedback loop, and it is why biologics targeting IL-23 and IL-17 work so well. R
But this raises a question the immune model struggles to answer.
What starts the loop, and what decides where it starts?
That is where the nerves come in.
The Neurogenic Layer
Psoriatic skin is not just immunologically abnormal, it is neurologically abnormal.
Psoriatic lesions contain an increased density of nerve fibers and elevated levels of the neuropeptides substance P (SP), calcitonin gene-related peptide (CGRP), and vasoactive intestinal peptide (VIP). R
Each one contributes to the plaque.
Substance P is chemotactic for neutrophils, activates T cells, releases interleukin-1 from keratinocytes, and helps initiate the inflammatory process. R
CGRP is a potent vasodilator and synergizes with substance P to stimulate keratinocyte proliferation, while both CGRP and VIP are potent mitogens for the endothelial cells that build the abnormal blood vessels of a plaque. R
Substance P also drives the immune engine directly, stimulating Th17 differentiation and IL-17A production through the NK-1 receptor on T cells. R
So the nerves are not downstream of the immune loop.
They feed it from the top.
NGF Is The Central Neuro-Driver

If one molecule ties the neurogenic story together, it is nerve growth factor (NGF).
NGF protein is markedly increased in psoriatic skin, psoriatic keratinocytes produce more of it than normal keratinocytes, and its receptors TrkA and p75NTR are upregulated on the nerves in lesions. R
NGF does almost everything a psoriatic plaque needs.
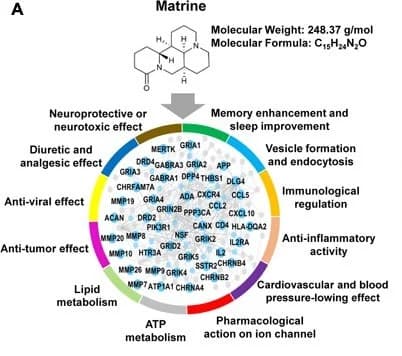
It stimulates keratinocyte proliferation, sprouts and sensitizes nerve fibers, upregulates substance P and CGRP, activates T cells, induces the chemokine RANTES in keratinocytes, induces the adhesion molecule ICAM-1, degranulates mast cells, and promotes angiogenesis. R
Read that list again, because it is essentially the full pathology of a psoriasis plaque produced by a single neurotrophin.
This is why NGF is a recurring villain across inflammatory skin disease, and why blocking NGF and its receptor improves psoriasis in models. R
NGF is the link between the keratinocyte, the nerve, and the immune cell.
The Smoking Gun: Cut The Nerve, Clear The Plaque
Here is the observation that proves nerves are causal, not incidental.
When the nerve supplying a patch of psoriatic skin is damaged, the psoriasis in that area often clears.
A review of denervation cases found that in 20 out of 20 reports, psoriatic lesions under the control of an injured nerve cleared or improved spontaneously, with only about a third experiencing partial recurrence. R
The causes of denervation included surgical nerve injury, stroke, and polio, all of which spared the affected skin from psoriasis. R
This has been known for decades, with the classic report of psoriasis remission following cutaneous nerve section. R
Animal work confirms the mechanism.
Surgically cutting the nerves to psoriasiform mouse skin reduced dendritic cells, improved the skin thickening, and lowered IL-23 and T cell numbers, in a way that depended on sensory neuropeptides. R
You cannot get a cleaner demonstration.
Remove the nerve input, and the immune-driven plaque recedes.
The Koebner Phenomenon
The neurogenic model also explains one of psoriasis's strangest features.
The Koebner phenomenon is the appearance of new psoriatic lesions at sites of skin trauma, like a scratch, a cut, or a tattoo.
In the neurogenic framework, trauma activates and damages cutaneous nerves, which release a surge of neuropeptides and NGF, which then triggers the local keratinocyte and immune cascade right at the injury site. R
This is why a wound in a person with psoriasis can heal into a plaque instead of normal skin.
The injured nerve turns a wound into a lesion.
It is the same nerve-driven mechanism, just triggered by physical trauma instead of stress.
Stress Flares Psoriasis
Stress is one of the most reliable psoriasis triggers, and the mechanism is the same neurogenic and neuroendocrine wiring.
Stress activates the sympathetic nervous system and the HPA axis, releasing neuropeptides and altering the cortisol response, which promotes inflammation and impairs the skin barrier. R
Interestingly, psoriasis patients whose disease is stress-reactive show a blunted cortisol response to stress, an impaired HPA axis rather than simply high cortisol. R
This fits the broader pattern covered in the stress and skin post, where a dysregulated rather than simply elevated stress response drives chronic skin disease.
The takeaway is that stress is not a psychological footnote in psoriasis.
It is a direct trigger of the neurogenic cascade that builds the plaque.
The Brain-Skin And Junction Dysfunction Connection
Psoriasis is a clear example of the brain-skin axis.
Nerves release substance P, CGRP, and NGF, which drive keratinocyte proliferation, mast cell degranulation, T cell activation, and angiogenesis, the same neurogenic inflammation and mast cell loop seen across the skin. R
The abnormal new blood vessels of a plaque are driven by VEGF and the neuropeptide mitogens, the kind of vascular remodeling that connects to Jacob's Junction Dysfunction framework, where VEGF should not be reflexively suppressed because it is part of an adaptive response.
There is also a framing point worth making.
Psoriasis is labeled autoimmune, but in Jacob's view the immune activity is largely a response to nerve-driven keratinocyte hyperproliferation and the resulting tissue signals, more cleanup and amplification than a random attack on self, consistent with his antibodies-as-cleanup framing.
Either way, the practical lesson is the same.
Calm the nerve and the stress driving it, and you take pressure off the immune loop.
What Helps
The full natural protocol is in the dedicated psoriasis reversal post, so this section focuses on the neuroimmune levers.
1. Deplete substance P with capsaicin
Topical capsaicin depletes substance P from cutaneous nerves with repeated use and has shown benefit in psoriasis, though the initial burning limits tolerability.
2. Calm the nerve and the stress driver
Because stress and neuropeptides drive the plaque, nervous-system work is mechanistically central, covered in the JD chapter on limbic retraining.
3. Reduce mast cell and neurogenic inflammation
Mast cell stabilizers like quercetin and luteolin, and anti-inflammatory compounds like curcumin, target the shared inflammatory machinery.
4. Support vitamin D and resolve the gut
Vitamin D signaling is central to psoriasis (topical vitamin D analogs are standard care), and addressing gut-driven inflammation reduces systemic IL-17 pressure.
5. Consider medical neuro-immune options
For resistant disease, IL-17 and IL-23 biologics are highly effective, and botulinum toxin, which reduces substance P and CGRP nerve signaling, has shown benefit in most trials and is an emerging neuroimmune option. R
Testing
Testing addresses both the disease and its well-known comorbidities.
Blood And Urine Markers
Psoriasis is a systemic inflammatory disease linked to metabolic syndrome and cardiovascular risk, so inflammatory and metabolic markers matter beyond the skin.
Vitamin D, fasting insulin, lipids, and inflammatory markers are the highest-yield.
I use the Cardio Zoomer (Vibrant Wellness) for the metabolic and cardiovascular comorbidity picture and the Nutrient Zoomer (Vibrant Wellness) for vitamin D status.
Functional Lab Panels
Because gut inflammation feeds the IL-17 axis, I use the Gut Zoomer (Vibrant Wellness), and the Immune Zoomer (Vibrant Wellness) for the broader inflammatory and autoimmune picture.
Mechanisms Of Action
Simple:
- Psoriasis is driven by both the immune system and the nerves in the skin, and the nerves often start the process that the immune system then amplifies.
- The clearest proof is that when a nerve to a psoriasis patch is damaged, the patch usually clears.
Advanced:
- IL-23/IL-17 amplification. Dendritic-cell IL-23 drives Th17 IL-17 production, which stimulates keratinocyte hyperproliferation and chemokine output (CCL20), recruiting more Th17 cells and DCs in a self-sustaining loop. R
- Neuropeptide drive. Substance P (chemotactic, T-cell-activating, Th17-promoting via NK-1R), CGRP (vasodilator, keratinocyte mitogen synergizing with SP), and VIP (endothelial mitogen) are elevated in lesional skin and feed the immune loop from the top. R
- NGF as master neuro-driver. Elevated keratinocyte NGF, with upregulated TrkA and p75NTR on lesional nerves, drives keratinocyte proliferation, neuropeptide upregulation, RANTES and ICAM-1 induction, mast cell degranulation, and angiogenesis. R
- Denervation evidence. Sensory nerve injury clears lesions in human case series and reduces dendritic cells, acanthosis, IL-23, and T cells in mouse models in a neuropeptide-dependent manner, establishing nerves as causal. R
Genetics
Psoriasis is highly heritable.
HLA-C
The HLA-C*06:02 allele (the PSORS1 locus) is by far the strongest genetic risk factor for psoriasis, especially early-onset and guttate forms.
IL23R And IL12B
These genes encode components of the IL-23 pathway, the central immune driver; the protective IL23R R381Q variant (rs11209026) and the IL12B variant rs3212227 modulate psoriasis risk and biologic response.
CARD14
CARD14 variants drive keratinocyte NF-kB activation and are a cause of familial psoriasis, linking the keratinocyte directly to the inflammatory cascade.
NGF And NTRK1
NGF and its receptor TrkA, central to the neurogenic layer, modulate the nerve-keratinocyte signaling that drives lesions.
More Research
A few additional threads are worth following.
Botulinum toxin's benefit in psoriasis is mechanistically revealing, since it works by reducing substance P and CGRP nerve signaling rather than by immunosuppression, which supports the neurogenic model directly. R
The blunted cortisol response in stress-reactive psoriasis suggests the problem is a dysregulated stress axis rather than simply high cortisol, which is why supporting a healthy cortisol rhythm matters more than blanket cortisol suppression. R
Psoriatic arthritis shares this neuro-immune biology, with elevated substance P and NGF in the joint fluid, suggesting the same mechanism extends beyond the skin. R
For the full natural protocol see the psoriasis reversal post, and for the broader framework, the brain-skin axis pillar.
For biomarker testing I use the Cardio Zoomer and Gut Zoomer to assess the metabolic comorbidities and gut drivers of psoriasis.
If you have psoriasis and want help addressing the upstream neuroimmune drivers, reach out for a consultation.
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Quercetin
500mg 2x/day
Vitamin D3 + K2
5000 IU + 200mcg/day
DAO Enzyme
1 cap before meals