The Cholinergic Anti-Inflammatory Pathway: The Vagus Nerve Brake On Inflammation
By Jacob Gordon, INHC, FMT-CThis article contains affiliate links. As an Amazon Associate, MyBioHack earns from qualifying purchases at no extra cost to you. We only link products we research and stand behind.
Most chronic-illness protocols spend all of their effort lowering inflammation and almost none restoring the nerve that is supposed to switch it off.
In this post, we will discuss the cholinergic anti-inflammatory pathway, the vagus-to-spleen circuit that runs it, the alpha-7 nicotinic receptor that does the actual braking, why low vagal tone keeps you systemically inflamed, and how to rebuild the signal.

Basics Of The Cholinergic Anti-Inflammatory Pathway
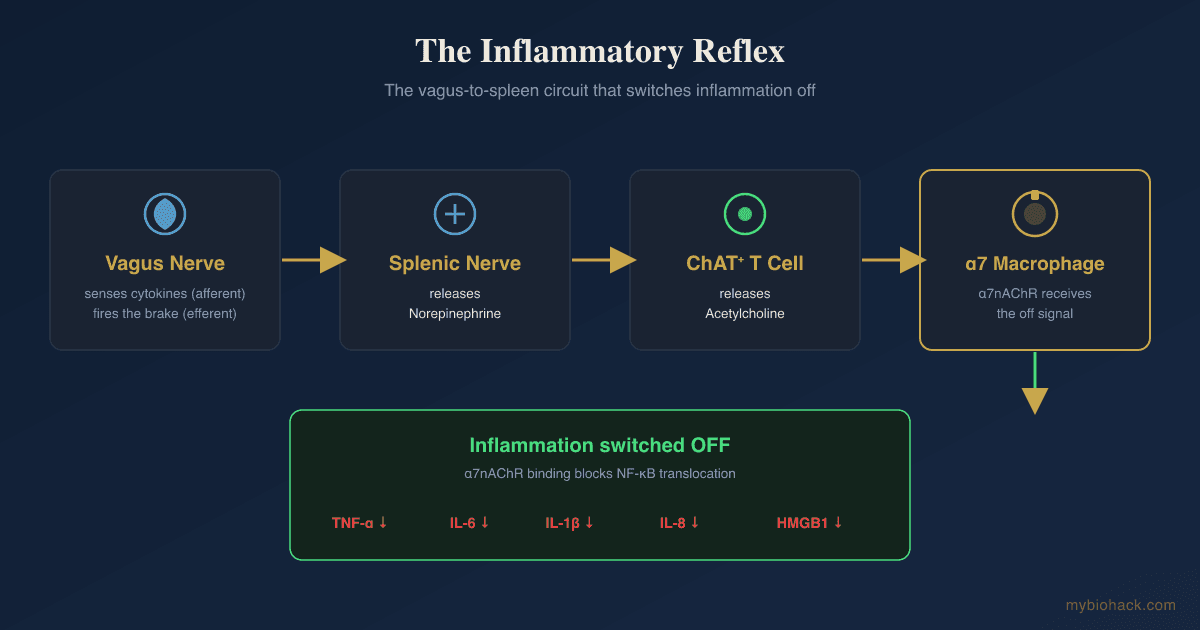
The Cholinergic Anti-Inflammatory Pathway (CAP) is a hardwired reflex in which the vagus nerve detects inflammation and then actively shuts it down. R
It is the efferent (motor) arm of what Kevin Tracey named the inflammatory reflex. R
The afferent (sensory) arm of the vagus senses circulating cytokines and pathogen fragments, and the efferent arm sends a signal back out that suppresses the production of inflammatory cytokines. R
The signaling molecule at the business end of this pathway is Acetylcholine (ACh), the primary parasympathetic neurotransmitter. R
The original experiment was simple and striking.
Electrical stimulation of the vagus nerve in animals given a lethal dose of endotoxin sharply reduced Tumor Necrosis Factor Alpha (TNF-α) and protected against shock. R
Cutting the vagus did the opposite and made the inflammatory response worse. R
This is the brake that most chronic-illness protocols never touch.
You can chase down TNF-α, IL-6, and Nuclear Factor Kappa B (NF-κB) with supplement after supplement, but if the nerve that is supposed to govern them is offline, you are bailing water without fixing the leak.
The Vagus-To-Spleen Circuit
The vagus nerve does not release acetylcholine directly onto the immune cells that matter most.
The circuit runs through the spleen, which is where a large share of the body's inflammatory cytokine production happens during a systemic challenge. R
The relay works in a specific sequence.
Vagal signals synapse onto the splenic nerve, which releases norepinephrine inside the spleen. R
That norepinephrine then acts on a specialized population of T cells that express Choline Acetyltransferase (ChAT), the enzyme that synthesizes acetylcholine. R
These ChAT-positive T cells release the acetylcholine that the rest of the circuit depends on. R
In other words, a subset of your immune cells has been recruited to act as the final neurotransmitter source for a nerve reflex. R
The acetylcholine they release diffuses onto nearby cytokine-producing macrophages, and that is where the inflammation actually gets switched off. R
The Alpha-7 Nicotinic Brake On Macrophages
The receptor that receives the off signal is the Alpha-7 Nicotinic Acetylcholine Receptor (α7nAChR), expressed on macrophages and other innate immune cells. R
This single receptor is the molecular core of the entire pathway.
When acetylcholine binds α7nAChR on a macrophage, the cell stops translocating NF-κB into the nucleus, which collapses the transcription of the major inflammatory cytokines. R
The result is reduced TNF-α, IL-1β, IL-6, IL-8, and HMGB1 output from that macrophage. R
The proof that α7nAChR is non-negotiable comes from knockout work.
Vagus nerve stimulation suppresses TNF in normal mice but completely fails to do so in mice that lack the α7 subunit. R
No α7nAChR means no brake, no matter how much acetylcholine is present. R
There is a second function here that is easy to miss.
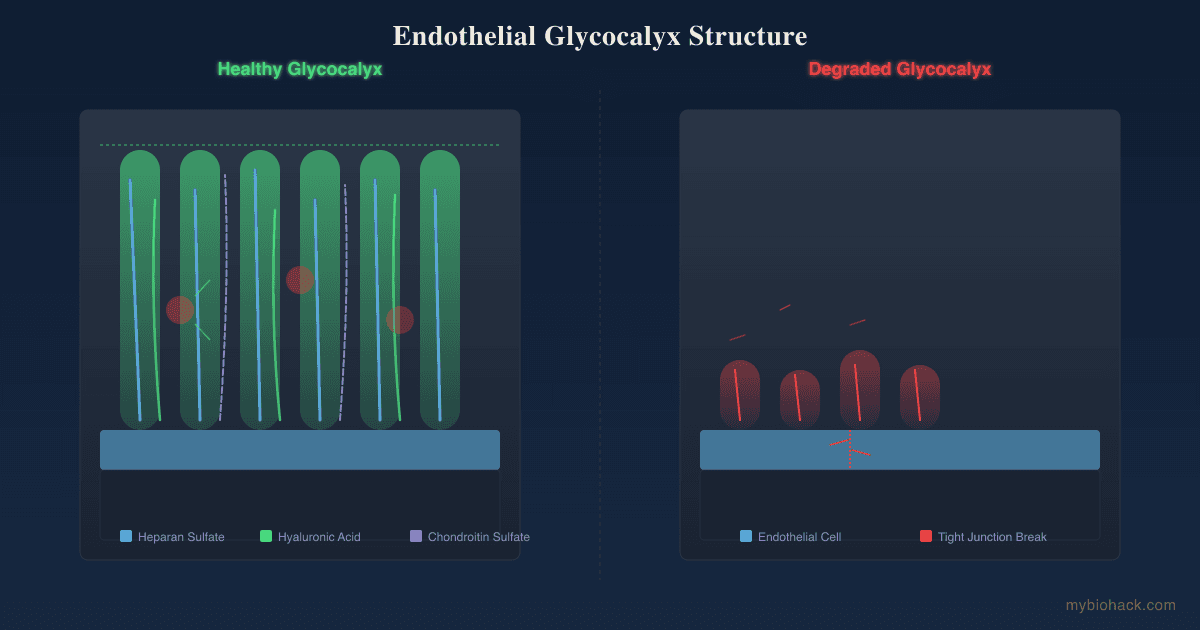
α7nAChR signaling does not only quiet macrophages, it also supports their phagocytic competence and the orderly cell-to-cell interactions needed to clean up debris and resolve an inflammatory episode. R
This is the part that matters for the Junction Dysfunction (JD) framework, the umbrella pathology Jacob describes when the glycocalyx breaks down and the body gets stuck in chronic inflammation.
In Jacob's model, without proper α7nAChR activation, macrophages do not regain the phagocytic ability to clear the debris generated during inflammatory cascades, so the wound healing cycle never finishes.
Cholinergic signaling through α7 also governs how monocyte-derived macrophages migrate during acute inflammation, which is another way the vagus shapes whether an inflammatory event resolves cleanly or smolders. R
Why Low Vagal Tone Drives Systemic Inflammation
Vagal tone is not an abstraction, it is measurable.
Heart Rate Variability (HRV) is the beat-to-beat variation in your heart rhythm, and the high-frequency component of HRV is a validated readout of parasympathetic (vagal) activity. R

When vagal tone is high, the cholinergic brake is online.
When vagal tone is low, the brake is weak, and the data show this is exactly when inflammation runs hot.
In a large, nationally representative sample, high-frequency HRV was inversely related to IL-6, C-reactive protein, and fibrinogen, meaning lower vagal tone tracked with higher inflammation. R
The Heart and Soul Study found the same inverse relationship between HRV and both CRP and IL-6 even after adjusting for covariates. R
Midlife cohort data continue to show that lower HRV predicts higher circulating inflammatory markers. R
This is the vagal anti-inflammatory pathway showing up in human population data, not just in animal models. R
There is a JD-specific reason the brake fails in post-viral and chronically inflamed people, and it is worth understanding because it explains why "just stimulate the vagus" is not always enough.
Chronic interferon signaling activates Indoleamine 2,3-Dioxygenase (IDO1), which shunts tryptophan down the kynurenine pathway and raises Kynurenic Acid (KYNA). R
KYNA is an antagonist at the α7nAChR.
So the same inflammatory state that should be calling for the cholinergic brake is simultaneously producing a metabolite that blocks the brake at the receptor.
Jacob's framing is that this is one of the core reasons the vagal anti-inflammatory pathway goes silent in chronic illness, and it ties the CAP directly to the tryptophan and kynurenine story covered in the JD guide chapter on tryptophan, NAD loss, and the vagus nerve.
Low gut serotonin compounds the problem, because a gut that cannot make serotonin loses one of the signals that keeps the vagus in a parasympathetic state, tipping the system toward sympathetic dominance. R
This is the same upstream driver discussed in the post on gut serotonin and mast cell activation.
When the brake stays off long enough, you get the chronic LPS exposure, inflammasome activation, and immune exhaustion that Jacob calls Micro-Sepsis (MSS), a term he coined for sub-lethal chronic sepsis that operates by the same mechanisms as acute sepsis without ever crossing the diagnostic threshold.
A leaky, inflamed microvasculature, which Jacob terms Transient Capillary Leak Syndrome (TCLS), keeps the endotoxin load high and the macrophages chronically activated, while the cholinergic brake that should resolve it is offline.
The CAP And Overlapping Conditions
A weak cholinergic brake shows up across most of the conditions covered on this site, which is part of why they cluster together in the same patients.
Long COVID (PASC) is associated with measurably impaired vagal activity, reduced HRV, and a sympathovagal shift toward sympathetic dominance, alongside elevated inflammatory markers. R R
This is consistent with the broader long COVID protocol and with the JD model in which spike-driven glycocalyx damage and persistent inflammation suppress the cholinergic pathway.
Postural Orthostatic Tachycardia Syndrome (POTS), which Jacob reframes as Vaso-Adaptive Disorder (VAD) and Adrenergic-Based Vaso-Adaptive Disorder (ABVAD), shows reduced cardiovagal HRV and attenuated parasympathetic tone, especially on standing. R R
In Jacob's framing the loss of microcapillary reserve and adrenergic-driven microthrombosis are upstream, and the blunted vagal tone is part of why the inflammatory load never clears (see the POTS root-causes post).
Myalgic Encephalomyelitis / Chronic Fatigue Syndrome (ME/CFS) shares the same autonomic signature of reduced vagal tone and sympathetic dominance against a backdrop of chronic immune activation.
Inflammatory Bowel Disease (IBD) is where the therapeutic side of this pathway has been tested directly.
Crohn's patients have blunted vagal tone, and in a pilot study, chronic vagus nerve stimulation restored vagal tone and put a majority of patients into clinical, biological, and endoscopic remission. R R
Rheumatoid Arthritis (RA) is the cleanest human proof of concept for the CAP.
Implanted vagus nerve stimulation reduced TNF production and attenuated disease severity in RA patients in the original mechanistic study. R
A more recent pivotal randomized controlled trial confirmed that vagus nerve stimulation improved RA disease activity versus sham. R
Mast Cell Activation Syndrome (MCAS) connects to this pathway through the receptor itself.
Mast cells express α7nAChR, and α7 activation suppresses IgE-mediated mast cell degranulation and histamine release in a dose-dependent way. R
This means a functioning cholinergic pathway is also a brake on mast cell flares, which links it to histamine intolerance, mast cell biology, and the nerve-to-mast-cell loop behind neurogenic inflammation.
The thread running through all of these is the same as the body's other built-in off switches, like the alpha-MSH and melanocortin anti-inflammatory system: when the brake fails, the condition that gets named depends mostly on which tissue is downstream.
How To Raise Vagal Tone And Alpha-7 Signaling
The goal is two-fold: raise the parasympathetic signal (more acetylcholine release, higher vagal tone) and keep the α7nAChR receptor available and functional.
A quick note before the protocol.
This is a chronic-illness audience, so the hormetic interventions below (cold, breathwork, exercise) must be dosed to your current capacity, because overdoing any of them backfires.

1. Slow Breathing (The Free First Move)
Breathing at roughly six breaths per minute is the most reliable, no-cost way to raise vagal tone.
Slow paced breathing at this rate increases HRV and enhances baroreflex sensitivity through a relative increase in vagal activity and a reduction in sympathetic activity. R R
In patients with chronic heart failure, slow breathing significantly increased baroreflex sensitivity, which is a direct measure of vagal control. R
This is the entry point because it costs nothing, can be done lying down on a bad day, and is the engine behind HRV biofeedback.
2. Cold Exposure To The Face
Cold applied to the face triggers the diving reflex, which is a direct vagal (parasympathetic) activation.
Cold water face immersion increases parasympathetic activity and accelerates post-exertional parasympathetic reactivation through stimulation of the trigeminal nerve. R R
For a debilitated patient, splashing cold water on the face or applying a cold pack to the cheeks and around the eyes is a far gentler entry than a full cold plunge.
3. Electrical Vagus Nerve Stimulation
Transcutaneous Auricular Vagus Nerve Stimulation (taVNS) stimulates the auricular branch of the vagus at the ear and is the most accessible form of direct electrical stimulation.
In randomized trials, taVNS reduced IL-6 and pro-inflammatory cytokine output in patients with active inflammation. R R
An Auricular Vagus Nerve Stimulator (taVNS) device clips to the ear and is the at-home version of the implanted devices used in the RA and Crohn's trials.
Pair it with slow breathing rather than treating it as a standalone fix.
4. Feed The Acetylcholine System
Acetylcholine is built from choline plus an acetyl group, so precursor availability matters.
Choline itself is not just a building block, it is a selective α7nAChR agonist that reduces TNF release through the same receptor the vagus uses. R
CDP-Choline (Citicoline): A bioavailable choline donor that raises central acetylcholine availability.
Alpha-GPC: A choline source that crosses the blood-brain barrier well and supports acetylcholine synthesis.
Acetyl-L-Carnitine: Supplies the acetyl group used to build acetylcholine and supports mitochondrial energy.
For the full breakdown of cofactors, foods, and pathways, see the deep dive on acetylcholine and the structural overview of nicotinic receptors.
5. Theanine, Omega-3s, And The Supportive Layer
L-Theanine: Shifts the system toward parasympathetic activity and is one of Jacob's listed acetylcholine-supportive compounds (see the post on theanine).
Omega-3 (DHA/EPA): Supplementation raises the high-frequency, vagally mediated component of HRV, consistent with increased parasympathetic tone. R
6. The Nicotine Debate
Nicotine is a direct nicotinic receptor agonist, including at α7, which is why it keeps coming up as a cholinergic biohack.
In randomized controlled trials, transdermal nicotine induced remission in active ulcerative colitis more often than placebo, a real-world demonstration of nicotinic anti-inflammatory signaling. R
Jacob frames low-dose nicotine (gum, lozenge, or patch, never smoking) as a cheap way to agonize α7nAChR while the vagal pathway is stuck, and he discusses its timing in the post on caffeine and nicotine power naps.
There is a big MAYBE here, because nicotine is addictive, can raise heart rate (a real problem in VAD/ABVAD), and is not appropriate for everyone.
A Nicotine Gum or Lozenge is the controllable, non-combusted form if it is trialed at all.
7. Galantamine (The Pharmacological Lever)
Galantamine is an acetylcholinesterase inhibitor that also positively modulates nicotinic receptors, and it raises cholinergic signaling centrally and through efferent vagal activity.
In a randomized trial in metabolic syndrome, galantamine lowered systemic inflammation and insulin resistance. R
It also reduced oxidative stress and improved cardiometabolic markers in a separate randomized trial. R
This is a more aggressive lever, and the organophosphate caveat below applies strongly to it.
8. Fix The Upstream JD Drivers
None of the above holds if the receptor is being antagonized and the glycocalyx is still degrading.
Lowering the IDO1 and kynurenine load takes KYNA off the α7nAChR, which is why the tryptophan, NAD, and vagus chapter is foundational here.
Rebuilding gut serotonin restores parasympathetic signaling from the gut, and reducing the endotoxin load from dysbiosis lowers the chronic LPS that keeps macrophages activated.
Supporting butyrate and other short-chain fatty acids helps the gut barrier and the broader anti-inflammatory tone the cholinergic pathway is trying to maintain.
What To Stay Away From
Chronic overexercise and overtraining (the single most common self-inflicted driver): pushing through post-exertional malaise damages the glycocalyx and worsens autonomic balance, which is why Jacob's position is do not tell a sick patient to exercise.
Combusted tobacco: any anti-inflammatory effect of nicotine is buried under the oxidative and vascular damage of smoking, so it is never the delivery method.
Organophosphate exposure (pesticides, some flame retardants): these paralyze the cholinergic system and push the body into sympathetic dominance, and Jacob's clinical observation is that people with organophosphate toxicity react badly to acetylcholine-boosting supplements with anxiety and brain fog.
Reflexive blind nicotine or galantamine use: in Jacob's experience, intolerance to cholinergics is usually a sign of underlying organophosphate poisoning rather than a problem with the cholinergic compound itself, so clearing the toxin comes first.
Stacking stimulants late in the day: caffeine and adrenergic load push the system sympathetic, which is the opposite of what you want when the goal is parasympathetic recovery.
Testing
Autonomic / Vagal Tone
HRV is the practical readout of vagal tone, and the high-frequency band specifically reflects parasympathetic activity. R
A chest-strap monitor gives the cleanest morning HRV data for tracking trends over weeks.
An HRV Chest Strap Monitor paired with a free HRV app is enough to see whether your interventions are moving vagal tone in the right direction.
A standing or NASA lean test (heart rate change on standing) is the cheap at-home screen for the VAD/ABVAD pattern that tracks with low vagal tone.
Blood And Urine Markers
The downstream inflammatory markers the cholinergic pathway is supposed to suppress are worth tracking, with the caveat that they are downstream readouts, not the root cause.
I use the Cardio Zoomer (Vibrant Wellness) to assess hsCRP and the metabolic and endothelial markers that move with chronic inflammation.
For the cytokine layer specifically (TNF-α, IL-1β, IL-6), I use the Immune Zoomer (Vibrant Wellness), which also covers the autoantibody and mast cell markers relevant to MCAS overlap.
The Cardio IQ Advanced Lipid Panel with Inflammation (Quest Diagnostics) is a more conventional alternative that includes hsCRP.
Mast Cell Markers (If MCAS Overlap)
Because α7 signaling restrains mast cells, the mast cell markers are worth checking when histamine symptoms are present.
I use the Tryptase (Quest Diagnostics) and Plasma Histamine (Quest Diagnostics) tests to assess mast cell burden.
Functional / Genetics
The cholinergic genes below are best read from raw genotyping data, and for the wider redox and detox SNPs that determine how you tolerate these interventions I cover testing routes in the genetics section.
Mechanisms Of Action
Simple:
- The vagus nerve is a brake on inflammation, and acetylcholine is the fluid in the brake line.
- The brake pad presses on a receptor called α7 that sits on the immune cells that make inflammation, and pressing it tells those cells to stop.
- When your vagal tone is low (low HRV), the brake is weak, so inflammation runs unchecked.
- You can press the brake with slow breathing, cold on the face, ear-clip vagus stimulation, choline, and (debatably) nicotine.
Advanced:
- The efferent reflex arc runs from the vagus to the celiac/splenic nerve, which releases norepinephrine onto β2-adrenergic receptors on ChAT-expressing CD4+ T cells in the spleen, which then secrete acetylcholine onto cytokine-producing macrophages. R
- α7nAChR signal transduction suppresses NF-κB nuclear translocation and engages the JAK2-STAT3 axis, collapsing transcription of TNF-α, IL-1β, IL-6, IL-8, and HMGB1 without affecting anti-inflammatory IL-10. R R
- Receptor-level antagonism by KYNA is the JD-relevant failure mode: chronic IFN drives IDO1, the kynurenine pathway raises kynurenic acid, and KYNA antagonizes α7nAChR, so the inflammatory state itself disables the brake even when acetylcholine is present. R
- Phagocytic competence depends on α7 signaling, so a silent cholinergic pathway leaves macrophages unable to clear debris, which in Jacob's model stalls the wound healing cycle and sustains TCLS and MSS. R
- Mast cell restraint occurs because mast cells express α7nAChR, and agonism suppresses IgE-mediated degranulation, linking cholinergic tone to histamine load. R
Genetics
CHRNA7
CHRNA7 encodes the alpha-7 subunit of the nicotinic acetylcholine receptor, the exact receptor that mediates the cholinergic brake.
Variants in CHRNA7 and its partially duplicated, human-specific gene CHRFAM7A alter the anti-inflammatory response, and CHRFAM7A acts as a dominant-negative that can blunt α7 channel function. R R
Polymorphisms in both genes have been associated with an increased inflammatory response in human immune cells, which is one inherited reason some people have a weaker cholinergic brake. R
CHRM2
CHRM2 encodes the M2 muscarinic acetylcholine receptor that mediates vagal slowing of the heart.
Variants in the acetylcholine pathway, including CHRM2, have been associated with differences in heart rate variability, meaning they help set your baseline cardiovagal tone. R
CHAT
CHAT encodes choline acetyltransferase, the enzyme that synthesizes acetylcholine in both neurons and the ChAT-positive T cells of the splenic circuit.
Reduced choline acetyltransferase capacity means less acetylcholine available to drive the pathway, and acetylcholine pathway genes including CHAT have been examined for their contribution to heart rate variability. R
ACHE
ACHE encodes acetylcholinesterase, the enzyme that breaks down acetylcholine and therefore sets how long the signal lasts.
rs17228616 sits in the 3'-UTR of ACHE and weakens regulation by miR-608, and carriers of the minor allele show higher acetylcholinesterase levels, which would shorten cholinergic signaling. R
BCHE
BCHE encodes butyrylcholinesterase, a second enzyme that hydrolyzes acetylcholine and helps clear organophosphates.
rs1803274 (the K-variant) reduces enzyme activity by roughly 30% and has been associated with dysregulated pro-inflammatory cytokine levels, which is relevant both to cholinergic tone and to organophosphate clearance. R
More Research
For biomarker and inflammation tracking I use the Immune Zoomer and Cardio Zoomer (Vibrant Wellness) to follow the cytokines the cholinergic pathway is meant to suppress, and an HRV Chest Strap Monitor to track vagal tone over time.
Galantamine's human trial data are promising but small, and the cardiometabolic and anti-inflammatory effects come from metabolic-syndrome populations rather than from post-viral cohorts, so its role in JD remains an extrapolation. R
KYNA antagonism of α7nAChR is, in Jacob's framing, one of the most underappreciated reasons the vagal anti-inflammatory pathway goes silent in chronic illness, and it argues for treating the tryptophan and kynurenine shunt as upstream of any vagal intervention. R
Organophosphate exposure is, in Jacob's clinical observation, a frequently missed reason patients fail to tolerate cholinergic support, so the organophosphate angle deserves more formal study in the post-viral population.
The implanted vagus nerve stimulation data in rheumatoid arthritis and Crohn's disease are the strongest human proof that switching this pathway back on changes disease course, and the open question is how much of that benefit non-invasive taVNS can reproduce at home. R R
The CAP overlaps mechanistically with the body's other anti-inflammatory off switches, including the glymphatic clearance system and the cell danger response, and reading them together gives a fuller picture of why these conditions cluster.
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Electrolyte Complex
1 scoop/day
CoQ10
200mg/day
Magnesium Glycinate
400mg at bedtime