Red Light Therapy Has A Dose Ceiling: Why More Light Eventually Shuts Your Cells Down
By Jacob Gordon, INHC, FMT-CThis article contains affiliate links. As an Amazon Associate, MyBioHack earns from qualifying purchases at no extra cost to you. We only link products we research and stand behind.
Red light therapy works through a real molecular target inside your mitochondria, and the benefit follows a curve that rises to a peak and then falls back below zero.
In this post, we will discuss how red and near-infrared light actually works, why more is not better, the four variables that decide whether a session helps or hurts, and where this fits for people with broken redox systems.

Basics Of Red Light Therapy
Photobiomodulation (PBM), the technical name for red light therapy, is the use of red and near-infrared light to change how cells behave without heating or cutting tissue.
The older name was Low-Level Laser Therapy (LLLT), from the era when the field used lasers instead of LED panels.
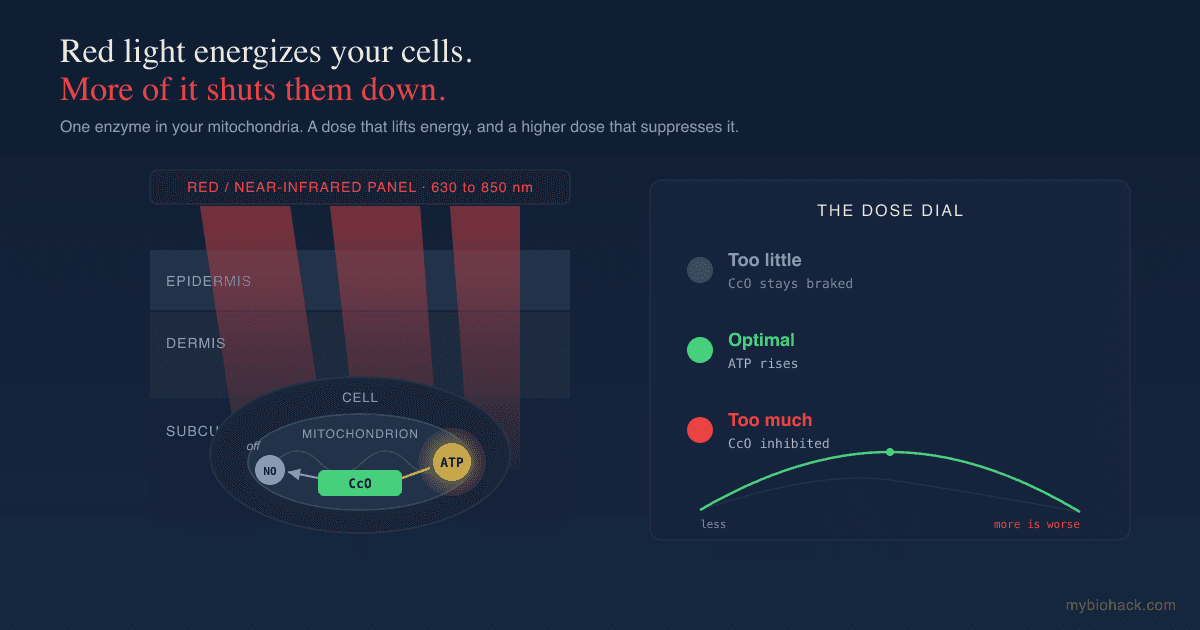
The light sits in a narrow band, roughly 600 to 850 nanometers, that the field calls the optical window because it passes through skin better than other wavelengths.
Red light around 630 to 660 nanometers is absorbed shallowly and acts mostly on skin.
Near-infrared light around 810 to 850 nanometers penetrates deeper, on the order of several millimeters, which is why it is used on joints, muscle, and the head. R
The single most important fact about this therapy is not that it works, but that it has a ceiling, and most people walk straight past it.
How Red Light Actually Works
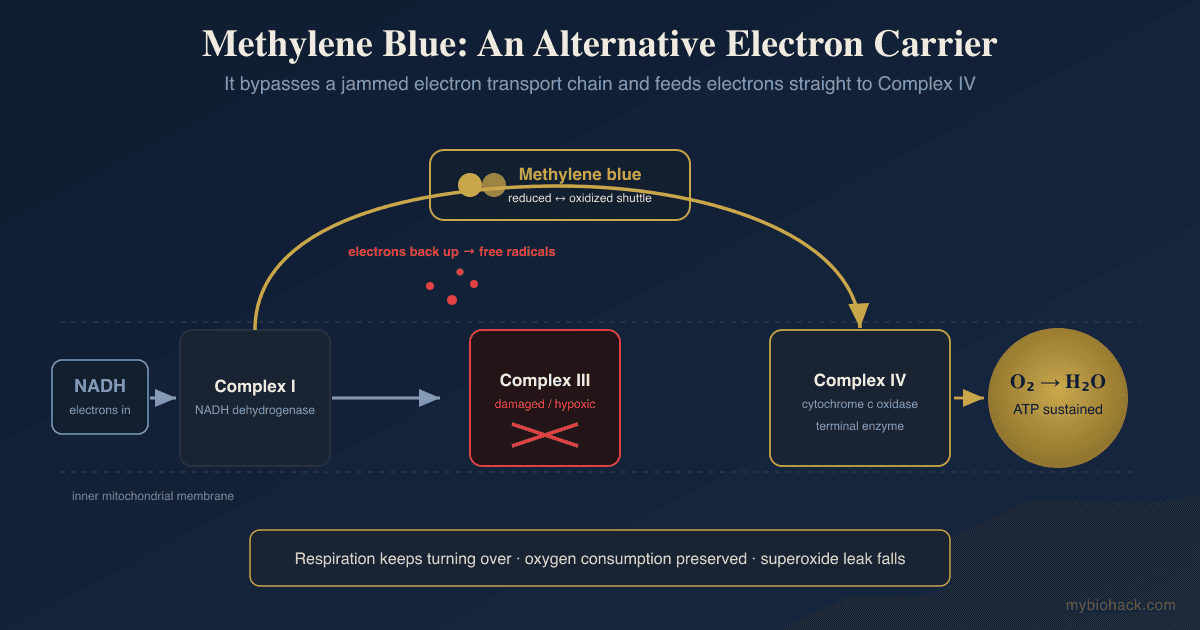
The main molecule that absorbs red and near-infrared light inside the cell is cytochrome c oxidase (CcO), the fourth and final enzyme in the mitochondrial electron transport chain. R
CcO is where electrons finally meet oxygen to make water, the step that drives most of your ATP production.
The widely accepted account is that the light knocks a molecule of inhibitory nitric oxide (NO) off cytochrome c oxidase. R
Nitric oxide can sit on that enzyme and act as a brake, competing with oxygen at the same binding site.
When light dissociates that nitric oxide, the brake comes off, electrons flow faster, oxygen consumption rises, and ATP output climbs.
That single step, more available cellular energy, is the engine behind the wound healing, pain relief, and skin effects the therapy is used for. R
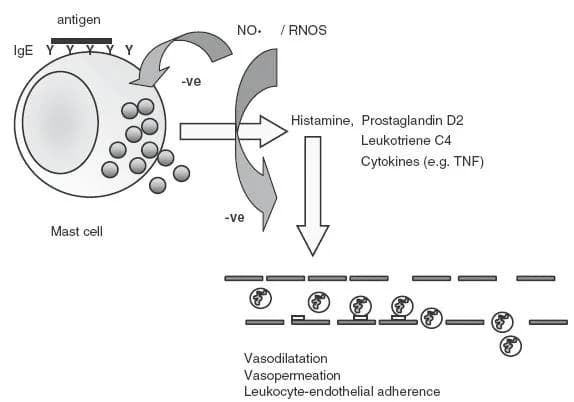
A second wave of effects follows the energy bump, including a brief burst of reactive oxygen species, a rise in nitric oxide, and shifts in calcium signaling, all of which act as messengers that switch on protective genes. R
So the mechanism is not mystical, and it is not heat.
It is one enzyme, one released brake, and a cascade of signaling that follows.
The Biphasic Dose Response
The organizing principle of this entire field is that the dose response is biphasic, meaning the benefit climbs to a peak and then reverses.
This pattern is reproduced often enough to have a name, the Arndt-Schulz curve, after the old pharmacology observation that low doses stimulate and high doses inhibit. R
Low doses of red light stimulate and repair tissue.
Higher doses of the exact same light have an inhibitory effect.
The relationship between dose and result is an arch, not a ladder, so the benefit rises to an optimum and then falls back toward zero and below.
This has been shown for the downstream markers themselves, where ATP and mitochondrial membrane potential rise and then fall as the dose increases. R
The practical translation is uncomfortable for anyone selling brighter devices.
Past the optimal dose, the same light that was raising a cell's energy output starts shutting it down.

Why The High End Turns Inhibitory
The reason the high end turns inhibitory is not actually settled, and it is worth being precise here rather than inventing a clean mechanism.
The leading explanations are too much reactive oxygen species, too much nitric oxide, and overdriving the very signaling that was helpful at lower doses, but the field has not nailed down which one dominates. R
The reactive oxygen story is a good example of how context-dependent this is.
The same light produces a brief, useful burst of reactive oxygen species in healthy cells.
Yet in oxidatively stressed cells and in animal models of disease, the same treatment lowers reactive oxygen levels and raises antioxidant defenses. R
In other words, the cell's starting redox state can change the direction of the effect, which is exactly why a dose that helps one person can do nothing or harm in another.
There is a big MAYBE at the top of the curve, and honest sources say so instead of pretending the inhibitory zone has one tidy cause.
What The Evidence Actually Supports
This is not a reason to dismiss the therapy, because the dosing question only matters if the tool does something in the first place.
A controlled trial in 136 volunteers found that red and near-infrared treatment improved intradermal collagen density and reduced fine lines and skin roughness against a control group. R
The therapy has reasonable support for skin rejuvenation, wound healing, and certain kinds of pain and inflammation. R
It also has a growing, less settled literature for the brain, where near-infrared light is being studied for cognition and mood. R
The honest summary is that the evidence is real but uneven, and the unevenness is largely a dosing problem, not a "does it work" problem.
That is the whole point.
The literature contains so many negative trials sitting right next to the positive ones in part because the negative trials missed the window.
The Four Variables That Decide The Dose
Four variables decide whether a session lands in the helpful zone or sails past it, and a scoping review of dosage versus efficacy makes the case that getting them wrong is a large part of why results are so inconsistent. R
Wavelength decides what gets absorbed and how deep the light reaches, with red for skin and near-infrared for deeper tissue.
Intensity (irradiance, measured in milliwatts per square centimeter) is how much power lands on the tissue at a given moment.
Distance changes intensity dramatically, because moving closer to a panel raises the power hitting your skin in a nonlinear way.
Time sets the total dose (fluence, measured in joules per square centimeter), which is intensity multiplied by duration.
The failure mode is treating every one of these as "more is better."
Standing closer, running it longer, buying a brighter panel, and using it more often all push you up and over the peak toward the flat or inhibitory part of the curve.
The device is not the hard part.
The dose is.
Red Light Therapy And Junction Dysfunction
This is where the chronically ill need a different conversation than the general biohacking audience, and it follows directly from the mechanism above.
The benefit of red light runs partly on releasing nitric oxide and producing a small, controlled burst of reactive oxygen species, which is a hormetic stress that a healthy cell answers by upregulating antioxidant enzymes.
I have written before about why NRF2 activation can backfire in people whose redox systems are already overloaded, and red light is another hormetic input that follows the same logic.
If the cell cannot mount the antioxidant response, the "stimulating" dose is just more oxidative load.
There is a second, more specific concern in Junction Dysfunction (JD), the framework I use for glycocalyx and microvascular breakdown in chronic illness.
In my framing, when the cofactor tetrahydrobiopterin (BH4) is depleted, the enzyme that makes nitric oxide in your vessels uncouples, and instead of clean nitric oxide it starts producing nitric oxide alongside superoxide, which combine into peroxynitrite, a far more damaging oxidant. R
My hypothesis is that adding a nitric-oxide-releasing input like red light on top of a depleted BH4 system and a degraded glycocalyx can feed that peroxynitrite pathway rather than the clean signaling pathway, and this is my framing rather than settled science.
This is the same reason I am cautious with nitric oxide boosters in this population.
None of this means people with long COVID, POTS, or post-viral fatigue cannot use red light.
It means they should start at the bottom of the curve, support the antioxidant and methylation machinery that recycles BH4 first, and watch for crashes rather than assuming more is better.
The infrared end of the spectrum is useful for mitochondria in this group, and I keep it in my own protocol, but the dosing discipline matters more here than anywhere.
How To Dose It
The goal is to land on the helpful part of the curve and stay there, not to maximize exposure.
1. Pick the right wavelength for the target
Use red light around 630 to 660 nanometers for skin, scars, and surface wounds.
Use near-infrared around 810 to 850 nanometers for joints, deep muscle, and the head.
Many red light panels combine both bands, which is fine for general use.
2. Respect the manufacturer's distance and time
Follow the irradiance and distance the manufacturer specifies for a given session length, because that is where they measured the dose.
Standing closer to feel like you are getting more is the single easiest way to overshoot the peak.
3. Keep sessions short
A few minutes per area is typically enough at panel-level irradiance, not twenty.
If you respond well, the answer is not to double the time.
4. Dose in the daytime
Red and near-infrared exposure in the morning or midday stacks with natural sunlight and supports your circadian rhythm.
Sunlight is the original infrared source, and a device is a supplement to it, not a replacement.
5. Start low if you are chronically ill
If you have post-viral illness, mast cell issues, or known redox problems, begin with the shortest sessions and the greatest distance, then increase slowly only if you tolerate it.
Pair it with NRF2 and BH4 support so the hormetic signal has somewhere to go.
What To Stay Away From
Chasing brightness (the brighter-panel arms race): a higher-output device makes it easier to overshoot the optimal dose, not easier to get results.
Long sessions: doubling the time does not double the benefit, and past the peak it reverses it.
Standing too close: distance changes intensity nonlinearly, so creeping closer quietly multiplies your dose.
Thermal devices marketed as red light: if the panel mainly heats you, you are getting a heat lamp effect, not photobiomodulation, and heat has its own separate risks.
Unprotected eyes under high-power near-infrared: use the eye protection the manufacturer provides for direct facial or transcranial use.
Stacking with nitric oxide boosters in the JD population: combining red light with L-arginine or other nitric oxide boosters when your BH4 and antioxidant systems are depleted compounds the peroxynitrite risk described above.
Testing
Most people do not need a lab to use red light sensibly, but if you want to personalize the dose, the relevant thing to measure is your redox and mitochondrial status, not the light itself.
Functional Lab Panels
I use the Cellular Zoomer (Vibrant Wellness) to assess organic acids, mitochondrial function, oxidative stress, and methylation markers, which together tell you whether your antioxidant machinery can actually answer a hormetic input like red light.
Markers of oxidative damage on this kind of panel are what would tip you off that you are adding stress faster than you can clear it.
Genetics
A redox-focused genetic panel that includes the variants below tells you in advance whether you are likely to need more antioxidant and BH4 support before leaning on hormetic light.
Mechanisms Of Action
Simple:
- Red and near-infrared light is absorbed by one enzyme in your mitochondria, knocks an inhibitory molecule off it, and lets your cells make more energy, but only up to a point, after which the same light slows them down.
Advanced:
- Cytochrome c oxidase photoreception: CcO contains copper and heme centers that absorb photons in the red and near-infrared bands, which is why the action spectrum for the biological effect tracks the absorption spectrum of the enzyme. R
- Nitric oxide photodissociation: the photons disrupt the weak non-covalent bonds holding inhibitory nitric oxide on CcO, releasing it, restoring electron flow, raising the proton gradient, and increasing ATP synthesis. R
- Secondary signaling: the resulting brief reactive oxygen species burst, nitric oxide release, and calcium flux act as second messengers that activate transcription factors and shift cells toward survival, proliferation, and reduced inflammation. R
- Biphasic reversal: above the optimal fluence, the same mediators overshoot, with excess reactive oxygen species and nitric oxide proposed as the drivers of the inhibitory phase, though the dominant mechanism is not settled. R
- Redox context dependence: in oxidatively stressed cells the same dose lowers reactive oxygen species and raises antioxidant defenses, so baseline redox state changes the sign of the response. R
Genetics
NOS3
NOS3 encodes endothelial nitric oxide synthase, the enzyme that produces nitric oxide in your blood vessels.
Variants change how much nitric oxide you make and how readily the enzyme uncouples under cofactor stress.
rs1799983 (Glu298Asp) is associated with reduced nitric oxide availability and endothelial function, which is relevant to how a nitric-oxide-releasing input behaves in you. R
SOD2
SOD2 encodes manganese superoxide dismutase, the mitochondrial enzyme that quenches the superoxide produced inside mitochondria.
A weaker enzyme means a brief reactive oxygen species burst is cleared less efficiently.
rs4880 (Ala16Val) alters how the enzyme is imported into mitochondria and is the variant I see most often in clients with redox imbalances, which is one reason hormetic doses need to start low. R
mtDNA
Mitochondrial DNA haplogroups carry sequence differences in the cytochrome c oxidase subunits themselves.
This could plausibly change how efficiently a given person responds to red light, but the human data here are preliminary and I would not make decisions on it yet.
More Research
Continuous versus pulsed delivery is still unsettled, with some evidence that pulsing changes the effective dose, which adds another variable on top of the four above. R
Industry conflicts of interest are worth naming, because several widely cited reviews in this space are authored by researchers who disclose financial ties to device makers, and the right response is to lean on the findings that replicate across independent groups, where the biphasic curve holds regardless of who funded the work. R
Systemic effects beyond the treated area are reported, where light on one region appears to influence distant tissue through circulating mediators, but the magnitude and reliability are not yet clear.
For redox and mitochondrial testing I use the Cellular Zoomer (Vibrant Wellness) to decide whether someone's antioxidant systems can handle hormetic inputs before adding them.
The deeper mechanistic question for the chronically ill, which is whether a nitric-oxide-releasing therapy helps or feeds the peroxynitrite pathway in a depleted BH4 system, is the part I am most interested in and the part the literature has not addressed.
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Quercetin
500mg 2x/day
SPM Active (Pro-resolving Mediators)
2 softgels/day
Curcumin (Liposomal)
500mg 2x/day