Spike Protein Persistence And The Glycocalyx
By Jacob Gordon, INHC, FMT-CSpike protein is the part of SARS-CoV-2 that first grabs the sugary coating of your blood vessels, and a growing body of evidence suggests fragments of it can linger in tissue and blood long after the infection clears.
In this post, we will discuss what the endothelial glycocalyx is, how spike protein binds it as a co-receptor step alongside ACE2, what glycocalyx shedding markers tell us about COVID severity, the honest debate over spike persistence, and how all of this maps onto my Junction Dysfunction framework for long COVID microvascular symptoms.

What The Endothelial Glycocalyx Is
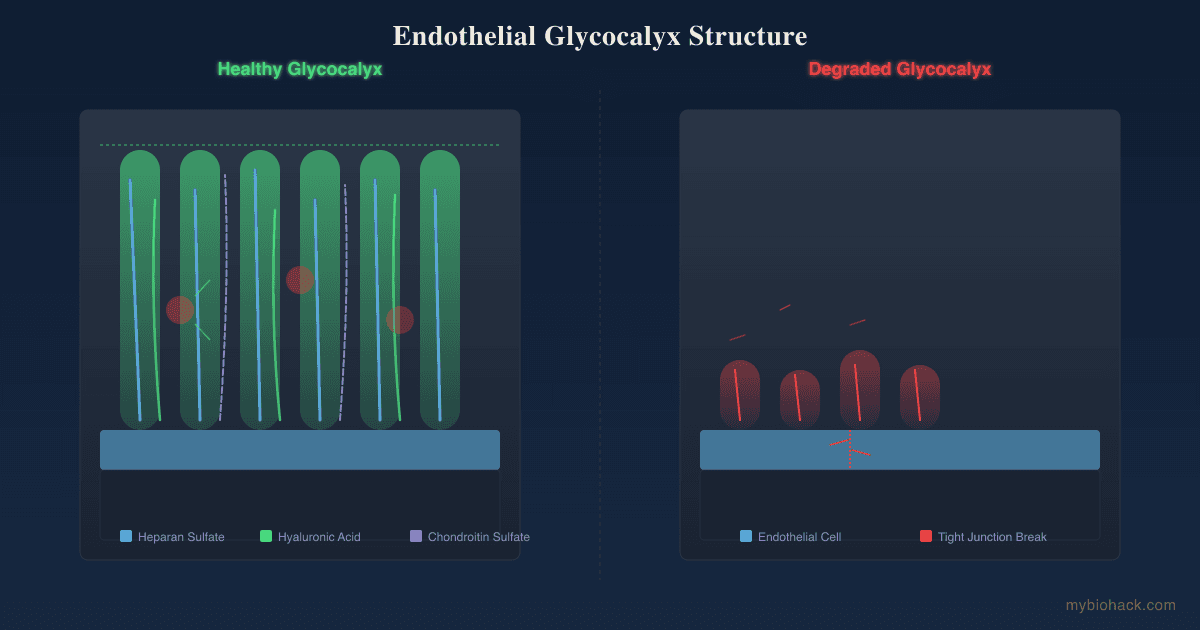
The endothelial glycocalyx is the negatively charged, highly sulfated sugar layer that coats the inner lumen of every blood vessel.
It is built from proteoglycans, glycosaminoglycans, and glycoproteins, with heparan sulfate (HS), hyaluronan (HA), and chondroitin sulfate as its dominant chains.
I cover the full structure, biomarkers, and imaging in the glycocalyx and the rebuild logic in Rebuilding Trees of the Forest, so this post stays focused on spike.
The glycocalyx is not decoration.
It senses shear stress to release nitric oxide, it holds antioxidant enzymes like extracellular superoxide dismutase on its surface, it regulates which immune cells can dock to the vessel wall, and it keeps fluid inside the vessel rather than leaking into tissue.
When it thins, all of those jobs degrade at once.
I call the umbrella pathology that follows glycocalyx compromise Junction Dysfunction (JD), and its two sub-pathologies are Transient Capillary Leak Syndrome (TCLS) and Micro-Sepsis (MSS), both terms I coined.
The glycocalyx is also the exact structure SARS-CoV-2 reaches first.
How Spike Protein Binds The Glycocalyx
Most coverage of SARS-CoV-2 entry jumps straight to angiotensin-converting enzyme 2 (ACE2).
The step before that is the glycocalyx, and this matters mechanistically.

The Heparan Sulfate Co-Receptor Step
Clausen and colleagues showed that SARS-CoV-2 infection depends on cellular heparan sulfate in addition to ACE2. R
Spike binds heparan sulfate through its receptor-binding domain at a site adjacent to the ACE2-binding site, and that binding shifts spike into an open conformation that makes ACE2 docking easier. R
In other words, heparan sulfate concentrates the virus at the cell surface and pre-positions it for ACE2, acting as a true co-receptor rather than a bystander. R
Heparin and other sulfated polysaccharides block this because they mimic heparan sulfate and act as decoys for spike. R
This is the molecular basis for why I pay so much attention to sulfated polysaccharides like fucoidans, which I cover in the guide.
The Sialic Acid Step
Spike also engages sialic acids, the negatively charged sugar caps on glycoproteins and gangliosides.
The N-terminal domain of spike binds terminal sialic acids and 9-O-acetylated sialic acid structures present in the airway. R
Sialic-acid-containing glycolipids mediate spike binding and viral entry with binding affinities in the same range as heparan sulfate. R
Single-molecule imaging shows that host sialic acid allosterically stimulates the receptor-binding domain, again favoring the open, ACE2-ready conformation. R
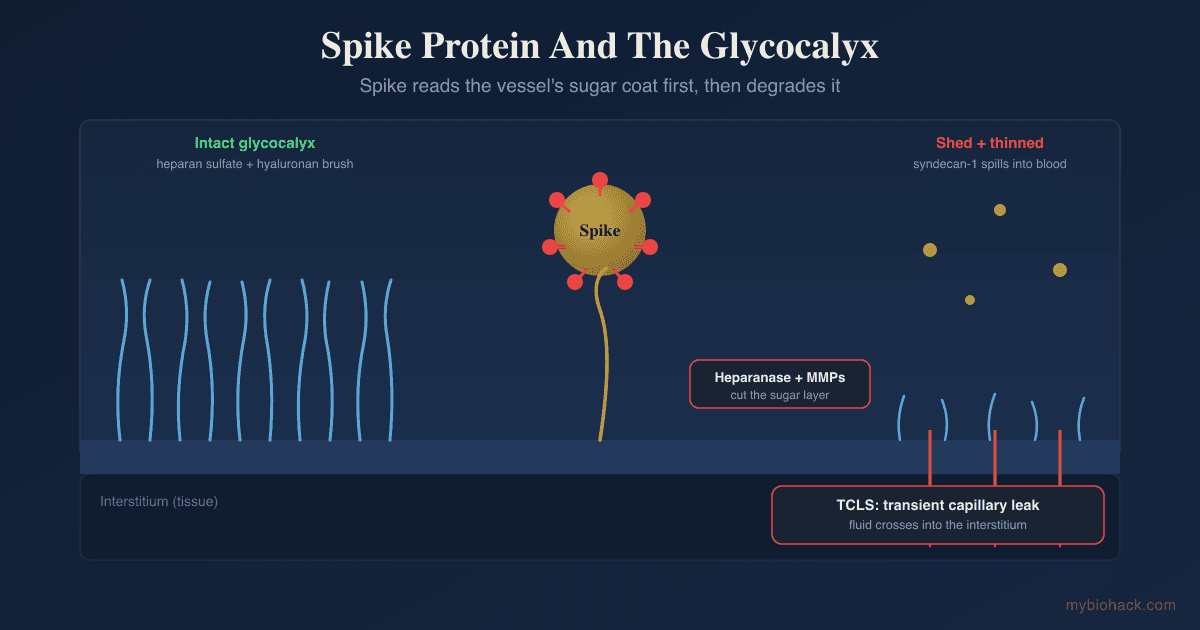
The takeaway is that spike is built to read the glycocalyx first.
It binds the same sulfated and sialylated sugars that make up the protective layer, and the act of binding both degrades that layer and primes the virus for entry.
Glycocalyx Shedding And COVID Severity
When the glycocalyx is cut, its fragments spill into the blood, where they can be measured.
The shed markers track disease severity closely.
- Heparan sulfate rises in plasma as the glycocalyx is degraded and correlates with severity. R
- Hyaluronan rises alongside heparan sulfate as hyaluronidase and metalloproteinases cleave the layer. R
- Syndecan-1 (the core proteoglycan that anchors heparan sulfate) is the most studied shedding marker, and admission levels rise in step with severity scores and predict mortality and longer hospital stays. R R
The enzymes doing the cutting matter as much as the markers.
Heparanase is a putative mediator of endothelial glycocalyx damage in COVID-19, cleaving heparan sulfate and amplifying inflammation. R
Interleukin-6 drives endothelial glycocalyx damage in both COVID-19 and bacterial sepsis, which is one reason the JD framework treats severe COVID and sepsis as mechanistic cousins. R
You can see the damage at the bedside, not just in a tube.
Sublingual imaging in critically ill COVID patients shows a thinner glycocalyx (a higher perfused boundary region) plus up to a 90% reduction in small-capillary density. R R
This capillary loss is the bridge to the long-term symptoms, because it does not always reverse.
Persistent capillary rarefication has been documented in long COVID patients well past the acute phase. R
The Spike Persistence Question
Here is where honesty matters more than narrative.
The claim that spike protein persists for months is partly supported and partly still contested, and it deserves to be presented that way.
What The Evidence Shows
Swank and colleagues detected circulating spike antigen predominantly in patients with post-acute sequelae of COVID-19 (PASC), in some cases up to 12 months after diagnosis, and rarely in those who recovered fully. R
A separate analysis of soluble and extracellular-vesicle-linked spike found persistent circulation in PASC at multiple time points. R
Patterson's group reported persistence of the S1 spike fragment inside CD16+ non-classical monocytes out to 15 months post-infection. R
A large Yale-led study of plasma antigen persistence found viral antigen, including spike, detectable in a subset of people in the post-acute phase. R
What Is Still Uncertain
Antigen detection does not prove a replicating viral reservoir, and assay sensitivity, cross-reactivity, and cohort selection all vary between studies.
Not every long COVID patient tests positive for circulating spike, so persistence is unlikely to be the whole story for everyone.
The honest position is that there is a big MAYBE here.
Spike or its fragments clearly persist in a meaningful subset of patients, the source (intact reservoir, antigen depot in tissue, or extracellular-vesicle cargo) is not settled, and the causal link to specific symptoms is associative rather than proven.
What is mechanistically coherent, regardless of source, is that any persistent spike has a standing supply of its preferred substrate (the glycocalyx) to keep degrading.
How This Connects To TCLS And Junction Dysfunction
This is my framework, so I will flag the speculative parts as my hypotheses, not settled science.
In the JD model, persistent or recurrent spike exposure is a chronic trigger that keeps the glycocalyx degradation cascade running.

The cascade I describe runs from inflammatory trigger, to immune-cell release of heparanase and matrix metalloproteinases, to glycocalyx degradation, to tight-junction opening, to TCLS.
TCLS is my term for the micro and transient form of capillary leak, where fluid transverses from the vessel lumen into tissue at the microvascular level.
When that leak happens at the capillary scale, classical blood-volume sensors do not register it, which is the heart of my hypothesis about vasoadaptive POTS.
My hypothesis is that TCLS explains the renin-aldosterone paradox seen in POTS, which I work through in full in microcapillaries and vascular POTS.
I also propose a bidirectional ANGPT/TIE2 and glycocalyx loop, where glycocalyx loss destabilizes Tie2 signaling under hypoxia, and Tie2 destabilization in turn accelerates glycocalyx shedding via heparanase release.
The supporting literature here is mixed and should be read honestly.
Angiopoietin-2 is clearly elevated in acute severe COVID and predicts ICU admission, which fits the loop. R
In long COVID specifically, some studies show angiopoietin-2 lower rather than higher than controls, so my loop is best treated as a hypothesis that holds most strongly in the acute and severe phase. R
The spike-RAGE arm reinforces the same endpoint.
Spike can bind and activate the receptor for advanced glycation end-products, driving NF-kB, reactive oxygen and nitrogen species, and further glycocalyx shedding, which is why I treat RAGE as a parallel road to the same TCLS endpoint.
I also separate this from the mainstream "asymptomatic long hauler" idea with my own framing.
My hypothesis (which I cannot currently prove) is that spike S1 alone, without viral replication, may be enough to break down the glycocalyx in people who were exposed without a symptomatic infection, a mechanism I work through in how SARS-CoV-2 targets people's weak spots.
I apply the same caution I apply to myself here, since I regret my own early Moderna booster, but this remains a mechanism I am proposing, not a proven cause.
For the full chapter-length treatment, the JD guide covers this in the TCLS chapter and the Micro-Sepsis chapter.
Spike Persistence And Overlapping Conditions
The glycocalyx-spike axis does not stay in one organ, which is why these conditions overlap.
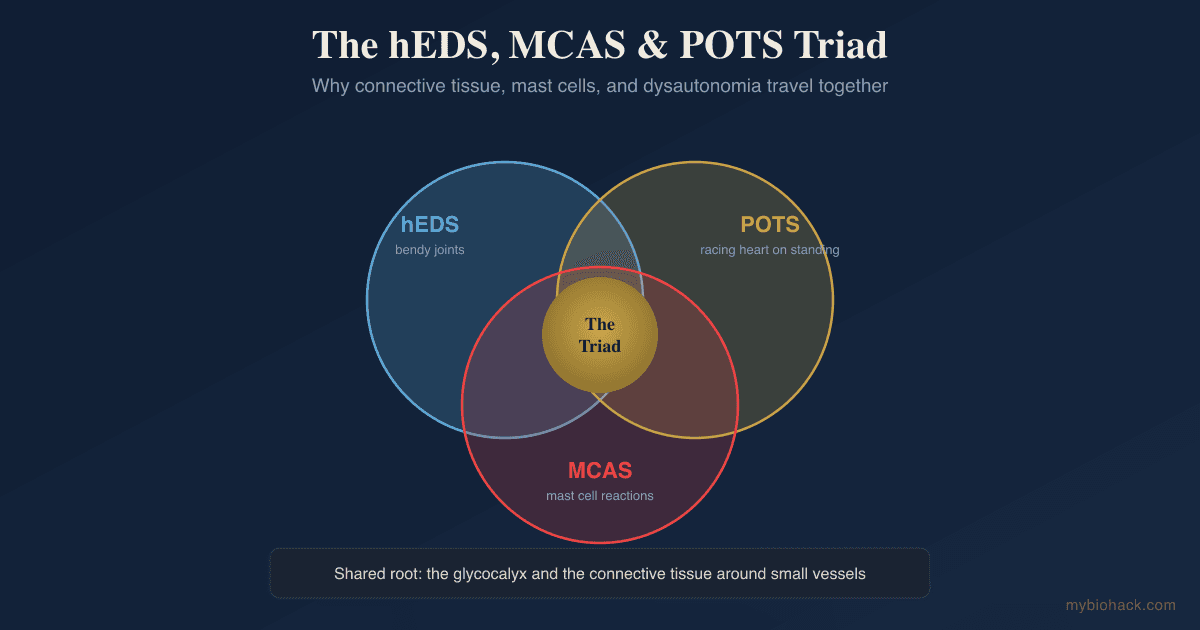
- Long COVID maps onto glycocalyx degradation, persistent capillary rarefication, and (in a subset) persistent spike, and I cover the full protocol in 7 steps to naturally treat long COVID. R
- ME/CFS overlaps heavily with long COVID and shows the same microvascular and microclot pathology, so I treat it as TCLS plus MSS plus circadian uncoupling. R
- Microclots (fibrinaloid, amyloid-resistant deposits) trap inflammatory cargo, resist normal fibrinolysis, and block capillaries, which I connect to my Adrenergic-Based Vaso-Adaptive Disorder (ABVAD) model in blood clots, platelets, and fibrin. R
- Vaso-Adaptive Disorder (VAD, my renaming of vascular POTS) follows from the loss of reserve microcapillaries described in microcapillaries and vascular POTS.
Two growth-factor responses tie these together, and I argue against reflexively suppressing either.
VEGF and TGF-beta1 both rise as part of the repair attempt, and I explain why lowering them blindly is a mistake in VEGF and TGF-beta1.
The leaked fluid has to go somewhere, which is the interstitium, the third circulatory system I cover in the interstitium.
For the upstream question of why spike hits some people harder, see how SARS-CoV-2 targets people's weak spots and how COVID causes aging.
How To Support The Glycocalyx
The logic is simple even when the biology is not.
Stop the cutting, supply the building blocks, and protect the charge.
Stop the cutting means blunting the heparanase, hyaluronidase, and matrix metalloproteinases that shed the layer.
Supply the building blocks means feeding it the sulfated sugars and glycosaminoglycans it is actually built from.
Protect the charge means defending the redox environment and the negative surface charge that let the layer sense flow and hold fluid inside the vessel.
That is the reasoning, and I give it away in full so you understand why the layer breaks and what direction repair has to take.
The protocol that follows from it is the part I keep inside the guide rather than this post.
The exact compounds, the high versus low molecular weight fucoidan logic, the decoy and repair sequencing, the dosing, the fasting and ketone repair window, and the loosely held spike and microclot tier are all sequenced and kept current in the Junction Dysfunction guide.
The glycocalyx rebuild chapters walk through the stack step by step in Rebuilding Trees of the Forest, and the fucoidan selection detail is in not all fucoidans are equal.
The Path membership unlocks the full guide and every glycocalyx chapter, and Pro adds the Health Hub so you can track your repair markers over time and run them past the Biohacking Bot.
Limbic and circadian work sit underneath all of it, because I do not see people get better with supplements and modalities alone, and the guide sequences that layer too.
Nothing in the guide is a treatment claim, and the protocol is built to be applied alongside a practitioner.
What To Stay Away From
A few common moves actively work against a damaged glycocalyx.
- High blood sugar, since hyperglycemia alters glycosaminoglycan sulfation and blocks hyaluronan binding to the layer.
- Overexercise and overtraining while symptomatic, since post-exertional crashes are mechanistic and high shear on a thin glycocalyx causes more shedding.
- Reflexive suppression of VEGF or TGF-beta1, which I argue against in VEGF and TGF-beta1.
- Blind L-arginine and nitric-oxide boosters, since uncoupled eNOS turns nitric oxide into peroxynitrite and L-arginine can reactivate latent viruses, a point I expand on in nitric oxide.
- Treating persistent symptoms as purely psychological, since capillary rarefication and microclots are measurable. R
Testing
Spike and glycocalyx damage leave measurable footprints, even if the cleanest research markers are not yet routine.
Endothelial And Glycocalyx Markers
The direct shedding markers (syndecan-1, heparan sulfate, hyaluronan) are mostly research-grade and hard to order clinically, but they are the cleanest readout when available. R
For the accessible proxies, I use the Cardiometabolic Panel (Vibrant Wellness) to assess endothelial function, ApoB, insulin resistance, and ceramides, since metabolic and endothelial stress travel together.
I use the Advanced Lipid Panel with Inflammation (Quest Diagnostics) when I want hsCRP and Lp-PLA2 alongside lipoprotein particle data.
Microclot And Coagulation Context
Microclots themselves require specialized fluorescence microscopy that few labs offer, but D-dimer and fibrinogen give an accessible coagulation snapshot, and I read them alongside the cardiometabolic markers above. R
Comprehensive Functional Panels
I use the Long COVID Bundle (Vibrant Wellness) to assess the cardio, toxin, gut, cellular, and viral domains together when the picture is post-viral.
I use the Cellular Health Panel (Vibrant Wellness) to assess oxidative stress and mitochondrial function, which downstream TCLS and MSS both degrade.
I use the Immune Panel (Vibrant Wellness) to read autoantibodies, which I frame as cleanup signatures of inflammatory debris rather than the immune system attacking healthy tissue.
I use the Viral Infections Panel (Vibrant Wellness) to assess reactivated latent viruses that ride along with immunosuppression.
For personalized interpretation of any of these, a consultation is the right venue.
Mechanisms Of Action
Simple:
- Spike protein grabs the sugary coating of your blood vessels first, and grabbing it both tears it and sets the virus up to enter the cell.
- When that coating thins, your vessels leak fluid, lose small capillaries, and stop signaling normally, which is most of what makes long COVID feel the way it does.
- Fixing it means blocking the things that cut the coating, feeding it the sugars it is made of, and keeping your blood sugar low enough to let it rebuild.
Advanced:
- Heparan sulfate co-receptor priming Spike engages heparan sulfate at a site adjacent to the ACE2-binding site on the receptor-binding domain, shifting the trimer to an open conformation and concentrating virus at the cell surface for ACE2 docking. R R
- Sialic acid allosteric stimulation The N-terminal domain binds terminal and 9-O-acetylated sialic acids and gangliosides, allosterically favoring the ACE2-ready conformation with affinities comparable to heparan sulfate. R R
- Enzymatic shedding cascade Inflammatory signaling, including interleukin-6, upregulates heparanase, hyaluronidase, and matrix metalloproteinases that cleave heparan sulfate, hyaluronan, and chondroitin sulfate, releasing syndecan-1 and exposing endothelial tight junctions. R R
- TCLS endpoint Tight-junction opening and microvascular leak produce intravascular hypovolemia, interstitial edema, immune-cell stasis, and capillary rarefication, which is the TCLS sub-pathology of Junction Dysfunction in my framework. R R
- Persistence as a standing trigger Circulating and cell-associated spike detected months after infection in a subset of PASC patients provides a chronic stimulus that, regardless of source, keeps the shedding cascade running on its preferred substrate. R R
Genetics
These are the variants from my Junction Dysfunction priority list that bear most directly on spike and the glycocalyx.
ACE2
ACE2 encodes the primary spike receptor and a regulator of the renin-angiotensin system.
Variants change ACE2 expression and spike binding affinity, which shifts both infection susceptibility and downstream angiotensin II signaling.
rs2285666 and rs4646116 (K26R) alter ACE2 expression and spike interaction.
AGER (RAGE)
AGER encodes the receptor for advanced glycation end-products, a parallel route spike can exploit to drive NF-kB and glycocalyx shedding.
Variants shift RAGE binding affinity and inflammatory set point.
rs2070600 (Gly82Ser), rs1800624, and rs1800625 change RAGE signaling and may raise the baseline shedding drive.
SUOX
SUOX encodes sulfite oxidase, which converts sulfite to sulfate.
Because the glycocalyx depends on heavily sulfated chains like heparan sulfate and chondroitin sulfate, impaired sulfate supply makes the layer harder to rebuild.
rs7297662 is associated with reduced sulfite-to-sulfate handling.
SOD2
SOD2 encodes mitochondrial superoxide dismutase, and extracellular SOD sits on the glycocalyx surface, so SOD loss and glycocalyx loss compound each other.
Variants reduce superoxide quenching capacity and raise oxidative shedding of the layer.
rs4880 (Ala16Val) is the variant I see most often in clients with redox imbalance, and I carry it myself.
More Research
- Angiopoietin-2 elevation is robust in acute severe COVID but inconsistent in long COVID, so the ANGPT/TIE2 and glycocalyx loop should be read as strongest in the acute and severe phase rather than as a universal long COVID marker. R R
- Antigen-persistence studies disagree on prevalence and source, so detecting circulating spike supports a reservoir or depot in a subset of patients without proving it drives every symptom. R R
- For biomarker tracking over time I use the Cardiometabolic Panel and the Long COVID Bundle so repair-window interventions can be measured rather than guessed.
- Nattokinase spike degradation is in-vitro only, and the clinical question of whether oral dosing reaches and degrades tissue or circulating spike is unresolved. R
- Sulodexide is the most promising glycocalyx-precursor drug with human long COVID data, and larger blinded trials are the obvious next step. R R
If you want the protocol that follows from all of this, it lives in the Junction Dysfunction guide, which Path and Pro members unlock in full.
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Electrolyte Complex
1 scoop/day
CoQ10
200mg/day
Magnesium Glycinate
400mg at bedtime