7 Steps to Naturally Treat Long Covid (Science-Based Protocol)
By Jacob Gordon, INHC, FMT-CThis article contains affiliate links. As an Amazon Associate, MyBioHack earns from qualifying purchases at no extra cost to you. We only link products we research and stand behind.
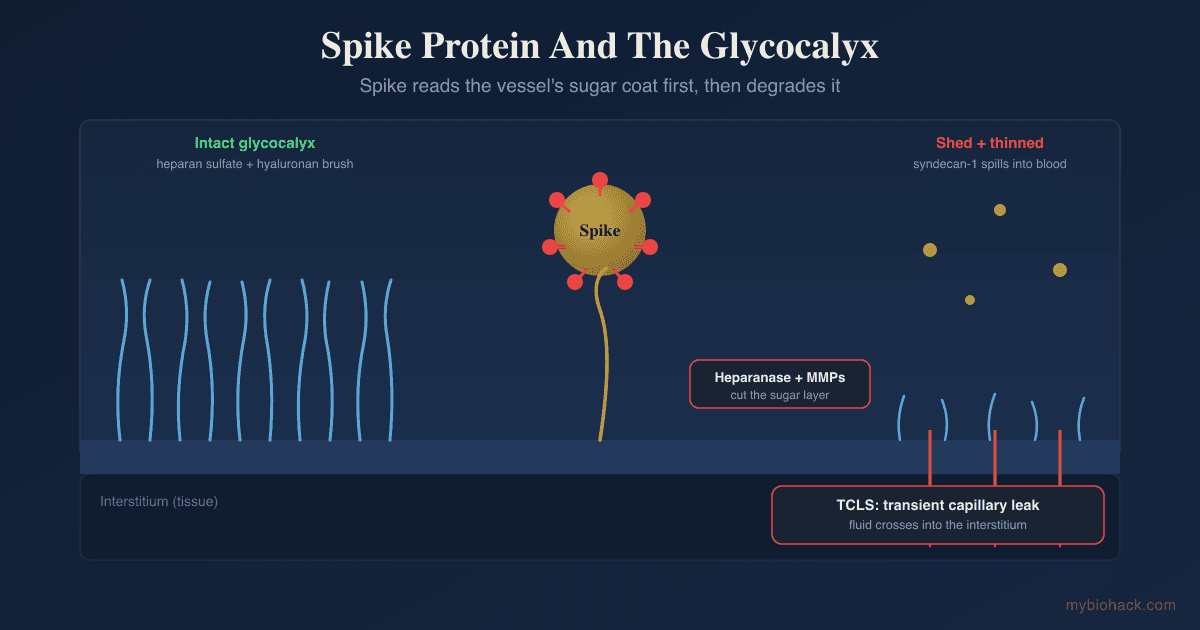
Long Covid is what happens when an acute viral infection ends but the damage it did to your blood vessels, immune system, and energy production never resolves.
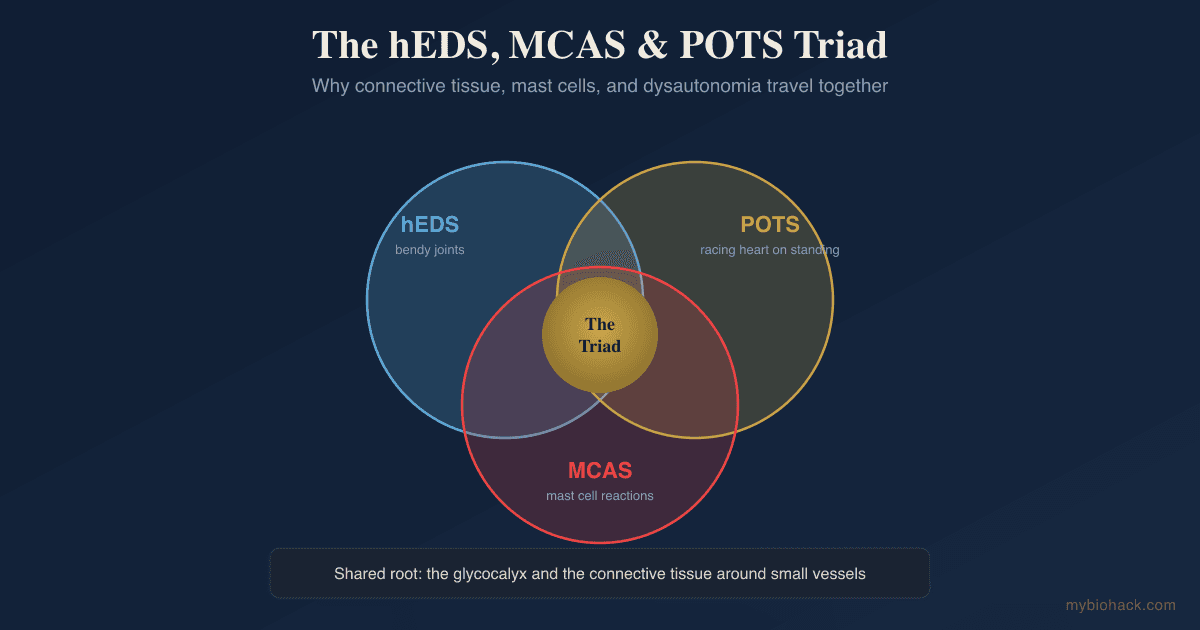
In this post, we will discuss what Long Covid actually is, why it persists at a mechanistic level through Junction Dysfunction, which conditions overlap with it, the step-by-step protocol I use to address it, what to avoid, and how to test for the underlying drivers.
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Electrolyte Complex
1 scoop/day
CoQ10
200mg/day
Magnesium Glycinate
400mg at bedtime