The Interstitium: The Body's Third Circulatory System
By Jacob Gordon, INHC, FMT-CThis article contains affiliate links. As an Amazon Associate, MyBioHack earns from qualifying purchases at no extra cost to you. We only link products we research and stand behind.
The interstitium is a body-wide, fluid-filled network of interconnected spaces woven through every tissue and organ in the human body, and it was only formally characterized as a distinct anatomical system in 2018 using live-tissue imaging, before which it had been routinely collapsed and discarded during standard histological processing.
In this post, we will discuss what the interstitium actually is, how its structure was hidden for so long, how it regulates fluid, pressure, sodium, and immune function, what happens when it breaks down, which chronic conditions involve interstitial dysfunction, what you can do to support it, and the emerging research implications for cancer, fibrosis, edema, and drug delivery.
What The Interstitium Is
The human body has two well-recognized circulatory systems: the cardiovascular system, which moves blood under pressure through a closed network of vessels, and the lymphatic system, which collects fluid from tissues and returns it to the bloodstream. The interstitium is the third.
It is not a vessel system. It is the space itself: a continuous, fluid-filled compartment that exists in and between essentially every tissue in the body, through which interstitial fluid flows from capillaries toward lymphatic capillaries. It is the environment in which every cell in the body actually lives. R
The interstitial compartment accounts for approximately 20% of total body weight by volume in a healthy adult. R
To put the volumes in perspective: About two-thirds of total body water is intracellular. The remaining third is extracellular. Of that extracellular fraction, roughly one-seventh sits inside blood and lymph vessels. The rest, the vast majority of extracellular fluid, is interstitial. R
The interstitium is not simply a passive space that fluid passes through. It is a mechanically active, biochemically responsive, immune-competent tissue that sets the physical and chemical conditions for every cell it contacts. R
The 2018 Discovery: Why It Was Hidden In Plain Sight
Despite being everywhere in the body, the organized macrostructure of the interstitium was not formally characterized until 2018.
In 2015, two gastroenterologists, Dr. David Carr-Locke and Dr. Petros Benias, were examining a patient's bile duct for cancer using probe-based confocal laser endomicroscopy (pCLE), a technology that provides real-time histological imaging of living tissue at a depth of 60 to 70 micrometers during endoscopy. They saw a reticular pattern of fluorescein-filled sinuses that had no known anatomical correlate. They could not identify it. R
They brought in Dr. Neil Theise, a pathologist at NYU, who discovered that the same structures that appeared as organized, fluid-filled spaces in living tissue appeared as collapsed cracks in conventionally prepared microscope slides.
The reason is processing: conventional histology fixes tissue, dehydrates it, and embeds it in paraffin. That process drains the interstitial fluid. When the fluid leaves, the collagen bundles that support the open spaces collapse inward. What was a fluid-filled honeycomb highway becomes a dense-appearing wall of collagen under the microscope. Pathologists had been taught for decades to ignore those cracks as tissue processing artifacts. They were not artifacts. They were the interstitium. R
By freezing biopsy tissue before fixation, the 2018 Scientific Reports paper preserved the anatomy and revealed a previously unappreciated, widespread macroscopic fluid-filled space within and between tissues, supported by thick collagen bundles and lined on one side by fibroblast-like cells bearing endothelial markers and vimentin. R
The study found these structures in the submucosa of the entire gastrointestinal tract, the dermis, the peri-bronchial and peri-arterial soft tissues, the fascia between muscles, the urinary bladder, and the lining of the digestive tract, lungs, and urinary systems. The structures appeared wherever tissues are subject to intermittent or rhythmic compression: where the body moves, squeezes, pulses, and breathes. R
The "organ" question:
The 2018 paper called the interstitium an organ. That framing generated significant debate, and the consensus since has been more precise: the interstitium is a system rather than a standalone organ, analogous to how the immune system or the lymphatic system is not a single organ but an integrated, body-wide network. R
Whether it is called an organ, a system, or a compartment does not change its biology. What changed is that we now have the imaging tools to see it in a living state.
Structure: Collagen, GAGs, And The ECM Scaffold
The non-fluid components of the interstitium are collectively called the extracellular matrix (ECM). The ECM is not inert scaffolding. It is an active mechanical and signaling environment. R
The structural proteins:
Collagen types I, III, and V form the primary load-bearing scaffold. Thick collagen bundles provide tensile strength and define the geometry of the fluid-filled spaces. These bundles are rigid enough to maintain open lumens but flexible enough to deform under compression and spring back. R
An important and underappreciated property of collagen: when stacked to sufficient density, it becomes piezoelectric, meaning it converts mechanical deformation into electrical current. Movement of the body, organ contractions, breathing, and heartbeat all generate piezoelectric signals within the collagen scaffolding. These electrical signals may drive the movement of charged molecules through the interstitium and contribute to intercellular communication across tissue layers independent of chemical signaling. R
Elastin provides recoil: the ability of compressed tissue to return to its resting volume.
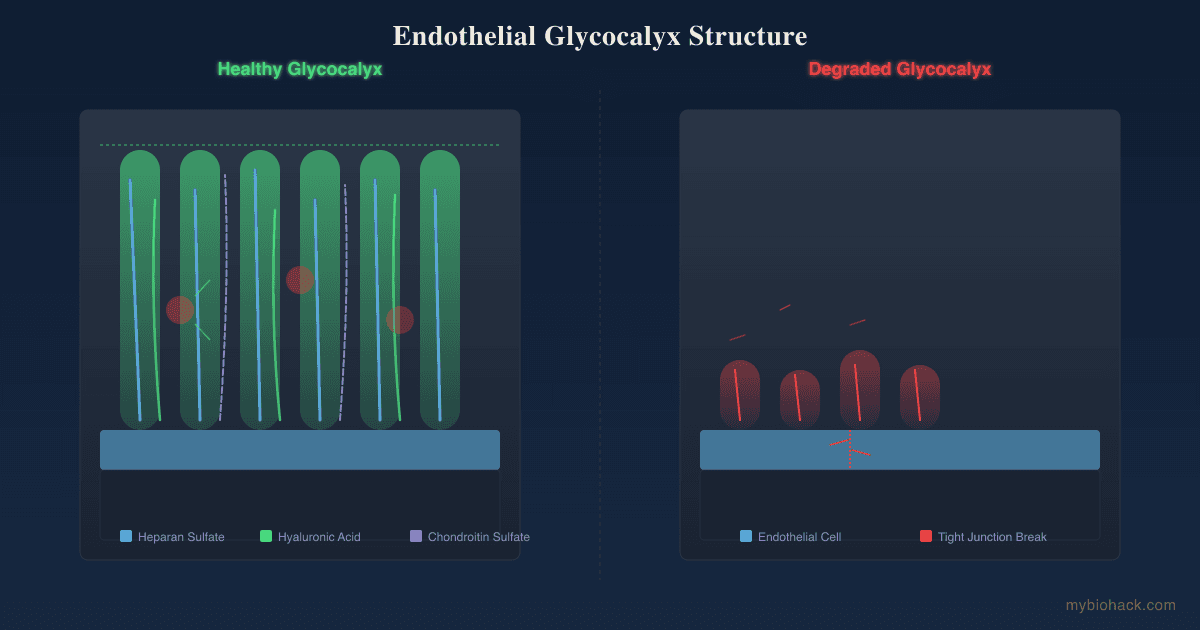
Glycosaminoglycans (GAGs) are the water-loving molecules of the matrix. GAGs include hyaluronan (non-sulfated) and the sulfated GAGs: heparan sulfate, chondroitin sulfate, dermatan sulfate, and keratan sulfate. The sulfated GAGs are covalently bound to protein cores to create proteoglycans, large macromolecules that carry a net negative charge and attract and bind cations, particularly sodium ions. R
Hyaluronan creates imbibition pressure: it acts like a sponge, drawing water into the interstitium and expanding interstitial volume while reducing interstitial fluid pressure.
The interstitial cells:
The spaces between the structural proteins are populated by several cell types:
- Fibroblasts: synthesize and maintain ECM components; actively compact the matrix by attaching to collagen fibers via integrin connections and pulling them inward, which acts as a counterbalancing force against GAG-mediated expansion R
- Dendritic cells: antigen-presenting cells that sample the interstitial fluid for foreign material
- Macrophages: tissue-resident immune effectors; also critical sensors of interstitial electrolyte concentration
- Mast cells: sentinel immune cells that trigger local inflammation when activated
- Interstitial cells of Cajal (in gut): pacemaker cells that coordinate smooth muscle contraction
Fibroblasts, through their integrin-mediated attachments to collagen, play a continuous mechanical role in maintaining normal interstitial pressure. When integrin signaling is blocked or disrupted experimentally, interstitial fluid pressure falls within minutes. This has direct implications for inflammation, where cytokines (IL-1alpha, PGE2) inhibit fibroblast compaction and reduce interstitial pressure as part of the inflammatory response. R
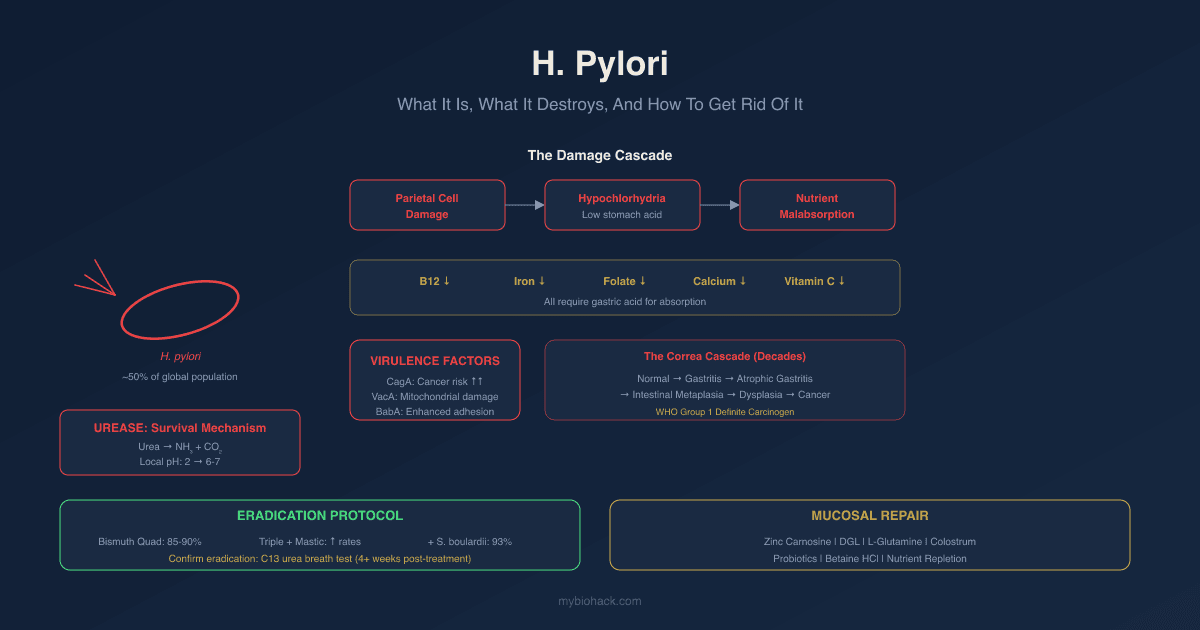
What The Interstitium Does
Nutrient and waste transport:
Capillaries deliver oxygen, nutrients, hormones, and signaling molecules into the interstitial fluid. Cells absorb what they need from the interstitial fluid surrounding them and export metabolic waste into it. That waste-laden fluid then flows through the interstitium toward lymphatic capillaries for removal.
This pathway is not just passive diffusion. Bulk convective flow of interstitial fluid drives the delivery of macromolecules (proteins, growth factors, cytokines) that are too large to diffuse efficiently through the dense ECM gel. Interstitial fluid flow is essential for protein transport to parenchymal and interstitial cells precisely because these macromolecules cannot readily diffuse through the ECM unassisted. R
Shock absorption:
The fluid-filled spaces of the interstitium act as mechanical shock absorbers, distributing compressive forces across tissues to prevent tearing during normal movement, breathing, heartbeat, and peristalsis. This is likely why interstitial macrostructures are most developed in tissues subject to intermittent or rhythmic compression: the submucosa, fascia, peri-arterial adventitia, and dermis. R
Lymph formation:
The interstitial fluid that enters blind-ended lymphatic capillaries in tissue becomes lymph. The interstitium is therefore the direct precursor and primary source of lymph. Lymph formation depends on interstitial fluid pressure being sufficient to open the overlapping endothelial flap valves at the lymphatic capillary wall. R
Immune trafficking:
The interstitium is the route through which antigens, immune cells, and cytokines move between tissue compartments. Dendritic cells loaded with antigen from the interstitium migrate via lymphatic capillaries to regional lymph nodes to initiate adaptive immune responses. Chemokines in the interstitial fluid create gradients that direct immune cell migration. Interstitial fluid flow itself orients interstitial chemokine gradients and influences which direction cells migrate. R
Blood pressure buffer and circulatory reserve:
When blood volume drops acutely (hemorrhage, dehydration), the body rapidly recruits interstitial fluid into the circulation to maintain blood pressure. This autotransfusion from the interstitium is possible because of the low compliance of the interstitium at normal-to-low volumes: a small reduction in interstitial pressure (from the drop in capillary filtration pressure) drives interstitial fluid back across the capillary wall into the blood. This is the mechanism that buys time after blood loss before full circulatory collapse. R
The Starling Forces: How Fluid Moves
Fluid movement across the capillary wall into and out of the interstitium is governed by Starling forces, four competing pressures across the capillary membrane:
Capillary hydrostatic pressure (Pc): the blood pressure pushing fluid out of the capillary into the interstitium.
Interstitial fluid pressure (Pi): the pressure in the interstitium that opposes inflow. Normal interstitial fluid pressure is slightly subatmospheric in many tissues (approximately -1 to -3 mmHg), creating a mild suction that draws fluid out of capillaries.
Plasma colloid osmotic pressure (COP): the osmotic pressure created by plasma proteins (primarily albumin) that draws fluid back into the capillary.
Interstitial colloid osmotic pressure: the osmotic pressure created by proteins in the interstitial fluid, which tends to draw fluid out of the capillary.
Net filtration = hydraulic conductivity x capillary surface area x [(Pc - Pi) - sigma(COP plasma - COP interstitium)]
In normal tissue, net filtration is slightly positive: a small amount of fluid continuously leaves the capillary, crosses the interstitium, and drains into lymphatic capillaries. This constant flow maintains protein homeostasis (preventing protein accumulation in the interstitium), delivers macromolecules to cells, and drives immune traffic. R
When Starling forces are disrupted:
Elevated capillary hydrostatic pressure (heart failure, venous obstruction): excessive filtration outpaces lymphatic drainage and edema forms.
Reduced plasma colloid osmotic pressure (low albumin states: malnutrition, liver failure, nephrotic syndrome): the oncotic draw into the capillary is lost and interstitial fluid accumulates.
Lymphatic obstruction (lymphedema, infection, post-surgical damage): fluid cannot drain and backs up in the interstitium.
Capillary leak (sepsis, burns, severe inflammation): capillary permeability increases dramatically, proteins flood the interstitium, raising interstitial colloid osmotic pressure and driving massive edema. R
The interstitial compliance buffer:
An important protective mechanism: at normal-to-low interstitial volumes, the interstitium has very low compliance (a small volume increase causes a large pressure increase). This low-compliance state keeps the system primed to defend against edema: when excess fluid enters, pressure rises quickly, which automatically reduces the pressure gradient driving filtration and partially self-limits edema formation. At higher volumes, compliance increases and fluid can accumulate more freely, which is the transition from compensated to decompensated edema. R
Interstitial Sodium Storage And Blood Pressure
One of the most clinically underappreciated functions of the interstitium is non-osmotic sodium storage.
The standard model of sodium and blood pressure places the kidney at the center: you eat salt, the kidney adjusts excretion, plasma volume changes, and blood pressure follows. This model is incomplete.
Human and animal studies have demonstrated that sodium can be stored in the interstitium, primarily in the skin and muscle, without a proportional increase in water retention. This sodium does not exist in free solution: it is bound to the negatively charged sulfated GAGs (primarily chondroitin sulfate and heparan sulfate) in the ECM. R
In rats fed a high-salt diet, skin sodium content increases without a corresponding increase in skin water, meaning the GAGs absorb the sodium non-osmotically, buffering plasma sodium concentration and blunting the blood pressure response to salt. Human subjects show a positive correlation between the GAG content of skin, arterial, and muscle tissue and tissue total sodium levels. R
When sodium storage capacity is exceeded or GAG structure is altered (a high-salt diet induces increased GAG sulfation and higher charge density in rats), the interstitium loses its sodium buffering function and blood pressure rises more steeply in response to dietary salt.
Macrophages and immune cells as interstitial electrolyte sensors:
Interstitial macrophages do not just surveil for pathogens. They function as local sensors of interstitial electrolyte concentration and, together with the lymphatic system, regulate sodium release and storage as a systemic mechanism of blood pressure control. This represents an extrarenal, immune-mediated blood pressure regulatory system that operates in parallel with the kidney. R
The clinical implications are significant: people who are "salt sensitive" (those whose blood pressure rises more with dietary salt intake) may have reduced interstitial sodium storage capacity due to GAG composition changes, structural ECM remodeling, or macrophage dysfunction. This is a kidney-independent pathway to hypertension.
The Interstitium And Immune Function
The interstitium is not just a transit corridor for immune cells. It is an active immune compartment.
Interstitial flow and immune cell orientation:
Interstitial fluid flow (the slow, pressure-driven bulk movement of fluid from capillaries toward lymphatics) creates chemokine concentration gradients in the interstitium that direct dendritic cell and T cell migration. The direction of flow creates a directional chemokine gradient that points toward the nearest lymphatic capillary. Immune cells follow these gradients toward lymph nodes. When flow is abnormal (as in lymphedema or tumors), these gradients are disrupted and immune trafficking fails. R
Interstitial macrophages:
Tissue-resident macrophages in the interstitium serve multiple roles: phagocytosis of pathogens and debris, antigen presentation, ECM remodeling, and electrolyte sensing. They exist in the interstitium of virtually every organ, including the myocardial interstitium of the heart, the renal interstitium of the kidney, and the pulmonary interstitium. In the skin, interstitial macrophages that sense elevated sodium concentration activate lymphangiogenesis via VEGF-C signaling, driving the growth of new lymphatic capillaries to drain the excess sodium-laden fluid. R
This macrophage-lymphatic axis is a mechanistic explanation for why dietary sodium affects both fluid balance and immune function.
Overlapping Conditions
Lymphedema
Lymphedema is the most direct consequence of interstitial dysfunction. When lymphatic drainage fails (from post-surgical damage, radiation, obesity-induced lymphatic dysfunction, filariasis, or congenital malformation), interstitial fluid and protein accumulate faster than they can drain.
The protein-rich interstitial fluid itself becomes the problem. Accumulated protein triggers chronic inflammation, mast cell and macrophage recruitment, fibroblast activation, and progressive fibrosis and adipogenesis in the interstitium. Proteoglycans accumulate faster than they are degraded, and the interstitial matrix stiffens and contracts, further impairing lymphatic function in a self-perpetuating cycle. R
Secondary lymphedema affects approximately 1 in 1,000 people globally and is the most common complication of cancer treatment (particularly post-mastectomy for breast cancer). R
Cancer Metastasis And Elevated Tumor Interstitial Fluid Pressure
The interstitium is implicated in cancer at two levels.
First, tumors that invade the interstitial space gain direct access to the lymphatic highway. The 2018 Benias et al. paper specifically noted that interstitial macrostructures provide a conduit for tumor cells to spread to lymph nodes, which is one of the primary routes of metastasis. R
Second, solid tumors develop pathologically elevated interstitial fluid pressure (tumor interstitial fluid pressure, or TIFP). Normal interstitial fluid pressure is slightly subatmospheric. TIFP in solid tumors is typically 5 to 40 mmHg above atmospheric pressure, created by a combination of: leaky tumor vasculature (plasma proteins flooding the interstitium and raising interstitial COP), absent or dysfunctional intratumoral lymphatics (fluid cannot drain), and ECM stiffening from cancer-associated fibroblasts. R
Elevated TIFP is an established negative prognostic factor in multiple tumor types (cervical cancer, melanoma, breast cancer) and directly impairs drug delivery. When TIFP at the tumor periphery equals or exceeds capillary pressure, the normal inward pressure gradient that drives drug uptake reverses. Drugs are swept away from the tumor rather than into it. This is often misattributed to cellular drug resistance when it is a physical transport barrier. R
Elevated TIFP is therefore a primary reason why many drugs that work in cell culture fail in solid tumors.
Fibrosis And Connective Tissue Diseases
Progressive fibrosis in conditions like scleroderma, pulmonary fibrosis, hepatic fibrosis, and chronic kidney disease represents uncontrolled ECM remodeling in the interstitium. In each case, activated fibroblasts (myofibroblasts) overproduce collagen, cross-link it excessively, and stiffen the interstitial compartment. This stiffening impairs fluid flow, increases interstitial fluid pressure, reduces oxygen diffusion, and produces progressive organ dysfunction.
The mechanical stiffness of the fibrotic interstitium is itself a disease driver: cells sense ECM stiffness through integrin-mediated mechanotransduction, and stiff ECM activates signaling cascades (YAP/TAZ, TGF-beta) that further drive fibroblast activation and collagen deposition in a self-amplifying loop. R
Sepsis And Hypovolemic Shock
During sepsis, massive interstitial edema develops from capillary leak. Plasma proteins flood the interstitium, driving a dramatic increase in interstitial colloid osmotic pressure and further pulling fluid out of the vascular compartment. The interstitium expands while the bloodstream contracts. This is the pathophysiology of distributive shock: the fluid has not been lost from the body, it has moved from the vascular to the interstitial compartment. R
Managing interstitial fluid dynamics is now a primary focus of sepsis resuscitation research, with trials showing that both under- and over-resuscitation with IV fluids worsen outcomes by either failing to refill the vascular compartment or driving further interstitial flooding. R
Chronic Inflammatory And Autoimmune Conditions
In rheumatoid arthritis, systemic lupus, and other autoimmune conditions, the inflamed interstitium is the theater in which immune cells accumulate, cytokines concentrate, and tissue damage propagates. Interstitial fluid pressure falls during acute inflammation (from cytokine-mediated inhibition of fibroblast compaction), which paradoxically increases fluid flow into tissue and can actually accelerate immune cell recruitment and antigen delivery to lymph nodes. In some contexts, the interstitium amplifies rather than containing inflammation by acting as a high-flow immune corridor. R
Edema-Related Conditions
Heart failure: elevated venous back-pressure raises capillary hydrostatic pressure and drives interstitial flooding, producing pulmonary edema, peripheral edema, and ascites.
Hypoalbuminemia (from liver failure, nephrotic syndrome, malnutrition, or chronic protein-losing enteropathy): reduced plasma COP removes the oncotic pull keeping fluid in the vessel, and interstitial edema forms even at normal capillary pressures.
POTS and dysautonomia: impaired upright vasoconstriction allows excessive hydrostatic pressure in lower extremity capillaries, driving interstitial fluid accumulation in the legs and reducing circulating blood volume.
How To Support The Interstitium
Interstitial health is not commonly targeted in clinical practice because it is not yet a familiar clinical target. The interventions below address the biochemical and mechanical conditions that maintain interstitial function.
1. Maintain Hyaluronan And Proteoglycan Integrity
Hyaluronan is the most abundant GAG in the interstitium and the primary structural molecule maintaining interstitial hydration and pressure homeostasis. Its degradation by hyaluronidase enzymes (which are released during inflammation, cancer, and bacterial infections) collapses interstitial organization.
Hyaluronic acid supplementation: while oral hyaluronan has limited direct bioavailability, clinical trials have demonstrated reductions in knee joint synovial fluid pressure and dermal water content improvements, suggesting that oral HA can influence extracellular matrix hydration via systemic mechanisms. R Typical dosing: 120 to 200 mg daily.
Vitamin C: essential cofactor for collagen synthesis (prolyl and lysyl hydroxylases require ascorbate). Without adequate vitamin C, newly synthesized collagen cannot be properly hydroxylated, and collagen fiber integrity in the interstitium degrades. Vitamin C also directly scavenges interstitial reactive oxygen species that degrade hyaluronan. Typical dosing: 500 to 2000 mg daily; liposomal form for better absorption.
Collagen peptides: clinical evidence shows that oral hydrolyzed collagen peptides reach the dermal interstitium and stimulate fibroblasts to produce more collagen and hyaluronan. One randomized controlled trial found significant improvement in skin elasticity (p < 0.05) and a trend toward reduced wrinkle depth after 12 weeks of oral collagen supplementation, consistent with ECM remodeling in the dermal interstitium. R Typical dosing: 5 to 15 g daily of hydrolyzed marine or bovine collagen.
2. Support Lymphatic Flow
Because the interstitium drains into the lymphatic system, lymphatic stasis is the most direct cause of interstitial dysfunction. Supporting lymphatic flow is the most evidence-based way to maintain interstitial health.
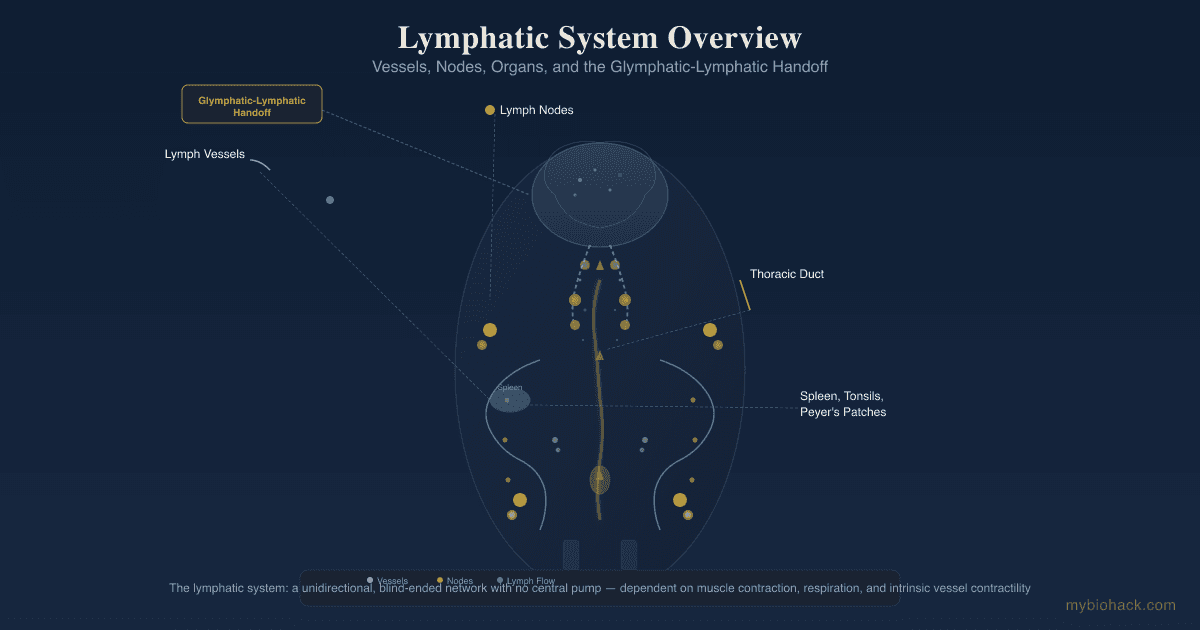
Movement: skeletal muscle contraction is the primary driver of lymphatic flow in the limbs. The lymphatic system has no central pump. It relies on muscle contraction, arterial pulsation adjacent to lymphatic vessels, respiratory pressure changes, and the intrinsic smooth muscle contractions of lymphatic collecting vessels. R Any sustained movement supports lymphatic drainage. Walking, swimming, and rebounding (mini-trampoline exercise) are particularly effective because they generate rhythmic compressive forces in tissues.
Diaphragmatic breathing: thoracic pressure changes during deep breathing create a pumping action that drives lymph through the thoracic duct, the main lymphatic trunk that returns lymph to the bloodstream. Deep, slow breathing with full diaphragmatic excursion is a practical tool for improving central lymphatic flow.
Manual lymphatic drainage (MLD): a specialized massage technique developed specifically to stimulate superficial lymphatic vessels and redirect stagnant interstitial fluid. It is the standard first-line treatment for lymphedema and is evidence-based for that condition. R
Compression garments: applied external pressure increases interstitial fluid pressure in the limb, opposing the hydrostatic gradient that drives fluid filtration from capillaries and promoting lymphatic vessel filling. Standard clinical recommendation for lymphedema and orthostatic edema.
3. Reduce Dietary Sodium To Interstitial Tolerance
Excessive dietary sodium, particularly in the context of reduced GAG storage capacity (which correlates with aging, ECM remodeling, and chronic inflammation), overwhelms interstitial sodium buffering and drives blood pressure elevation through a kidney-independent pathway. R
Targeting dietary sodium below 2.3 g per day (standard recommendation) and monitoring blood pressure response to sodium reduction is practical. Individuals with salt-sensitive hypertension may be expressing exhausted interstitial buffering capacity rather than primary renal dysfunction.
4. Address Hyaluronan Degradation Sources
Several common exposures accelerate hyaluronan and proteoglycan degradation in the interstitium:
Chronic infection: many bacteria (Streptococcus, Staphylococcus, Pseudomonas) produce hyaluronidase as a virulence factor to dissolve the interstitial ECM and spread through tissue. Persistent low-level infection can produce ongoing interstitial degradation. R
Smoking: cigarette smoke components including acrolein and reactive aldehydes directly degrade hyaluronan and collagen in the interstitium, contributing to the characteristic dermal aging and lung interstitial disease of chronic smokers.
Hyperglycemia: advanced glycation end products (AGEs) accumulate on collagen in the interstitial ECM in chronic hyperglycemia, crosslinking fibers abnormally and stiffening the interstitium in a pattern that resembles premature fibrosis. This is one mechanism through which diabetes accelerates tissue aging and organ fibrosis.
Berberine: has documented effects on reducing AGE formation and may modulate ECM composition through AMPK activation. R Typical dosing: 500 mg twice daily with meals.
5. Maintain Albumin And Colloid Osmotic Pressure
Hypoalbuminemia removes the primary oncotic force keeping fluid in capillaries. Clinical albumin below 3.5 g/dL (optimal range 4.0 to 5.0 g/dL) predicts interstitial edema and is associated with poor clinical outcomes across virtually every disease state.
Adequate protein intake (1.2 to 1.6 g per kg body weight daily) is necessary to maintain albumin synthesis. Liver function is required for albumin production, so hepatic support matters. In people with chronic illness, especially those with gut malabsorption, targeted amino acid supplementation may be required.
6. Proteolytic Enzymes For Interstitial Clearance
Serrapeptase and nattokinase are systemic proteolytic enzymes with evidence for breaking down fibrin and other interstitial protein accumulations, potentially improving fluid flow through fibrotic or congested interstitial compartments. The evidence base is modest (primarily observational) but the safety profile is reasonable in the absence of anticoagulant therapy. Typical dosing: serrapeptase 120,000 IU on an empty stomach; nattokinase 2000 to 4000 FU daily away from meals.
What To Stay Away From
- Prolonged sitting or standing without movement, which eliminates the skeletal muscle pump that drives lymphatic flow and allows gravity-dependent interstitial edema to develop, particularly in the lower extremities R
- Excess dietary sodium beyond the interstitial GAG buffering capacity, particularly relevant for individuals with age-related ECM remodeling, chronic inflammation, or obesity-related lymphatic dysfunction R
- Hyperglycemia and uncontrolled blood sugar, which drives AGE formation on interstitial collagen, abnormally crosslinks fibers, stiffens the ECM, and impairs interstitial fluid dynamics in a pattern resembling fibrosis R
- Smoking, which degrades hyaluronan, damages collagen, and promotes pulmonary interstitial disease
- Chronic NSAID overuse, which while acutely anti-inflammatory, chronically impairs prostaglandin-dependent regulation of interstitial pressure and can alter fibroblast compaction dynamics R
- Severely hypo-protein diets (including aggressive caloric restriction without adequate protein), which reduce albumin and colloid osmotic pressure, destabilizing Starling equilibrium and promoting interstitial edema and tissue wasting R
- TGF-beta promoting states (chronic inflammation, ongoing oxidative stress, high AGE load), as TGF-beta is the primary driver of myofibroblast activation and interstitial fibrosis R
Mechanisms Of Action
Simple:
- The interstitium is a body-wide fluid-filled compartment of interconnected spaces, accounting for approximately 20% of body weight by volume, that sits between capillaries and lymphatics and is the physical environment every cell inhabits R
- Fluid moves from capillaries into the interstitium down a pressure gradient and drains into lymphatic capillaries, continuously delivering nutrients and removing waste in a slow bulk flow driven by the four Starling forces R
- The ECM scaffold (collagen, elastin, hyaluronan, and proteoglycans) maintains interstitial architecture, controls fluid volume by balancing fibroblast compaction against GAG imbibition pressure, and buffers sodium non-osmotically through the negative charge of sulfated GAGs R
- Interstitial macrophages sense local electrolyte concentration and regulate lymphangiogenesis and sodium excretion, functioning as an extrarenal blood pressure regulatory system R
- Tumors elevate their interstitial fluid pressure above capillary pressure, reversing the drug delivery gradient and creating a physical barrier to cancer treatment that is frequently misidentified as cellular drug resistance R
Advanced:
The fibroblast-GAG mechanical equilibrium:
Interstitial fluid pressure at normal volumes reflects the tension between two opposing mechanical forces. Fibroblasts, anchored to collagen fibers via beta-1 integrin receptors, continuously exert inward tension that compacts the matrix and drives interstitial fluid pressure upward. Hyaluronan molecules in the gel phase exert outward imbibition pressure (osmotic swelling pressure), tending to expand the matrix and draw fluid in. The steady-state interstitial pressure is the equilibrium point of these two competing forces.
In inflammation, IL-1alpha and PGE2 inhibit fibroblast-mediated compaction without reducing GAG imbibition pressure. The balance tips toward expansion. Interstitial pressure falls, which increases the filtration gradient from capillaries into the interstitium, which expands interstitial volume and increases local immune cell and protein concentration. This is the mechanistic basis of inflammatory edema: it is not purely a consequence of increased capillary permeability, but an active, fibroblast-mediated interstitial remodeling response. R
GAG charge and sodium binding:
Sulfated GAGs carry one or more sulfate groups per disaccharide unit, giving them a net negative charge. These charges attract sodium cations electrostatically, binding sodium within the interstitial matrix without requiring commensurate water to maintain osmotic neutrality. This is non-osmotic sodium storage, distinct from the osmotic sodium in plasma and interstitial free fluid.
When dietary sodium load increases, the interstitium adapts by increasing the sulfation density and charge density of its GAGs, effectively upregulating its sodium buffer capacity. This adaptation requires macrophage-mediated signaling (specifically tonicity-responsive enhancer binding protein, TonEBP, in macrophages) and VEGF-C-driven lymphangiogenesis to increase lymphatic drainage capacity for the additional sodium load. The system is adaptive up to a point. When the adaptive capacity is exceeded (high chronic sodium load, age-related loss of GAG synthesis, chronic inflammation degrading GAG structure), interstitial sodium buffering fails and blood pressure rises via the traditional renal mechanism. This is why salt sensitivity increases with age and chronic disease. R R
Piezoelectric collagen signaling:
Collagen in the interstitium, when organized into bundles of sufficient density, exhibits piezoelectricity: the conversion of mechanical strain (compression, tension, shear) into electrical polarization and charge separation. Any deformation of the collagen scaffold, including body movement, organ contraction, breathing, and arterial pulsation, generates electrical signals within the ECM.
These piezoelectric currents may serve several functions: driving the electrophoretic transport of charged molecules (including ions and charged signaling proteins) through the interstitium along the electric field; providing a form of long-range mechanical-to-electrical signal transduction across tissue; and potentially influencing the behavior of electrically sensitive cells (fibroblasts, Cajal interstitial cells, neurons) embedded in the matrix.
The implication for bodywork, movement therapies, and acupuncture (which may act partly through piezoelectric mechanisms in dense connective tissue) is that physical compression and tension of interstitial tissue is not merely mechanical but generates electrical signals with potential systemic effects. This is a genuine area of emerging science rather than established clinical physiology, but the biophysical basis is mechanistically grounded. R
Tumor interstitial fluid pressure and drug delivery failure:
In normal tissue, interstitial fluid pressure (Pi) is slightly subatmospheric (-1 to -3 mmHg). In solid tumors, Pi rises to 5 to 40 mmHg above atmospheric. The driving forces are: leaky fenestrated tumor vasculature (plasma proteins extravasate freely, raising interstitial COP); absent intratumoral lymphatics (no drainage pathway); and stiff, cross-linked ECM produced by cancer-associated fibroblasts (which compacts the tumor matrix and raises mechanical pressure).
The consequence: net filtration across the tumor capillary wall is zero or reversed. The pressure gradient that normally drives fluid (and drugs) from capillaries into tissue is absent. Drug molecules that leave the blood vessel at the tumor periphery are swept back outward by the high-pressure interstitial efflux rather than convected into the tumor center. Only diffusion remains to deliver drugs past the tumor rim, and diffusion is ineffective over the distances of tumors more than a few millimeters in diameter. This is the physical basis of the "enhanced permeability and retention effect" working in reverse: what was supposed to trap drugs inside tumors instead creates an outward barrier. R R
Genetics
VEGFR3 (FLT4) and primary lymphedema:
The gene encoding vascular endothelial growth factor receptor 3 (VEGFR-3) is critical for lymphangiogenesis. Loss-of-function variants in VEGFR3 are the most common cause of Milroy disease, an autosomal dominant primary lymphedema characterized by bilateral lower limb edema from birth or infancy. VEGFR-3 is required for the development and maintenance of lymphatic capillaries, and without it, interstitial fluid cannot drain adequately and chronically accumulates. R
FOXC2 and lymphedema-distichiasis syndrome:
FOXC2 is a transcription factor required for normal lymphatic valve development. Loss-of-function FOXC2 variants cause lymphedema-distichiasis syndrome, in which lymphatic valves are absent or malformed, allowing retrograde lymph flow and progressive interstitial fluid accumulation. FOXC2 is also involved in maintaining the identity of lymphatic endothelial cells, and its loss leads to inappropriate blood endothelial gene expression in lymphatic vessels. R
COL1A1 and COL3A1 (collagen synthesis genes):
Variants in COL1A1 (collagen type I alpha 1) and COL3A1 (collagen type III alpha 1) are the basis of Osteogenesis Imperfecta and Ehlers-Danlos Syndrome (EDS) respectively, two conditions in which interstitial structural integrity is compromised from birth. In hypermobile EDS (hEDS) and classical EDS, the defective interstitial collagen scaffolding cannot maintain normal Starling equilibrium: joints hyperextend, capillaries leak under minimal pressure, and interstitial edema and connective tissue fragility are systemic. The POTS (postural orthostatic tachycardia syndrome) overlap in hEDS is likely partly explained by abnormal interstitial compliance in vascular adventitia, allowing excessive hydrostatic pressure-driven fluid shifts on standing.
AGT, ACE, and the renin-angiotensin-aldosterone axis:
The classical blood pressure genetics (variants in angiotensinogen AGT, angiotensin-converting enzyme ACE, and aldosterone synthase CYP11B2) are relevant to interstitial function because angiotensin II acts on fibroblasts in the interstitium to drive collagen production and ECM remodeling. Chronic activation of this axis in hypertension promotes interstitial fibrosis in the heart (cardiac fibrosis), kidney (tubulointerstitial fibrosis), and blood vessels, progressively stiffening these tissues. R
TGF-beta pathway genes:
TGF-beta1 (encoded by TGFB1) and its downstream signaling components (SMAD2, SMAD3, SMAD4) are the dominant drivers of interstitial fibrosis across virtually every organ. Variants that increase TGF-beta signaling are associated with systemic sclerosis, idiopathic pulmonary fibrosis, and other fibrotic conditions. Conversely, loss of negative regulators of TGF-beta signaling (SMAD7, which acts as an inhibitory SMAD) promotes uncontrolled fibrosis. Targeting TGF-beta-SMAD signaling is a primary strategy in anti-fibrotic drug development. R
More Research
- Interstitial fluid as a diagnostic biomarker. The 2018 Benias et al. paper explicitly proposed that direct sampling of interstitial fluid may become a powerful diagnostic tool. R Interstitial fluid bathes every cell and collects the secretome, metabolites, and damage signals of the surrounding tissue before they are diluted into the systemic circulation. Wearable sensors that continuously sample interstitial fluid for glucose (the standard CGM approach) represent the first clinical application of this concept, but interstitial proteomic and transcriptomic profiling for cancer biomarkers, infection markers, and drug metabolites is an active research area with significant clinical promise.
- Targeting tumor IFP to improve cancer drug delivery. Elevated TIFP is increasingly recognized as a primary cause of treatment failure in solid tumors that is independent of cellular drug resistance. R Several approaches are under investigation: anti-VEGF therapy (bevacizumab) normalizes tumor vasculature and can reduce TIFP; collagenase and hyaluronidase enzymes directly dissolve the dense ECM that maintains high TIFP; platelet-derived growth factor receptor (PDGFR) inhibitors reduce fibroblast compaction of the tumor matrix. PEGPH20, a pegylated hyaluronidase, showed early promise in pancreatic cancer but had mixed results in Phase III trials, illustrating that the clinical translation of IFP targeting remains incomplete.
- The interstitium and acupuncture. The anatomical mapping of traditional acupuncture meridian systems shows significant overlap with planes of dense connective tissue, fascial interfaces, and the interstitial spaces characterized by Benias et al. The piezoelectric properties of interstitial collagen provide a biophysical mechanism through which needling connective tissue could generate local electrical signals, and the interstitial fluid flow changes induced by needle placement could alter the chemokine gradients that direct local immune cell trafficking. This is a speculative but mechanistically grounded research direction that may eventually provide a structural anatomy for what has historically lacked one.
- For biomarker testing, continuous glucose monitors (CGM devices like Dexcom and Libre) are already sampling interstitial fluid in clinical use. They measure interstitial glucose rather than blood glucose with a lag of 5 to 15 minutes behind capillary measurements, reflecting the time for glucose to equilibrate between the capillary and the interstitial compartment. This lag itself is clinically informative: it reflects the kinetics of interstitial fluid dynamics and indirectly reflects interstitial health. Beyond glucose, lymphatic function can be assessed clinically via limb circumference measurement, bioelectrical impedance analysis (which distinguishes intracellular from extracellular fluid), and in specialized centers by lymphoscintigraphy or indocyanine green (ICG) lymphography.
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Electrolyte Complex
1 scoop/day
CoQ10
200mg/day
Magnesium Glycinate
400mg at bedtime