Cold Exposure Therapy: Ice Baths, Cold Plunges, And Deliberate Cold Stress
By Jacob Gordon, INHC, FMT-CCold exposure therapy is one of the most potent hormetic stress interventions available, yet most people never get cold enough to trigger the biological response that matters.
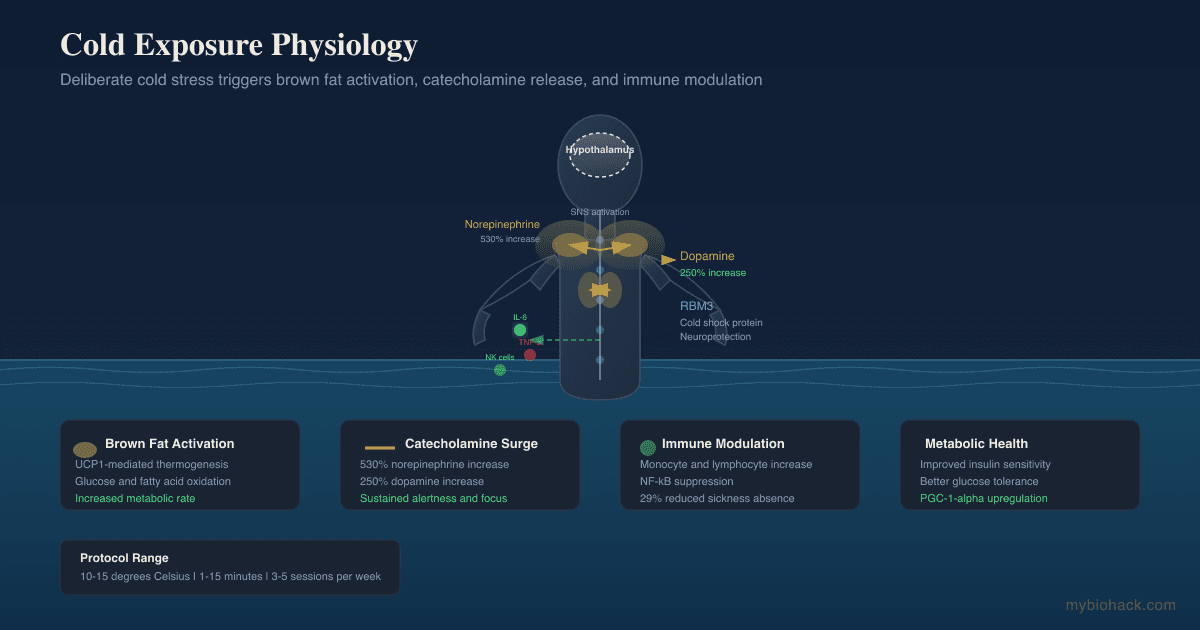
In this post, we will discuss how deliberate cold exposure works at a mechanistic level, what the research shows for brown fat activation, catecholamine release, immune modulation, and metabolic health, how to practice it safely (including for debilitated and mast cell sensitive patients), and the genetics that determine who gets the most from it.

Basics Of Cold Exposure Therapy
Deliberate cold exposure is the practice of intentionally subjecting the body to cold stress for a defined period to trigger adaptive physiological responses.
The core principle is hormesis: a controlled stressor that briefly disrupts homeostasis, followed by a compensatory adaptation that leaves the system more resilient than before R.
I covered the broader concept of hormetic stress in How Hormesis Works.
Cold exposure triggers two categories of response depending on intensity and duration.
The cold shock response occurs immediately on immersion in water below 15 degrees Celsius and includes gasping, hyperventilation, tachycardia, and peripheral vasoconstriction R.
The adaptive response unfolds over minutes to hours and includes the release of catecholamines, activation of brown adipose tissue (BAT) thermogenesis, and upregulation of cold shock proteins R.
Cold exposure therapy can be delivered through cold showers, cold water immersion (ice baths, plunges, wild swimming), whole-body cryotherapy chambers, or ambient cold exposure (cool rooms, cold air exposure).
The most studied and practical method is cold water immersion at 10 to 15 degrees Celsius for durations of 1 to 15 minutes R.
The Wim Hof Method combines cold exposure with cyclic hyperventilation and meditation, and a 2025 semi-randomized controlled trial in 404 participants found it produced greater improvements in energy, mental clarity, and perceived ability to handle stress compared to mindfulness meditation alone R.
Benefits Of Cold Exposure
The following benefits are supported by human research.
Evidence quality ranges from replicated RCTs to preliminary mechanistic studies, noted case by case.
1. Catecholamine Surge (Norepinephrine And Dopamine)
Cold water immersion at 14 degrees Celsius for one hour increases plasma norepinephrine by 530 percent and dopamine by 250 percent R.
These increases begin within minutes of immersion and persist for hours after rewarming, without the crash seen with stimulant drugs R.
Regular cold exposure maintains this norepinephrine response over weeks, showing no habituation of the sympathetic response R.
The practical effect is sustained alertness, focus, and elevated mood for two to four hours post exposure.
2. Brown Fat Activation And Metabolic Rate
Cold exposure is the most potent physiological activator of brown adipose tissue (BAT) in humans R.
BAT burns glucose and fatty acids to produce heat through uncoupling protein 1 (UCP1), a process called non-shivering thermogenesis R.

A 10-day cold acclimation protocol (14 to 15 degrees Celsius, 6 hours per day) significantly increased BAT activity and was associated with improved insulin sensitivity in lean, obese, and type 2 diabetic subjects R.
Cold acclimation with shivering (1 hour per day for 10 days) improved oral glucose tolerance, fasting glucose, triglycerides, and blood pressure in overweight and obese individuals R.
3. Immune Modulation
Repeated cold water immersion (1 hour at 14 degrees Celsius, three times per week for six weeks) increased the proportion of monocytes, lymphocytes with IL-2 receptors, and plasma tumor necrosis factor alpha, suggesting a mild activation of the immune system R.
A 2025 systematic review and meta-analysis found a 29 percent reduction in sickness absence among participants who took cold showers, although the effect on immune function immediately after exposure was not significant R.
The acute cold shock response increases circulating lymphocytes and natural killer cells, though these effects are transient and the clinical significance for infection resistance remains debated R.
4. Anti-Inflammatory Effects
Cold water immersion (14 degrees Celsius for 10 minutes) decreased TNF-alpha levels and produced a delayed increase in IL-6, consistent with an anti-inflammatory cytokine shift R.
The mechanism involves norepinephrine and cortisol suppressing NF-kB activation, which reduces transcription of pro-inflammatory cytokines R.
Post exercise cold water immersion blunted the rise of IL-6 and TNF-alpha compared to passive recovery, though this may also attenuate the adaptive signaling that drives muscle hypertrophy (discussed below in Safety) R.
5. Neuroprotection Via Cold Shock Proteins
Cold exposure upregulates RNA-binding motif 3 (RBM3), a cold shock protein that is highly neuroprotective in both in vitro and in vivo models R.
RBM3 expression is induced by moderate hypothermia (33.5 degrees Celsius) and protects neurons from hypoxia-induced cell death R.
The mechanism involves alternative splicing regulation: cold temperature represses the inclusion of a poison exon in RBM3 mRNA, increasing functional protein production R.
This is a promising but early area of research, with most data coming from animal and cell models.
6. Improved Insulin Sensitivity And Glucose Metabolism
Cold exposure improves whole-body insulin sensitivity through mechanisms that extend beyond BAT activation R.
Skeletal muscle glucose uptake increases during cold exposure via AMPK-dependent and contraction-independent pathways R.
A 2024 Nature Metabolism study found that 10 days of cold acclimation with shivering improved oral glucose tolerance, fasting glucose, and metabolic markers in overweight and prediabetic individuals R.
One note of caution: daily brief cold water immersion (10 minutes at 14 degrees Celsius for 16 days) temporarily decreased glucose tolerance and insulin sensitivity in young non-obese adults, though values returned to baseline after one week without exposure R.
This suggests the metabolic effects of cold exposure depend on duration, frequency, and individual metabolic status, and a brief daily protocol may not replicate the benefits of longer acclimation protocols.
7. Stress Resilience And Mood
Cold water immersion produced a significant reduction in self-reported stress at 12 hours post exposure in a 2025 meta-analysis, though no significant effects were observed immediately, at 1 hour, or at 24 hours R.
The Wim Hof Method trial found cumulative dose-dependent improvements in self-reported energy, mental clarity, and ability to handle stress over 29 days, with effects increasing across the protocol while the meditation control group's effects decreased R.
How To Do Cold Exposure
There is no single correct protocol.
The right approach depends on your health status, tolerance, and goals.
What follows is a tiered system from lowest to highest intensity.
For Debilitated Patients And Beginners
Start with cold showers, not full immersion.
End your warm shower with 30 seconds of cold water directed at your legs and feet.
Increase to 60 seconds over the first week, then add the torso and arms.
Target water temperature that feels cold but does not trigger severe shock (15 to 20 degrees Celsius from a tap is usually sufficient).
Progress to 90 seconds to 2 minutes before attempting full immersion.
The goal is to trigger the catecholamine response without overwhelming the nervous system.
Standard Cold Plunge Protocol
Water temperature: 10 to 15 degrees Celsius.
Duration: 1 to 5 minutes per session, 3 to 5 sessions per week.
Start at the warmer end (15 degrees) and shorter duration (1 minute) and increase as tolerance builds.
Enter the water slowly and control your breathing.
The initial gasping reflex passes within 30 to 60 seconds.
The commonly cited dose of approximately 11 minutes of total cold exposure per week (spread across 2 to 4 sessions) is a reasonable target for general health benefits R.
Wim Hof Method
The Wim Hof Method has three pillars: breathing, cold exposure, and commitment (meditation/focus).
The breathing component involves 30 to 40 rapid deep breaths followed by a breath hold after exhalation, repeated for 3 to 4 rounds.
Cold exposure in the WHM context is typically a 2 to 3 minute cold plunge or cold shower immediately following the breathing exercise.
The method has demonstrated safety in healthy adults in clinical trial settings with 404 participants R.
When To Cold Expose
Morning cold exposure is preferable for most people because the catecholamine surge supports alertness and focus for the workday ahead.
Cold exposure after resistance training may attenuate hypertrophy signaling and is not recommended if muscle growth is your primary goal R.
The 2025 PLOS One meta-analysis found stress reduction was most pronounced at 12 hours post exposure, suggesting afternoon cold immersion may improve evening wind-down R.
Contrast With Heat Exposure
Cold and heat stress produce overlapping but distinct biological responses.
Heat stress (sauna) activates heat shock proteins and vasodilation, while cold stress activates cold shock proteins (RBM3) and vasoconstriction.
I covered the dose ceiling phenomenon in Red Light Therapy Has A Dose Ceiling, which also applies to cold: more is not always better, and the goal is the minimum effective dose that triggers adaptation.
Safety And Contraindications
Cold exposure is safe for most healthy adults when practiced responsibly, but it carries real risks.
Absolute Contraindications
Cardiovascular disease, including unstable angina, recent myocardial infarction, heart failure, and uncontrolled hypertension.
The cold shock response causes acute vasoconstriction and increased cardiac workload, which can trigger ischemic events R.
Pregnancy (cold stress can reduce uterine blood flow).
Raynaud's phenomenon and cold urticaria (hives triggered by cold).
Severe peripheral vascular disease.
Cold, Mast Cells, And Histamine: A Critical Caution
Cold exposure activates mast cells.
This is a physiological response, not a pathology in everyone.
Research shows that norepinephrine released during cold exposure directly stimulates mast cell degranulation and histamine release R.
Cold-induced adipose tissue beiging in humans is mediated in part by mast cell recruitment and degranulation, meaning the process is mechanistically linked R.
For people with Mast Cell Activation Syndrome (MCAS) or histamine intolerance, cold exposure can trigger flushing, urticaria, gastrointestinal symptoms, and even anaphylactoid reactions R.
A 2021 case series identified that severe cold urticaria can indicate an underlying clonal mast cell disorder requiring further workup R.
Cluster analysis of MCAS patients found physical triggers (including cold) as a distinct subtype with specific symptom patterns R.
If you have MCAS or suspected histamine intolerance, start with brief cold exposure (30 seconds at 15 degrees Celsius) under medical supervision and monitor symptom response.
I covered the distinction between MCAS and histamine intolerance in Histamine Intolerance vs MCAS and the nerve-mast cell connection in Mast Cells, Substance P, And Neurogenic Inflammation.
Post Exercise Timing
Cold water immersion immediately after resistance training attenuates anabolic signaling, reduces satellite cell activity, and blunts long-term muscle hypertrophy R.
If muscle growth is a priority, separate cold exposure from resistance training by at least 4 to 6 hours, or skip post workout immersion entirely.
Testing
There are no standard clinical tests for cold exposure tolerance or adaptation, but several biomarkers can help determine baseline metabolic health and monitor response.
Blood And Urine Markers
- Fasting glucose and fasting insulin: these markers reflect baseline insulin sensitivity, which cold exposure may improve. I use the Cardio Zoomer to assess metabolic markers including insulin and glucose.
- High-sensitivity C-Reactive Protein (hs-CRP): a systemic inflammation marker that may decrease with regular cold adaptation. The Cardio Zoomer includes hs-CRP.
- Norepinephrine and dopamine: plasma levels of these catecholamines increase acutely with cold exposure, but single measurements are not clinically useful for diagnosis.
- Tryptase: a mast cell activation marker. Baseline tryptase is useful before starting cold exposure if MCAS is suspected. I use the Immune Zoomer to assess mast cell and immune markers.
Functional Lab Panels
I use the Cardio Zoomer to assess metabolic, lipid, and inflammatory markers that provide baseline context for cold exposure therapy.
For those with suspected mast cell involvement, the Immune Zoomer provides a comprehensive assessment including mast cell markers and systemic autoantibodies.
Contraindication Screening
Before starting cold exposure therapy, rule out cardiovascular risk factors with a comprehensive metabolic assessment.
I use the Foundation Zoomer for CBC, CMP, thyroid, and immune baselines, and the Cardio Zoomer for advanced lipid and metabolic profiling.
Mechanisms Of Action
Simple:
- Cold exposure activates the sympathetic nervous system, flooding the body with norepinephrine and dopamine that increase alertness, focus, and metabolic rate.
- Cold stress triggers brown fat to burn glucose and fat for heat, a process that improves insulin sensitivity and increases energy expenditure.
- Cold exposure induces cold shock proteins that protect neurons and reduce inflammatory signaling through NF-kB suppression.
Advanced:
- Catecholamine Release: Cold water immersion at 14 degrees Celsius activates the sympathetic adrenomedullary system, causing a 530 percent increase in plasma norepinephrine and a 250 percent increase in dopamine R. Norepinephrine binds beta-3 adrenergic receptors on brown adipocytes, activating lipolysis and UCP1-mediated thermogenesis R.
- Brown Adipose Tissue Thermogenesis: Cold exposure stimulates BAT via the beta-3 adrenergic receptor / cAMP / PKA signaling cascade, which upregulates UCP1 expression and mitochondrial uncoupling R. UCP1 dissipates the proton gradient across the inner mitochondrial membrane, converting the energy from fatty acid oxidation directly into heat rather than ATP R.
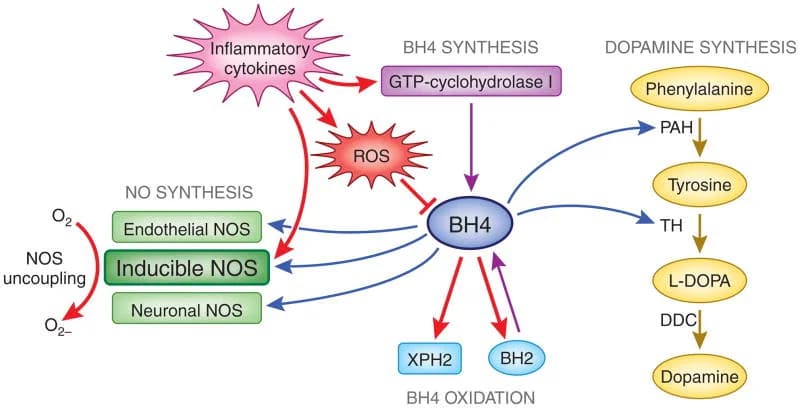
- Cold Shock Protein RBM3 Induction: Moderate hypothermia (33.5 degrees Celsius) upregulates the RNA-binding motif 3 (RBM3) protein through FAK/Src signaling and NF-kB activation R. RBM3 stabilizes synaptic proteins and promotes neuronal survival by preventing apoptosis R. The mechanism involves temperature-sensitive alternative splicing: cold represses a poison exon in RBM3 pre-mRNA that would otherwise target the transcript for nonsense-mediated decay R.
- NF-kB Suppression: Cold exposure elevates cortisol and norepinephrine, which activate glucocorticoid and beta-2 adrenergic receptors on immune cells R. This upregulates NFKBIA gene expression, increasing the IkB-alpha protein that sequesters NF-kB in the cytoplasm, reducing transcription of pro-inflammatory cytokines including IL-6, IL-1-beta, and TNF-alpha R.
- TRPM8 Cold Sensing: The transient receptor potential melastatin 8 (TRPM8) ion channel is the primary molecular sensor for non-painful cold temperatures (8 to 28 degrees Celsius) in peripheral sensory neurons R. TRPM8 activation initiates the afferent signal that drives central sympathetic outflow and BAT thermogenesis. TRPM8 agonism with menthol mimics some cold effects in animal models R.
- Peroxisome Proliferator-Activated Receptor Gamma Coactivator 1-Alpha (PGC-1-alpha): Cold exposure upregulates PGC-1-alpha in skeletal muscle and adipose tissue, driving mitochondrial biogenesis and oxidative metabolism R. PGC-1-alpha is a master regulator of the adaptive response to cold and a key node linking cold exposure to improved metabolic health.
- Fibroblast Growth Factor 21 (FGF21): Cold exposure increases circulating FGF21, a batokine secreted by activated brown adipocytes that promotes thermogenesis through both UCP1-dependent and UCP1-independent mechanisms R. FGF21 also drives hepatic lipid oxidation and ketogenesis.
Genetics
Genetic variation in cold-sensing, thermogenic, and catecholamine pathways significantly influences individual response to cold exposure therapy.
UCP1: Highest Population Risk
The UCP1 gene encodes Uncoupling Protein 1, the mitochondrial protein responsible for thermogenesis in brown adipose tissue R.
The rs1800592 (-3826 A to G) promoter variant reduces UCP1 expression and diminishes cold-induced thermogenesis R.
Children homozygous for the G allele (GG) showed significantly lower cold-induced thermogenesis compared to AA and AG carriers, despite having a higher autonomic response R.
A 2017 study across 40 kb of the UCP1 region found that haplotype variation alters non-shivering thermogenesis efficiency in humans, and haplotype frequencies correlate with latitude and ambient temperature R.
Carriers of the GG genotype may need longer or more frequent cold exposure to achieve the same thermogenic response as wild-type individuals.
TRPM8
The TRPM8 gene encodes the Transient Receptor Potential Melastatin 8 ion channel, the primary cold sensor in peripheral sensory neurons R.
rs11562975 (L250L, G to C): approximately 20 percent of individuals in studied populations carry the C-allele R.
Heterozygous carriers (GC) have increased cold sensation but a hypometabolic response to skin cooling, including decreased total metabolism, pulmonary ventilation, and oxygen extraction R.
Homozygous GG individuals have lower cold sensation and an appropriate thermoregulatory response to cooling (decreased respiratory heat loss, increased lipid metabolism) R.
rs10166942: this TRPM8 variant is associated with chronic migraine and allodynia, and T-allele carriers may have altered cold pain thresholds R.
BDNF
The Brain-Derived Neurotrophic Factor (BDNF) gene is relevant because BDNF is released in response to cold stress and is critical for synaptic plasticity R.
The Val66Met (rs6265) polymorphism reduces activity-dependent BDNF secretion and is associated with impaired cognitive flexibility and stress resilience.
ADRB3
The Beta-3 Adrenergic Receptor (ADRB3) mediates the effect of norepinephrine on brown adipocytes.
The Trp64Arg (rs4994) variant reduces ADRB3 sensitivity to catecholamines and is associated with lower BAT activity and increased obesity risk.
More Research

- Cold exposure and the glymphatic system. The sympathetic activation and norepinephrine surge from cold exposure may influence glymphatic clearance. I covered the glymphatic system and AQP4 in How To Improve Your Glymphatic System And AQP4. The intersection between cold-induced sympathetic outflow and CSF dynamics is underexplored but mechanistically plausible.
- Cold exposure for internal tremors and body buzzing. The norepinephrine and dopamine surge from cold exposure may temporarily modulate the sensory-motor disturbances in conditions like internal tremors. I covered this phenomenon in Body Buzzing And Internal Tremors. Some patients report transient relief from cold showers, though no systematic data exist.
- Cold exposure and mitochondrial psychobiology. The PGC-1-alpha and mitochondrial biogenesis effects of cold exposure connect directly to the mind-mitochondria axis. I covered this in Mitochondrial Psychobiology. Cold stress increases mitochondrial density in muscle and adipose tissue, and the cellular energy-sensing pathways activated by cold overlap with those involved in mood and cognition.
- The minimum effective dose for cold adaptation. Most cold exposure research uses protocols ranging from 10 minutes to 2 hours. The practical question for most people is whether shorter durations (1 to 3 minutes) produce meaningful adaptation. The 2025 PLOS One meta-analysis included studies with durations as short as 30 seconds and found time-dependent effects on inflammation and stress, but the optimal dose-response curve remains undefined R.
- Cold habituation versus cold adaptation. Regular cold exposure produces habituation of the cold shock response (reduced gasping, lower heart rate spike) within 2 to 3 weeks R. Metabolic adaptation (increased BAT activity, non-shivering thermogenesis) takes longer and may require lower temperatures or longer durations. These are distinct processes with different time courses and different implications for protocol design.
- The mast cell paradox. Cold exposure both activates mast cells (necessary for adipose beiging) and suppresses inflammatory cytokine production R. For most people this balance is beneficial. For those with MCAS, the activation side can dominate, producing symptom flares rather than adaptation. Individual mast cell stability determines which direction the balance tilts. For biomarker testing I use the Immune Zoomer to assess mast cell and immune status before starting cold exposure therapy.
- Cold versus heat stress. Cold and heat produce overlapping but not identical adaptations. Heat stress upregulates heat shock proteins (HSP70, HSP90) and promotes vasodilation and nitric oxide production. Cold stress upregulates RBM3 and promotes vasoconstriction and norepinephrine release. Some evidence suggests alternating cold and heat exposure (contrast therapy) produces distinct vascular and neuroendocrine effects not seen with either alone.
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Lion's Mane
1000mg/day
Omega-3 (DHA)
2g/day
Phosphatidylserine
100mg 3x/day