9 Benefits Of Methylene Blue: The Mitochondrial Electron Carrier And The Safety Line Most Biohackers Cross
By Jacob Gordon, INHC, FMT-CThis article contains affiliate links. As an Amazon Associate, MyBioHack earns from qualifying purchases at no extra cost to you. We only link products we research and stand behind.
Methylene blue is a century-old synthetic dye that doubles as an alternative mitochondrial electron carrier, and it lives on a narrow dose window where a little helps and a little more hurts.
In this post, we will discuss what methylene blue actually does inside the mitochondria, its effects on the brain, the near-infrared light synergy, the hormetic dose ceiling, and the three safety lines (serotonin syndrome, G6PD hemolysis, and product grade) that most biohackers cross.

What Is Methylene Blue
Methylene blue (MB) is a phenothiazine dye first synthesized in 1876 and the first fully synthetic compound ever used as a drug in humans. R
It is a redox-active molecule, meaning it can accept and donate electrons by cycling between an oxidized blue form and a reduced colorless form called leucomethylene blue. R
That single property is the whole story.
MB slips into the mitochondria and inserts itself directly into the electron transport chain (ETC), where it can pick up electrons from nicotinamide adenine dinucleotide (NADH) and hand them off further down the line, acting as a shuttle that keeps energy production moving. R
It is also the standard, FDA-approved antidote for acquired methemoglobinemia, which is the clinical use most doctors know it for. R
Everything the biohacking world is interested in (cognition, energy, longevity signaling) flows downstream from that electron-carrier behavior, and every danger flows from the fact that the same molecule does the opposite job at higher concentrations.
Benefits Of Methylene Blue
The benefits below are ranked by how well the mechanism is established, not by how exciting they sound.
Most human cognitive data is small and acute, and that caveat applies to nearly everything in this list.
1. It Rescues Mitochondrial Respiration As An Alternative Electron Carrier
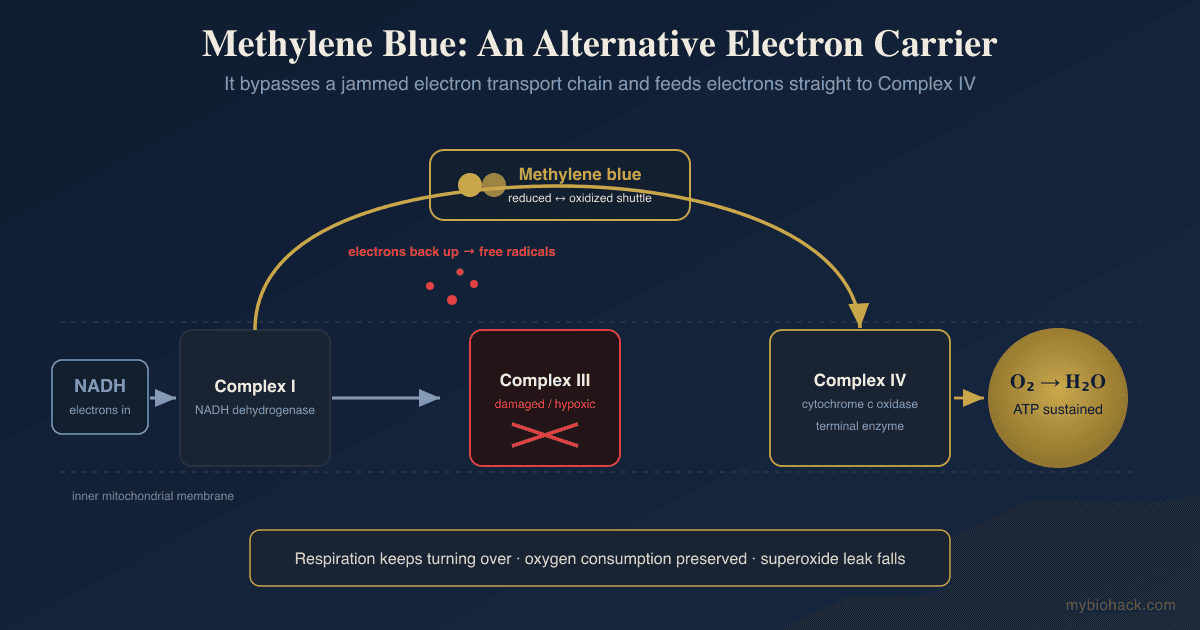
The defining benefit of MB is that it bypasses upstream bottlenecks in the electron transport chain. R
In a healthy cell, electrons flow Complex I to Complex III to Complex IV.
When Complex I or Complex III is damaged, sluggish, or hypoxic, electrons back up and spill out as free radicals.
MB reroutes traffic around the jam by accepting electrons from NADH and donating them straight to cytochrome c oxidase (Complex IV), the terminal enzyme that hands electrons to oxygen. R
This is why MB is described as an alternative electron transfer strategy for neuroprotection rather than just another antioxidant. R
In cultured human fibroblasts, low-nanomolar MB raised Complex IV activity by about 30% and cellular oxygen consumption by 37 to 70%. R
2. It Increases Cytochrome C Oxidase Activity And Brain Metabolism
Cytochrome c oxidase is the rate-limiting enzyme of brain energy metabolism, and MB increases its activity in a dose-dependent way.
A single 1 mg/kg dose raised brain cytochrome oxidase activity by roughly 30% at 24 hours, and three repeated daily doses pushed that to about 70% above controls. R
Because memory formation is metabolically expensive, raising the ceiling on oxidative metabolism is the mechanistic basis for most of the cognitive findings that follow. R
3. It Improves Short-Term Memory And Sustained Attention In Humans
This is the benefit with actual human imaging data behind it, though it is a single acute study.
In a randomized, double-blind, placebo-controlled trial with functional MRI, a single low oral dose of MB increased the fMRI response in brain regions handling sustained attention and short-term memory, and produced a 7% increase in short-term memory retrieval. R
The effect is real but modest, it was measured one hour after a single dose, and it has not been replicated across weeks of use.
4. It Enhances Memory Consolidation And Fear Extinction
In animal work, MB reliably strengthens the consolidation phase of memory, not the encoding or retrieval phases. R
A 1 mg/kg dose restored spatial memory that had been impaired by a cytochrome oxidase inhibitor, which ties the memory benefit directly back to Complex IV. R
Low-dose MB also improved retention of fear extinction, the process that lets the brain unlearn a conditioned fear, which is why it has been studied as a metabolic adjunct for exposure-based approaches to anxiety. R
Network imaging in an amnestic model showed MB improved memory by restoring metabolic coupling across brain regions rather than acting on a single site. R
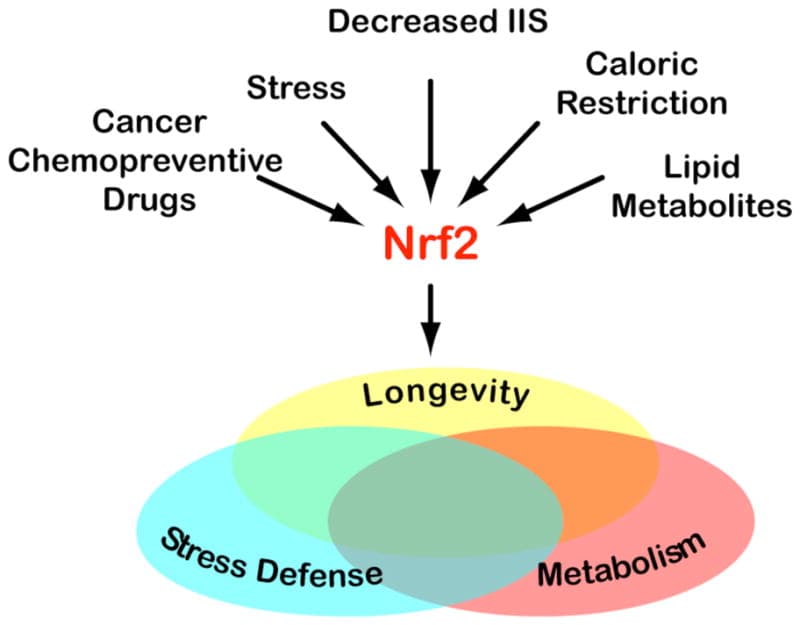
5. It Acts As A Low-Dose Antioxidant And Activates The NRF2 Pathway
At low concentration MB is a net antioxidant because it intercepts leaking electrons before they can form superoxide. R
It also upregulates Nuclear factor erythroid 2-related factor 2 (NRF2) and its downstream antioxidant response element (ARE) genes, including heme oxygenase-1, NQO1, and glutathione-related enzymes. R
This is a hormetic effect, which means it is the body's own antioxidant defense being switched on, not MB scavenging radicals one for one.
This is the same NRF2-driven hormesis that underlies why controlled stressors help resilient cells and can backfire in people with broken redox systems.
6. It Delays Cellular Senescence (A Longevity Signal)
In human IMR90 fibroblasts, MB extended replicative lifespan by more than 20 population doublings and delayed the onset of senescence at nanomolar concentrations. R
The same work showed MB reversed premature senescence triggered by hydrogen peroxide or cadmium, and the effect depended on the MB to leucomethylene blue redox cycle running inside the mitochondria. R
This is cell-culture data, not lifespan data in humans, so treat it as a promising signal and nothing more.
For the broader picture of mitochondrial longevity levers, see urolithin A and MOTS-c.
7. It Is Neuroprotective Under Hypoxia And Synergizes With Near-Infrared Light
When perfusion drops and tissue goes hypoxic, the electron transport chain stalls and free-radical output climbs, which is exactly the situation MB is built for.
In rats with chronic cerebral hypoperfusion, MB preserved cytochrome oxidase activity and prevented the neurodegeneration and memory loss that low blood flow otherwise causes. R
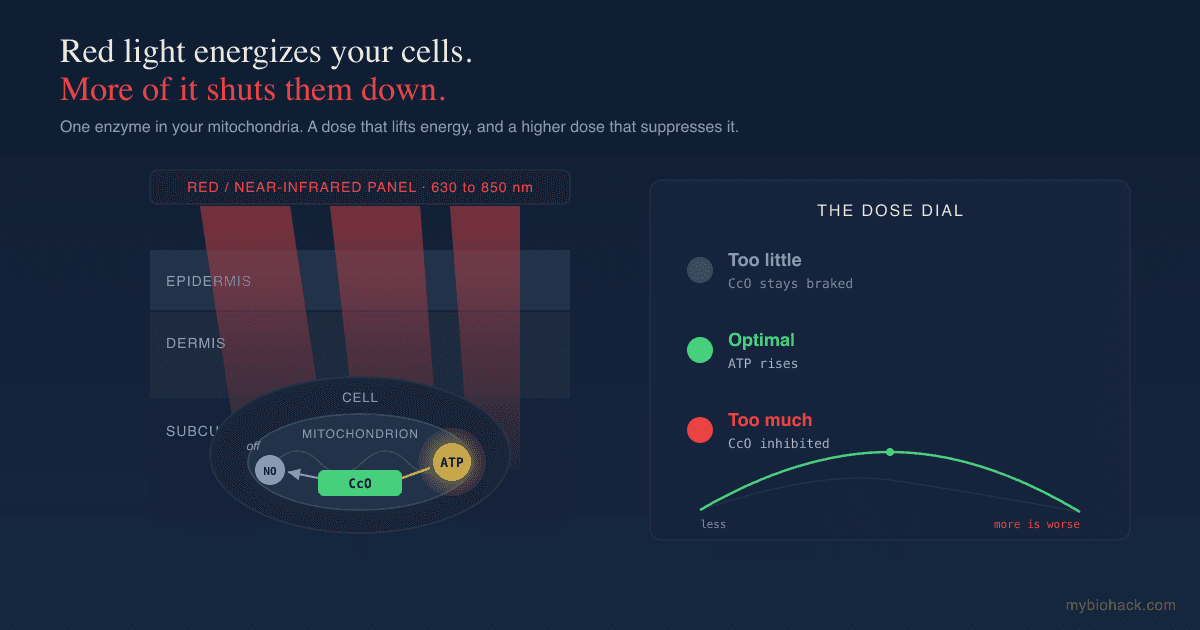
MB also stacks with near-infrared (NIR) light, because both target the same enzyme from different angles.
MB donates electrons to cytochrome c oxidase chemically, while NIR photons are absorbed by cytochrome c oxidase directly and dissociate inhibitory nitric oxide from it. R
Because both raise cytochrome oxidase activity through complementary routes, pairing MB with a red or near-infrared panel targets the same enzyme from two directions. R
This is the same cytochrome c oxidase target and the same hormetic dose ceiling covered in the red light therapy dose ceiling post, and the two interventions share a mechanism, so their dose limits stack rather than cancel.
8. It Has Antimicrobial And Antimalarial Activity
MB was the original antimalarial.
Guttmann and Ehrlich reported curing malaria patients with it in 1891, and Ehrlich's observation that MB selectively stained the parasite is where his "magic bullet" concept came from. R
It is not a historical footnote either.
Pharmaceutical-grade MB (marketed as Proveblue) retains in vitro activity against Plasmodium falciparum strains that are resistant to standard antimalarial drugs. R
MB also has broad antibacterial, antifungal, and antiviral activity in vitro, which is part of why it is being revisited for stubborn infections, though robust human data outside malaria is thin.
9. It Is The Established Antidote For Methemoglobinemia
This is the one setting where a higher dose is the correct dose, and it is worth understanding because it explains the whole safety picture.
In methemoglobinemia the iron in hemoglobin is stuck in a form that cannot carry oxygen, and MB at 1 to 2 mg/kg intravenously reduces it back to functional hemoglobin. R
The catch is that this rescue depends entirely on the enzyme Glucose-6-Phosphate Dehydrogenase (G6PD) supplying NADPH, which is why the same treatment is dangerous in people who lack it. R
That dependency is the bridge to the safety section, so read the dosage and genetics sections before touching this compound.
Sources And Forms
MB is not a nutrient and has no food source, so the only variable that matters is purity.
The single most important safety decision with methylene blue happens before you ever swallow it, and it is choosing the right grade.
- Aquarium grade is sold to treat fish and is not purified to remove the metal contaminants that commercial dye batches routinely carry. R
- Industrial or reagent grade is typically 85 to 95% pure and can carry zinc and other heavy-metal contaminants well above human limits. R
- Pharmaceutical USP grade must be at least 99% pure with heavy metals held to strict limits, and reputable suppliers publish a certificate of analysis for each batch.
Only the USP pharmaceutical grade is appropriate for human use, and analysis of commercial methylene blue samples has found metal contaminants making up as much as a quarter of the product by weight. R
For a product that meets this bar, look for pharmaceutical USP-grade methylene blue with a published certificate of analysis, sold as either a stabilized liquid or a pressed troche.
If a seller cannot show you a certificate of analysis, treat the product as aquarium dye regardless of what the label claims.
Dosage And Safety
The dose-response of MB is biphasic, which is the entire reason this section is long. R
Low doses are pro-mitochondrial and antioxidant.
High doses are pro-oxidant and inhibitory, and above a certain point MB will itself generate the reactive oxygen species it otherwise prevents. R

The Nootropic Range
Most cognitive and metabolic studies used roughly 0.5 to 4 mg/kg, with the memory benefit peaking near the low end and fading or reversing as the dose climbs. R
In practical terms that translates to oral microdoses in the single-digit to low-double-digit milligram range for most adults, not the concentrated dosing used in hospital antidote settings.
The honest position is that the optimal chronic human dose for cognition is not established, and more is decisively not better here.
Above roughly 10 mg/kg MB flips to a net pro-oxidant, and above about 7 mg/kg it can paradoxically induce the very methemoglobinemia it treats at antidote doses. R
Expect blue-green urine and possibly a blue tint to the tongue at any dose, which is harmless and simply confirms you took it.
The Three Contraindications That Actually Hurt People
Serotonin syndrome is the big one.
MB is a potent inhibitor of Monoamine Oxidase A (MAO-A), the enzyme that clears serotonin, so combining it with any serotonergic drug can drive serotonin to toxic levels. R
That means MB should not be combined with SSRIs, SNRIs, MAO inhibitors, tricyclics, triptans, or other serotonergic agents, because serotonin toxicity is one of the few drug interactions that can escalate to death within 24 hours. R
If you take an antidepressant, this compound is off the table unless a physician who understands the interaction has cleared it.

G6PD deficiency is the second.
People with Glucose-6-Phosphate Dehydrogenase (G6PD) deficiency cannot supply the NADPH that MB needs, and giving them MB can trigger Heinz-body hemolytic anemia instead of helping. R
Because G6PD deficiency is common and often undiagnosed, testing first is the conservative move. R
Product grade is the third, covered in the section above, and it is the one fully under your control.
MB is also not appropriate in pregnancy or in significant renal impairment, and it should be spaced well away from any serotonergic medication rather than simply reduced.
Mechanisms Of Action
Simple:
- Methylene blue is a rechargeable electron shuttle that picks up electrons where the mitochondrial assembly line is jammed and drops them off further down, keeping energy production running and cutting the free-radical spillover.
- At low doses that shuttle is protective, but at high doses the same molecule starts throwing off free radicals instead of preventing them, which is why the dose window is narrow.
Advanced:
- Alternative electron cycling at Complex IV. MB accepts electrons from NADH at Complex I, becoming leucomethylene blue, then reoxidizes by donating those electrons to cytochrome c and cytochrome c oxidase (Complex IV), bypassing Complex I and Complex III. R This maintains a partial proton gradient and sustains reduced-but-functional ATP synthesis while lowering superoxide leak, and flavin-dependent enzymes reduce MB while cytochrome c reoxidizes it, so the cycle is self-sustaining inside the mitochondrial matrix. R
- Hormetic redox reversal. The same redox activity that scavenges electrons at nanomolar-to-low-micromolar levels reverses at high micromolar levels, where MB begins auto-oxidizing and generating reactive oxygen species, producing the inverted-U dose-response seen in cytochrome oxidase activity and behavior. R
- NRF2-ARE induction. MB upregulates NRF2 and its target genes (HO-1, NQO1, glutathione-linked enzymes), engaging endogenous antioxidant defenses rather than acting purely as a stoichiometric scavenger. R
- MAO-A inhibition. MB is a potent reversible inhibitor of MAO-A, so it blocks the primary catabolic route for serotonin, which is the mechanistic basis for the serotonin toxicity seen when it is combined with serotonergic drugs. R
- G6PD and NADPH dependence. MB must be reduced to leucomethylene blue to do its antioxidant and methemoglobin-reducing work, and that reduction draws on NADPH generated by G6PD in the pentose phosphate pathway, which is why G6PD status determines whether MB helps or harms. R
Genetics
G6PD
G6PD encodes glucose-6-phosphate dehydrogenase, the rate-limiting enzyme of the pentose phosphate pathway and the only meaningful source of NADPH in red blood cells.
Loss-of-function variants leave erythrocytes unable to regenerate NADPH, so an oxidative challenge like MB causes hemoglobin to precipitate into Heinz bodies and the cell to lyse.
rs1050828 (the G6PD A- variant, common in people of African descent) and rs5030868 (the G6PD Mediterranean variant) are two of the most common deficiency alleles, and either one makes MB a hemolysis risk. R
Because the gene is X-linked, hemizygous males are affected more severely than heterozygous females. R
MAOA
MAOA encodes monoamine oxidase A, the enzyme MB inhibits.
Variants that lower baseline MAO-A activity leave less enzymatic reserve, which is plausibly relevant to how quickly MB pushes serotonin toward toxicity in someone also taking a serotonergic drug.
rs6323 is a functional coding variant that shifts MAO-A activity, and the MAOA-uVNTR promoter repeat also sets baseline expression level.
NQO1
NQO1 encodes NAD(P)H quinone dehydrogenase 1, a two-electron reductase in the NRF2 antioxidant program that MB helps induce.
rs1800566 (C609T, the P187S variant) markedly reduces NQO1 protein stability and activity, which lowers antioxidant reserve and is worth knowing for anyone leaning on redox-active compounds.
More Research
Alzheimer's and tau are the cautionary tale for anyone overselling this compound.
MB inhibits tau protein aggregation in the lab, which drove real excitement, but the phase 3 trial of the MB derivative LMTM (leucomethylthioninium) in mild-to-moderate Alzheimer's disease missed its primary endpoints. R
A monotherapy subgroup looked better in post-hoc analysis, which is hypothesis-generating and not proof, so the honest read is that MB's brain benefits remain small and unconfirmed at the clinical-outcome level.
Near-infrared light is the most practical stack, not oxygen or stimulants.
Because MB and NIR converge on cytochrome c oxidase, the cleanest pairing is a low MB dose with a red or near-infrared panel, and the dose-ceiling logic in the red light therapy dose ceiling post applies to both halves of that stack.
The NAD and NADPH picture matters more than the MB itself.
MB's whole function depends on redox cofactor availability, and its reduction to the active form is NADPH-limited, so people interested in this compound should understand the NAD and NADPH system first.
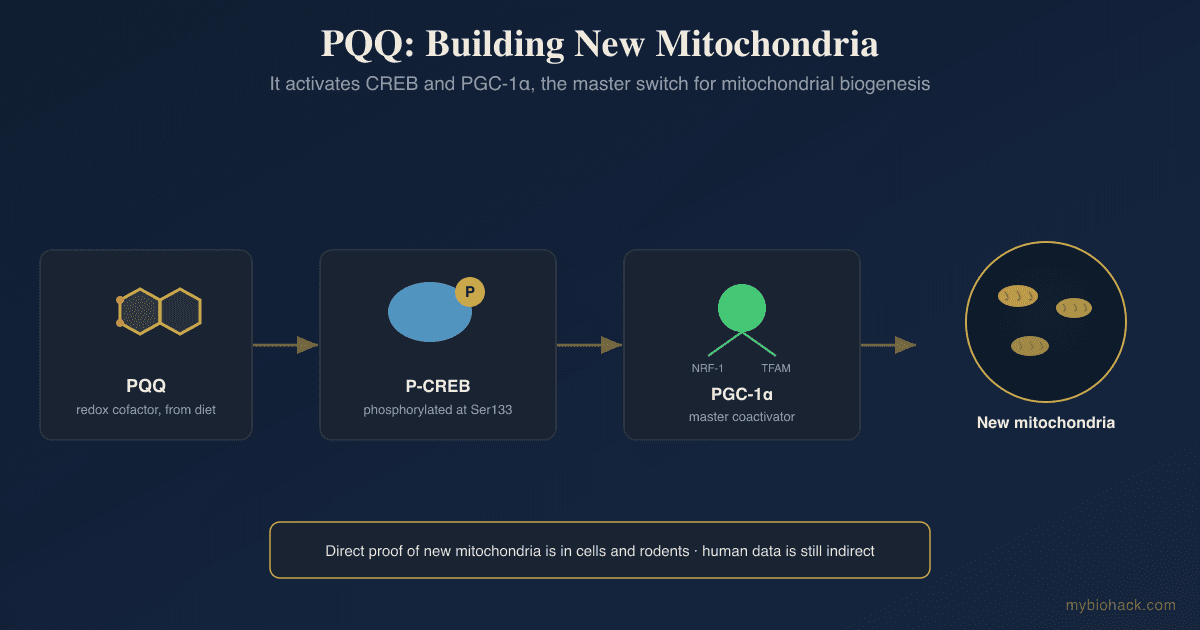
Related NAD-and-mitochondria levers worth reading alongside this are oxaloacetate, PQQ, and the humanin and mitochondrial-derived peptide work.
The post-viral angle is mechanistically interesting and clinically unproven.
In my Junction Dysfunction framework, a central hypothesis is that post-viral illness involves microcapillary perfusion loss and downstream tissue hypoxia, which stalls mitochondrial respiration and pushes cells toward free-radical output.
An alternative electron carrier that keeps Complex IV turning over under hypoxia is theoretically attractive in that setting, and I frame this as my hypothesis, not settled science.
There is no controlled trial of MB in long COVID or ME/CFS, the MAO-A and serotonin cautions are amplified in a population that is often already on serotonergic medication, and anyone exploring this should read the long COVID natural treatment protocol and work with a clinician rather than self-experimenting.
Timing and grade beat dose.
The two decisions that determine whether MB is safe are separating it from serotonergic drugs and buying a certified USP product, and both matter more than chasing an exact milligram.
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Lion's Mane
1000mg/day
Omega-3 (DHA)
2g/day
Phosphatidylserine
100mg 3x/day