Root Causes Of Postural Orthostatic Tachycardia Syndrome (POTS) And Ways To Reverse It
By Jacob Gordon, INHC, FMT-CThis article contains affiliate links. As an Amazon Associate, MyBioHack earns from qualifying purchases at no extra cost to you. We only link products we research and stand behind.
In this post, we will discuss root causes of Postural Orthostatic Tachycardia Syndrome (POTS) and cutting-edge ways to reverse it and the symptoms.
Basics Of POTS
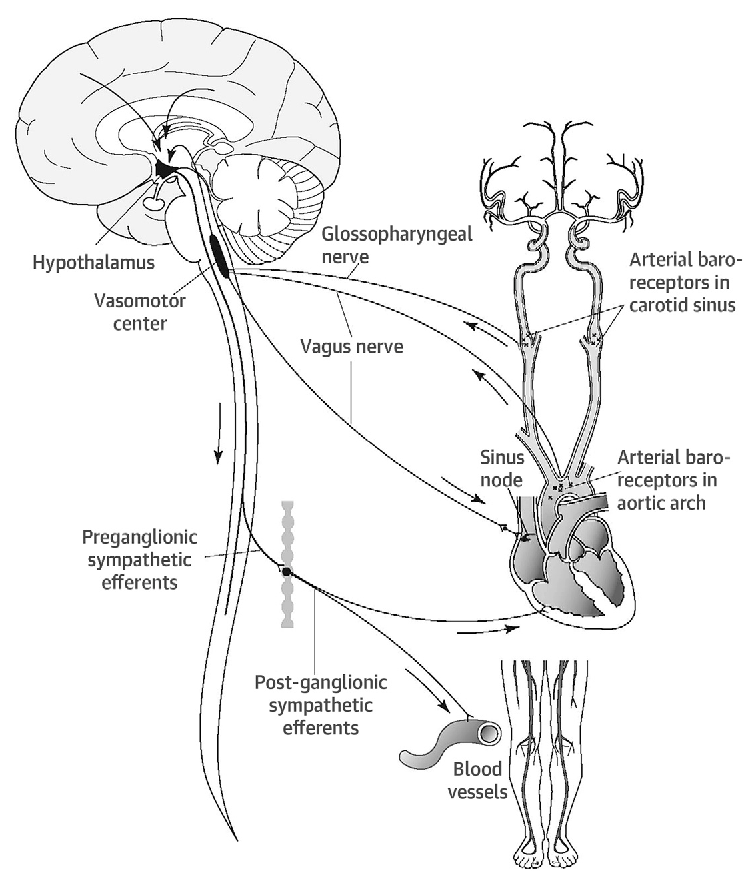
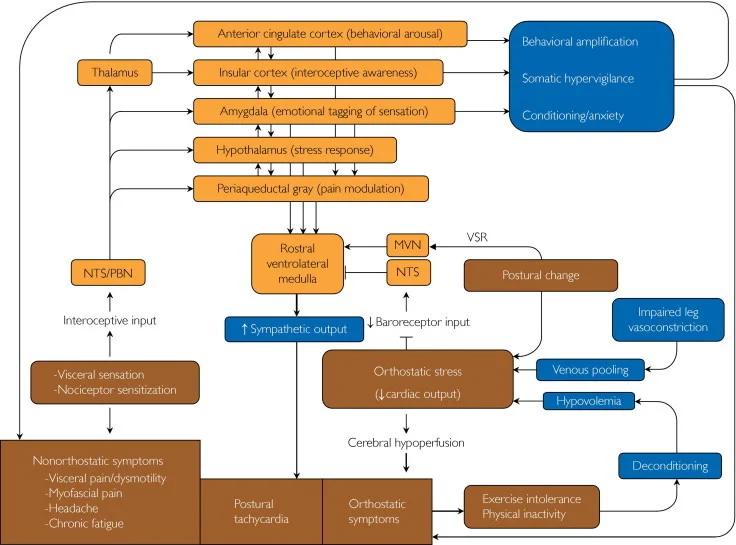
Postural orthostatic tachycardia syndrome (POTS) or chronic orthostatic intolerance (OI) is classified as an autonomic dysfunction of the nervous system from an abnormal vasovagal response.
This makes it difficult to keep an upright posture without abnormal heart-rate (tachycardia) and/or sympathetic activity. R
POTS is normally categorized into two categories:
Inflammation (usually from a toxin or infection) usually causes an autoimmune response inducing: R
Sympathetic activation (hyperadrenergic) - increased heart rate, but lower blood pressure (increased adrenergic vasoconstriction) R R
Parasympathetic withdrawal (neuropathic) - high adrenaline and noradrenaline (epinephrine and norepinephrine), which causes increased heart rate, but higher blood pressure (decreased adrenergic vasoconstriction) R R
If inflammatory dysautonmias aren't causing the symptoms of POTS, then it may be from spinal abnormalities, such as a CSF leak.
This autoimmune reaction depletes the body of molecules that quench oxidative stress.
Symptoms Of POTS
The hallmark sign of POTS is a measured increase in heart rate by at least 30 beats per minute within 10 minutes of assuming an upright position. R
Common symptoms of POTS are:
Abdominal Pain R
Anxiety R
Brain Fog R
Cognitive/Attention Deficits R
Depression R
Dizziness R
Exercise Intolerance R
Fatigue R
Headache R
Heart Palpitations R
Heat Sensitivity R
Impaired Consciousness R
Lightheadedness R
Nausea R
Sleep Disorders R
Sweating R
Tremors R
Tremulousness R
Weakness R
Symptoms are usually worse in the morning than at night (from intravascular volume loss overnight). R
Brain Fog, Oxidative Stress, And Temperature
POTS causes reduced blood flow to the brain, also known as cerebral blood flow (CBF). R
Many things can cause reduces CBF:
Low iron causes stress on red blood cells, causing an increases in eNOS, but decrease in hemoglobin. R
Reduced oxygenation of hemoglobin prevents cerebral oxygenation and vasodilation. R
POTS patients have decreased availability of nitric oxide (NO) from high ANG-II and low ACE2 levels, which leads to high levels of peroxynitrite (ONOO-). R R R R
Oxidative stress also increases adrenergic-mediated vasoconstriction (via excitotoxicity from ↑ NMDA activation). R R R
Increased ANG-II and decreased NO induces persistent hypoxia (low oxygen levels), as well as hypocapnia (low CO2 levels). R R
Hypoxia can cause reduce cerebral blood flow via downregulation of endocannabinoids. R
Low plasma renin activity and aldosterone levels, with high plasma ANG-II causes problems with sodium retention. R
Adrenomedullin (ADM) increases glomerular filtration in response to stress to protect the heart, but also increase NO. R
Endothelin (ET-1) is a vasoconstrictor that increases NE as well as ADM. R
Low levels of ET-1 can create a vasovagal reflex, while high levels (as seen in POTS) cause orthostatic hypotension. R
B-type natriuretic peptide (BNP) increases renal plasma flow, glomerular filtration rate, urine flow rate, and sodium excretion. R
Inflammation lowers BNP levels. R
Vasopression normally increases when standing. R
Galanin (GAL) can lower blood pressure and attenuate vagally-induced slowing of the heart rate. R
GAL usually increases when getting up from laying down, but in those with POTS GAL levels remain unchanged. R
All of this increases oxidative stress (specifically RNS, ROS), which induces brain fog. R
Blood pooling causes increased lactate, more ROS, and more brain fog. R R
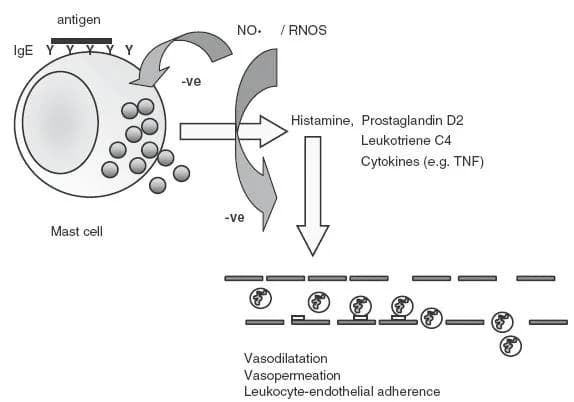
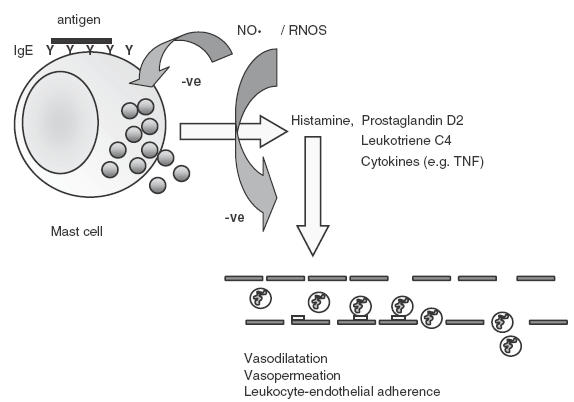
Mast cell degranulation also contributes to brain fog. R
NO also protects against mast cell degranulation and reduction of NO production has been seen in conditions such as histamine intolerance and mast cell activation syndrome (MCAS). R
NO can inhibit histamine and tryptase release and stabilize mast cells. R R R
Sjögren’s syndrome (SS) patients have less acetylcholine (ACh). R
NO increases ACh and transient receptor potential vanilloid type 1 (TRPV1), while neuronal NOS (nNOS) mediates ACh's of blood flow during extreme temperature changes and TRPV1 mediates CBF during extreme heat. R R R R R
Maintaining normal ACh (which may be low in POTS) helps keep keep orthostatic tolerance and CBF. R
All of this ultimately can lead to blunted responses to NO, reduced blood flow to the brain, and brain fog. R R
This is why some studies show that NO is high in POTS, especially since it induces vasodilation and inhibits adrenergic vasoconstriction, but with increased ONOO-, NO has less of a benefit. R R
Infections, Toxins, Choline, And Mitochondria
Infections and oxidative stress cause nitric oxide uncoupling (depletion of BH4). R R R
Infections and toxins turn NO into ONOO- when coupled with O2. R R
They also increase oxidative stress, that manifests in downregulation of nNOS. R
ONOO- can cause oxidation to the body, brain, and mitochondria while making NO less available. R
Mitochondria and cell thus can have less available choline (P-choline and CDP-choline via decreased CTL1/SLC44A1 activity), from constant oxidative stress. R
This oxidative stress also causes mitochondria to have reduced activity (lower respiration capacity, glycolytic activity, and ATP synthesis). R
Infections have shown high correlation to inducing POTS and other dysautonomias. R
The prevalence of these infections (if chronic) can cause autoimmunity (as with high resistin levels in POTS). R R R
Resistin can induce constriction (via increase of ET-1, VCAM1, and ROS) and reduce eNOS. R
CSF Leak, Cervical Instability, Hyper-Mobility, And Previous Trauma
CSF Leak
When there is a Dural Tear, Cerebrospinal Fluid (CSF) can leak out causing autonomic problems, especially hypotension from upright postures.
This can be caused from:
Calcification pushing on the dura
Hypermobility (overproduction of collagen)
Idiopathic nature
Injury (such as trauma to the spine)
This may require a blood patch - see post on natural and procedural Dural Healing techniques here.
I also recommend watching this video below.
Cervical Instability
Instability in the cervical neck can decrease the electrical firing and signaling of the vagus nerve, thus causing dysautonomic symptoms.
Testing for this would require a Digital Media X-Ray (DMX).
Dr. Ross Hauser does a great job at explaining it in the video below and resolves his patients with cervical prolotherapy.
Biomarkers
I usually look at a Total Toxicology Test for my POTS clients, as those are the most common issues to cause the dysautonomic biomarkers below.
Elevated:
Activin B R
α1-AR Ab R
ANA R
ANG-II R
beta1-AR Ab R
beta2-AR Ab R
Copeptin R
CRP R
IL-6 (can synergize with IL-1β and TGF-beta towards Th17 skewing Tregs) R R
IL-17A R
N-methylhistamine (high in MCAS) R
NE (can be low in neuropathic POTS) R
NO (increased in SS, but with higher antibodies) R
NPY R
Resistin R
Low:
Betaine R
Choline R
Iron R
Folate (not significant)
Vitamin B1 (low in adults)R
Vitamin B12 (low levels causes high adrenaline, also tends to be more common in adolescents) R R
Vitamin D (25-OH is common with low iron, while 1,25-OH is not common) R
Protocol To Improve POTS
Top Recommendations:
Astragalus (↓ ANG-II, ↑ eNOS, ↑ ACh) R R R
CDP-Choline (↑ mitochondrial CTL1/SLC44A1, ↑ ACh) R
Low Lectin diet (to reduce symptoms of autoimmunity) - eat frequent, smaller meals (less high insulin spikes) and keep physically active/not sitting laying down all day, helps reduce symptoms
Vitamin B1 (↑ ACh) R R
As POTS is multifactorial, this is not a one-size fits all – this order below is not definitive, but each section may be a contributing problem and must be addressed properly.
1. Deal With Underlying Infection, Toxin, Or Trauma
Infections can get into nervous tissue and cause dysautonomia, so they should be addressed first (posts pending): R
Candida
EBV/Mono
Herpes
Lyme
Mold
If you have a buildup of heavy metals they need to be removed as they can cause secondary POTS:
NRF2 activation also helps with some heavy metals as well as other oxidative factors contributing to secondary POTS.
If you have had trauma to the Dura Mater, then addressing that is very important to rule out CSF leak.
2. Increase Nitric Oxide
Typically you can get nitric oxide from eating leafy greens, but if you have dysbiosis in your mouth, this reaction of nitrates to nitrites will be blunted and you should supplement with nitrates until the oral dysbiosis is fixed. R
Also, depletion of BH4 will blunt the beneficial effects of NO, especially from an infection in the basal ganglia. R
Strong ways to increase nitric oxide (you want to increase nNOS, not iNOS): R
See all ways to increase nitric oxide here.
3. Other
Lifestyle/Therapies:
Avoid excessive heat, such as hot showers, sauna (sun may be an exception) R
Cognitive behavioral therapy R
CT-Guided, Percutaneous T2 Ethanol Ablation R
IV Saline R
Limit caffeine (↑ vasoconstriction, ↑ urination) unless you have CSF leak; alcohol; excessive carbs R R
Liquid and electrolyte (salt) intake R
Wear Compression stockings R
Supplements:
Drugs/Hormones:
Antibiotics (if you have SIBO) R
Beta-blockers R
Desmopressin (DDAVP) R
Droxidopa R
Erythropoietin R
Fludrocortisone R
Ivabradine R
Methyldopa
Methylphenidate R
Midodrine (for neuropathic POTS) R
Modafinil R
Naltrexone (as Low-Dose Naltrexone) R
Norepinephrine reuptake inhibitors R
Octreotide R
Physostigmine (strong for ACh inducing orthostatic tolerance) R
Propranolol R
Pyridostigmine R
Serotonin reuptake inhibitors R
Sertraline R
Vasopressin R
Pathways:
Increase α1-adrenergic receptor (for neuropathic POTS) R
Increase acetylcholine (acetylcholinesterase inhibition leads to an increase in CBF without a change in metabolism while supine) R
Increase GAL (via NPY) R
Increase RAAS (activating sodium retention to restore extracellular fluid volume) R
Inhibit HDAC (shown to increase SLC6A2 via MeCP2) R
Mechanism Of Action
Simple:
Nitric oxide becomes uncouple and depletes BH4 which causes high inflammatory nitric oxide, aka peroxynitrate (ONOO-), and thus nitric oxide is high, but less bioavailable.
Also, see biomarkers above.
Advanced:
Impaired vascular innervation, high plasma norepinephrine concentrations, mutation/reduced activity in the NE transporter (NET) SLC6A2 (A457P), α‐receptor sensitivity, β‐receptor hypersensitivity and baroreceptor dysfunction. R R
A blunted ACE 2 pathway which results in increased serum levels of ANGII, decreased Ang-(l-7), and resultant scant nitrous oxide (NO). R
The deficit in NO (as well as down-regulation of NO receptor sites) has been associated with increased plasma levels of ANG II, attributed to a defect in angiotension-converting enzyme-2. R
This is known to produce ROS via binding to ANG II type 1 receptors (AT1R) on NADPH oxidase and scavenging NO by superoxide. R
Cutaenously, eNOS is normal or high, while nNOS is low. R
Various autoantibodies, including those directed against cardiac proteins, β1/2-adrenergic, M2/3 muscarinic and N-type acetylcholine receptors, have been identified in POTS patients, strengthening the idea of POTS as member of the autoimmune autonomic neuropathies family. R
In choline synthesis R
↑ remethylate homocysteine (tHcy) + ↑ cystathione (tHcy metabolite) + ↓ cysteine (metabolite of cystathione)
The choline transporter is ↓ CTL1/SLC44A1 (~2.5x) in skin -> causing less cellular uptake (60%) and mitochonrdial (50%) uptake of choline
↓ P-choline and ↓ CDP-choline
↓ respiration capacity, ↓ glycolytic activity, and ↓ ATP synthesis
Primary actions of neuropeptides/peptide hormones: R
Vasodilation
B-type natriuretic peptide
Atrial natriuretic peptide
Adrenomedullin
Galanin
Vasoactive intestinal peptide
Vasoconstriction
Endothelin (1-3)
Vasopressin
RAAS inhibition
Endothelin (1-3)
Galanin
Diuresis
B-type natriuretic peptide (BNP)
Atrial natriuretic peptide (ANP)
Galanin
Vasoactive intestinal peptide (VIP)
Genetics
ENOS
rs2070744 (T-786C)
With E298D - experienced the largest changes in heart rate and plasma norepinephrine with standing R
C allele of the T-786C polymorphism reduces eNOS activity as a result of suppressed NOS3 transcription R
E298D
With Or without T-786C - experienced the largest changes in heart rate and plasma norepinephrine with standing R
TT allele - increased myocardial infarction (MI) in smokers vs GG R
SLC6A2
rs5564 (I'm AA)
significantly associated with the diagnosis of POTS R
rs7194256
T allele - found higher in POTS, panic disorder, major depression and hypertension R
More Research
Astronauts returning from space not yet re-adapted to gravity may demonstrate symptoms of POTS. R
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Electrolyte Complex
1 scoop/day
CoQ10
200mg/day
Magnesium Glycinate
400mg at bedtime