Cell Danger Response: Why Chronic Illness May Be A Stuck Survival Program
By Jacob Gordon, INHC, FMT-CThis article contains affiliate links. As an Amazon Associate, MyBioHack earns from qualifying purchases at no extra cost to you. We only link products we research and stand behind.
The Cell Danger Response (CDR) is an evolutionarily conserved metabolic defense that cells activate when they detect a threat, and chronic illness may result when this program fails to shut off.
In this post, we will discuss the basics of CDR, the three stages of the healing cycle, what triggers it, how it involves mitochondria and purinergic signaling, which chronic conditions are linked to a stuck CDR, how the model connects to Junction Dysfunction, the salugenesis healing program, the suramin story, and how to support its resolution.

Basics Of The Cell Danger Response
The Cell Danger Response is a universal cellular defense mechanism first formally described by Robert Naviaux at UC San Diego in 2014.R
When a cell detects danger (infection, toxin, physical trauma, or even severe psychological stress), it shifts its entire metabolic program away from normal energy production and toward defense.
Under normal conditions, mitochondria fuse into long networks and generate ATP through oxidative phosphorylation to power the cell.
During CDR, mitochondria fragment into small spheres and switch to aerobic glycolysis, a less efficient but faster mode of generating energy that also produces reactive oxygen species (ROS) as antimicrobial weapons.R
The cell simultaneously releases ATP into the extracellular space, where it no longer acts as fuel but instead serves as a "danger signal" to neighboring cells and the immune system.
Cell membranes stiffen, lipid metabolism shifts toward ceramides and sphingolipids, and the cell essentially barricades itself.
This response is ancient and highly effective against acute threats.
The problem is that CDR was designed to turn on, neutralize the threat, and then turn off through a stepwise healing cycle.
When the off-switch fails, the body gets locked into a chronic state of cellular defense that looks, from the outside, like persistent multisystem illness.
The CDR is a unifying hypothesis, not settled consensus medicine, and it is best understood as a framework that ties together findings from mitochondrial biology, metabolomics, and immunology that is still being tested.
The Three Stages Of CDR
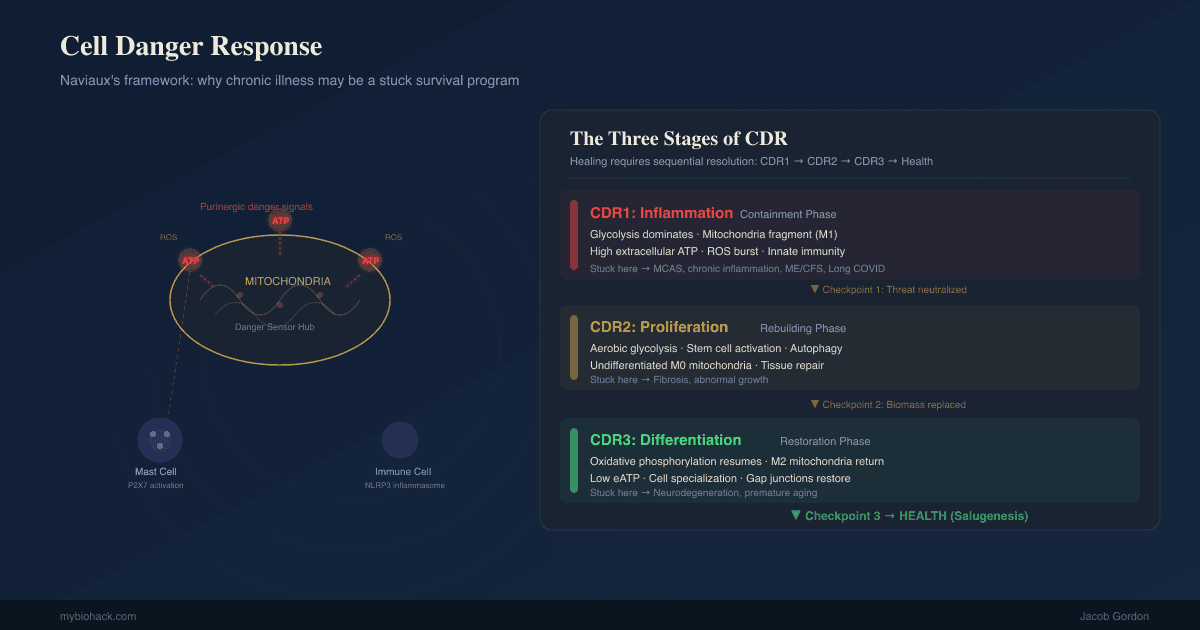
Naviaux's later work expanded the CDR model into a three-stage healing cycle, where each stage must fully resolve before the next can begin.R
Naviaux calls this healing program salugenesis, the active biological opposite of pathogenesis, a sequential process rather than a single event.RR
Each phase is governed by a different metabolic and mitochondrial program, and each must hand off cleanly to the next.R
If the danger signal never falls below threshold, the cell cannot progress, and that incomplete healing is what Naviaux argues drives both chronic disease and aspects of aging.R
CDR1: Innate Immunity And Acute Defense
CDR1 is the immediate "fight" phase triggered by threat detection.
Mitochondria fragment, shifting from oxidative phosphorylation to glycolysis.
Cells release ATP and other damage-associated molecular patterns (DAMPs) into the extracellular space.
The innate immune system activates, deploying mast cells, neutrophils, and macrophages.
Inflammation spikes as NF-kB signaling drives cytokine production.
ROS are generated intentionally as antimicrobial weapons.
Cell membranes stiffen to resist pathogen entry.
The NAD+/NADH ratio drops as resources are redirected away from normal metabolism.
If CDR1 resolves properly, the body transitions to repair.
If CDR1 gets stuck, the result is chronic inflammation, persistent immune activation, and the hallmark presentation of conditions like mast cell activation syndrome (MCAS) and SALI.
CDR2: Adaptive Immunity And Repair
CDR2 is the "rebuild" phase.
Stem cells activate and begin repairing damaged tissue.
Surviving cells dedifferentiate and divide to replace what was lost, and metabolism stays biased toward biosynthesis rather than efficient energy production.R
T helper cells and the adaptive immune system take over from innate responders.
Autophagy upregulates, clearing damaged organelles and intracellular debris.
New mitochondria are generated through biogenesis.
If CDR2 stalls, the persistent repair signaling can drive fibrosis (excessive scar tissue formation) and aberrant cell proliferation.
CDR3: Recovery And Reintegration
CDR3 is the "all clear" phase that returns the organism to health.
Newly made cells mature, re-specialize, reconnect to their neighbors, and the tissue restores its architecture, its autonomic wiring, and its relationship with the microbiome.R
Mitochondria fuse back into elongated networks and resume full oxidative phosphorylation.
The nervous system recalibrates from sympathetic dominance back toward parasympathetic tone.
The vagus nerve signals safety to the body, restoring coregulation capacity.
The microbiome rebalances.
Social engagement returns (this is a biological, not psychological, process).
If CDR3 fails, the person may appear physically recovered but remains withdrawn, fatigued, and unable to tolerate normal stimuli.
Many people with long-standing chronic illness are stuck at the CDR1/CDR2 boundary, unable to fully transition into repair, let alone recovery.R
What Triggers The Cell Danger Response
Any threat that damages cells or signals potential damage can initiate CDR.
Common triggers include: (not exclusive list)
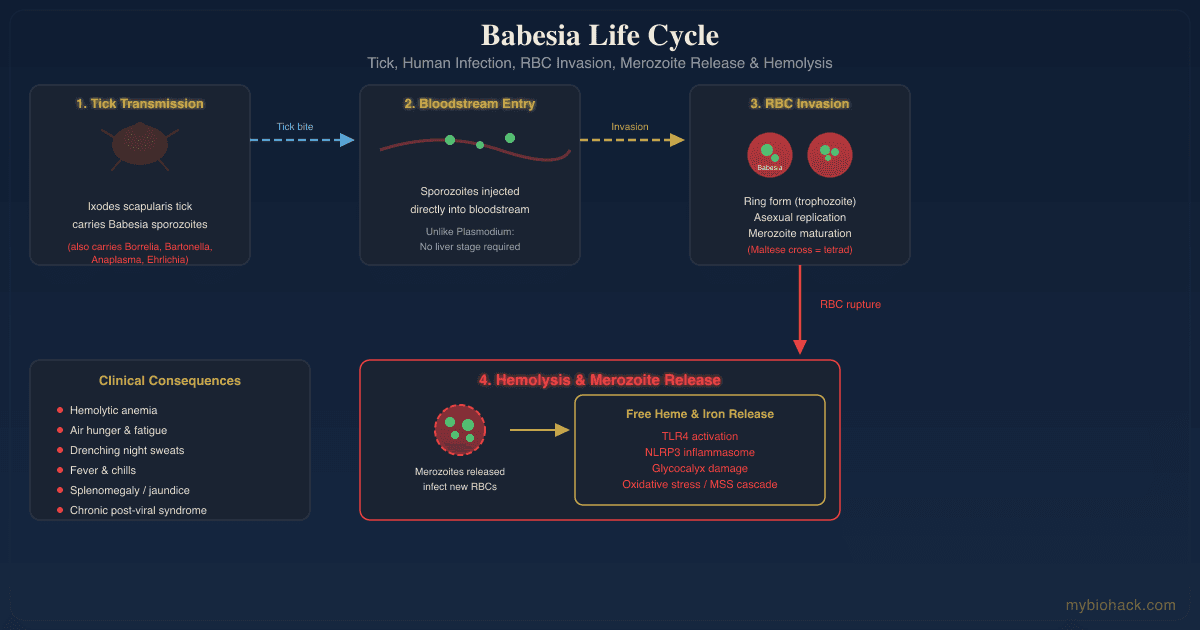
- Bacterial infections (LPS from gram-negative bacteria is a potent CDR trigger via TLR4 activation)R
- Chemical exposures (pesticides, solvents, heavy metals that damage mitochondrial membranes)R
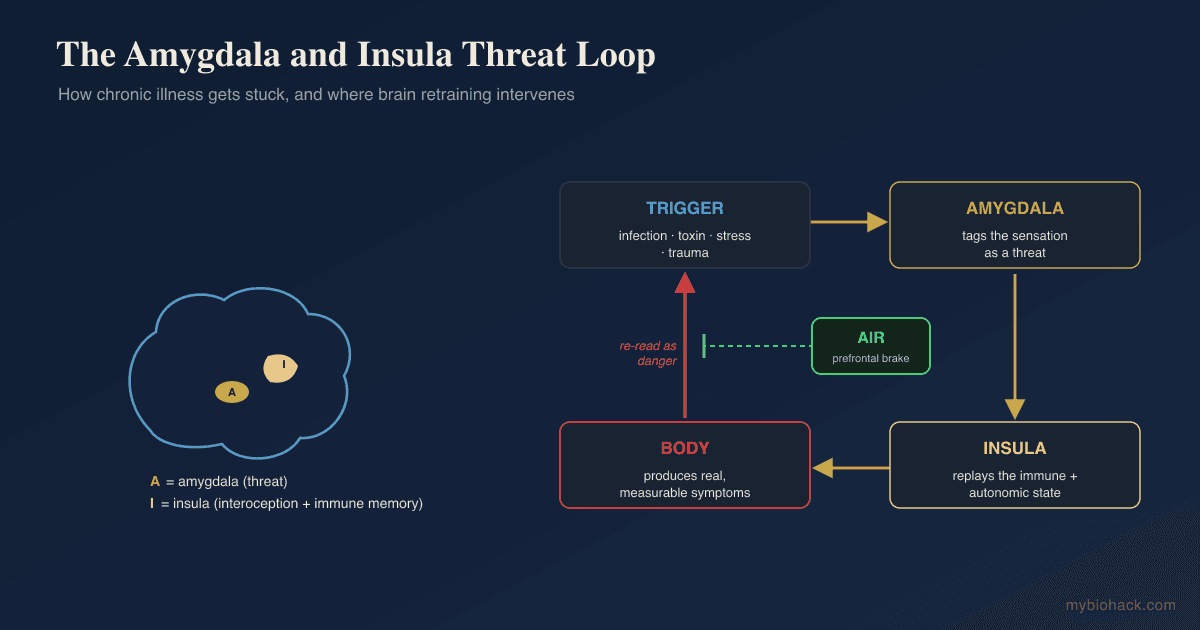
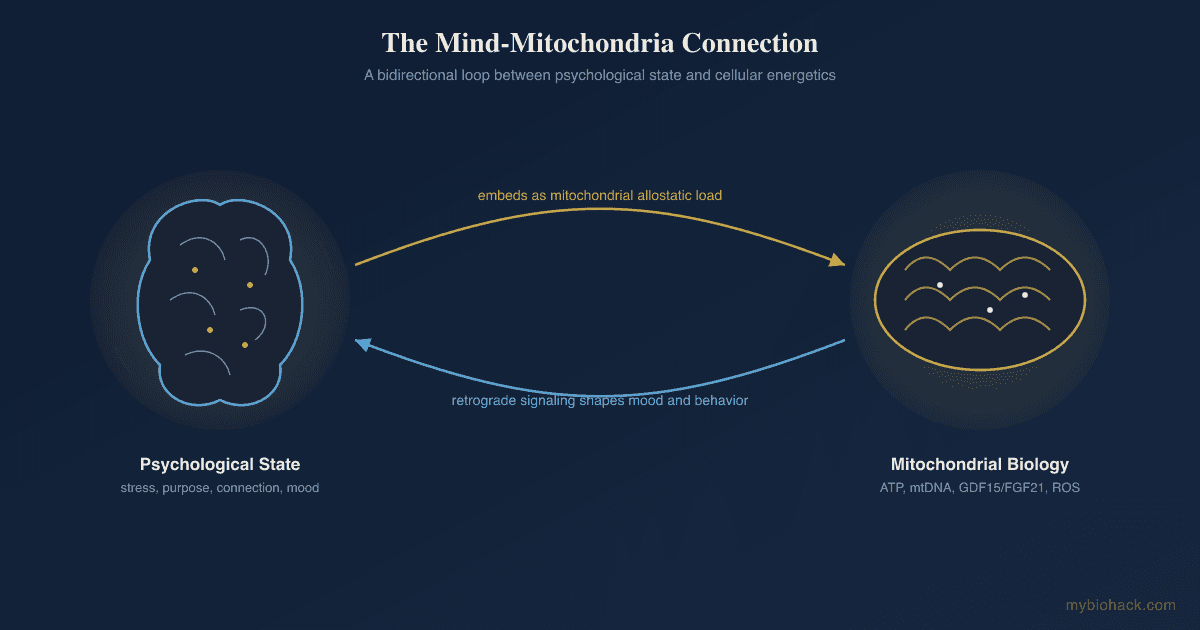
- Chronic psychological stress (sustained HPA axis activation converges on the same mitochondrial defense pathways)R
- Environmental biotoxins (water-damaged building exposure is one of the most common sustained CDR triggers in clinical practice)
- Mycotoxins (mold-derived toxins that directly damage mitochondrial electron transport chain complexes)R
- Physical trauma (traumatic brain injury, surgery, major tissue damage)
- Viral infections (SARS-CoV-2, EBV, HHV-6, and other persistent viruses that hijack mitochondrial dynamics)R
The critical insight is that the body does not distinguish between types of danger at the cellular level.
A mold exposure, a viral infection, and a severe emotional trauma all converge on the same mitochondrial defense switch.
This explains why patients with complex chronic illness often have multiple overlapping triggers, and why removing only one trigger sometimes fails to resolve symptoms.
CDR And Mitochondria
Mitochondria are the central executors of the Cell Danger Response.
They are not just "powerhouses of the cell" but are ancient danger sensors descended from alpha-proteobacteria that were engulfed billions of years ago.R
The CDR model reframes them as the cell's threat-monitoring and decision-making hub, sensing the physical, chemical, and microbial conditions inside and around the cell and deciding whether to invest in energy production or defense.R
Under normal conditions, mitochondria exist in fused, elongated networks that maximize oxidative phosphorylation efficiency.
When CDR activates, dynamin-related protein 1 (DRP1) drives mitochondrial fission, fragmenting these networks into small spheres.R
Fragmented mitochondria shift from producing ATP internally to releasing ATP externally as a purinergic danger signal.
They simultaneously increase ROS production, which serves as both an antimicrobial weapon and an intracellular alarm.
The electron transport chain partially uncouples, and NAD+ is consumed at accelerated rates by PARPs (poly ADP-ribose polymerases) for DNA repair and CD38 for immune signaling.R
This NAD+ depletion creates a cellular energy crisis that compounds over time.
This is also why fatigue is not a side effect in these conditions but a feature, because when mitochondria choose defense over energy the whole organism runs on a smaller power budget.
Tryptophan is shunted away from serotonin production and into the kynurenine pathway, producing neuroactive metabolites like quinolinic acid (neurotoxic) at the expense of mood and sleep.R
Lipid metabolism also shifts during CDR.
Ceramide and sphingolipid levels rise, stiffening cell membranes to prevent pathogen entry but also reducing membrane fluidity needed for normal receptor signaling.R
Cholesterol synthesis increases as membranes are reinforced.
This is why many chronically ill patients show elevated cholesterol on labs, not from dietary intake, but from a defensive metabolic program that is still running.
It is worth contrasting the stuck CDR with mitohormesis, the beneficial response where a mild, transient mitochondrial stress leaves the cell more resilient afterward.R
Mitohormesis is the healthy, self-limiting version of this signaling, which is the whole logic behind hormesis as a tool, and the CDR is what happens when the same machinery gets stuck on instead of resolving.
CDR And Purinergic Signaling
Purinergic signaling is the communication system that cells use to broadcast danger, and it is the primary language of the CDR.R
Under normal conditions, ATP is kept inside cells at a concentration of approximately 5 millimolar.
When a cell is damaged, stressed, or dying, ATP leaks or is actively secreted into the extracellular space.
This extracellular ATP binds to purinergic receptors on neighboring cells, triggering inflammatory and defensive cascades.R
Outside the cell, that extracellular ATP (eATP) becomes a damage-associated molecular pattern (DAMP), one of the body's core danger alarms, which is why Naviaux frames eATP and purinergic signaling as the language the CDR is spoken in.RR
As long as eATP stays elevated, cells keep reading "danger" and stay locked in CDR1, unable to advance to repair.
P2X Receptors (Ionotropic)
The P2X7 receptor is the most important purinergic receptor in CDR.
When extracellular ATP binds P2X7, it opens a large-pore ion channel that allows potassium efflux and triggers assembly of the NLRP3 inflammasome.R
NLRP3 activation drives processing and release of IL-1beta and IL-18, two of the most potent pro-inflammatory cytokines.R
P2X7 activation on mast cells causes degranulation, releasing histamine and other inflammatory mediators.
P2Y Receptors (Metabotropic)
P2Y receptors are G-protein coupled receptors that respond to various nucleotides (ATP, ADP, UTP, UDP).
They modulate calcium signaling, cell migration, and tissue repair processes.
P2Y12 on platelets drives aggregation, contributing to the hypercoagulability seen in many CDR-associated conditions.
P1 Receptors (Adenosine)
As extracellular ATP is broken down by ectonucleotidases (CD39 and CD73), it is converted to adenosine.
Adenosine binds P1 receptors (A1, A2A, A2B, A3), which are generally anti-inflammatory and represent the body's attempt to resolve CDR.R
This conversion is itself a switch, because CD39 (ENTPD1) and CD73 (NT5E) step ATP down to ADP, then AMP, then adenosine, turning a pro-inflammatory danger signal into a pro-healing one.RR
Impaired ectonucleotidase activity biases the whole system toward a persistent danger state.
The balance between ATP signaling (pro-inflammatory) and adenosine signaling (anti-inflammatory) determines whether CDR resolves or persists.
Suramin: The Antipurinergic Drug
Suramin is a century-old antiparasitic drug that blocks purinergic receptors nonselectively.
This is the logic behind antipurinergic therapy (APT), the idea that blocking the stuck purinergic signal should let cells stand down.R
Naviaux demonstrated that suramin corrected autism-like behaviors in a maternal immune activation mouse model by resetting purinergic signaling.R
In that maternal immune activation model, suramin corrected 16 separate multisystem abnormalities that defined the autism-like phenotype.R
A single dose restored normal social behavior and metabolism even in 6-month-old adult mice, suggesting the abnormalities were a maintained state rather than permanent damage.R
That word, maintained, is the whole thesis of the CDR, because something maintained can in principle be released.
In the small SAT-1 human trial (10 boys with autism spectrum disorder), a single low-dose suramin infusion produced measurable improvements in language, social interaction, and repetitive behaviors that lasted several weeks, with no serious adverse events.R
Suramin is not currently approved for CDR-related conditions and carries significant side effects at antiparasitic doses, but the research validates the purinergic model.
CDR And Chronic Illness
The central hypothesis of the CDR model is that many chronic, multi-system conditions represent a healing cycle that has stalled at one or more stages.
Each condition maps onto the CDR framework in a specific way.
ME/CFS (Myalgic Encephalomyelitis / Chronic Fatigue Syndrome)
Naviaux's 2016 metabolomics study of ME/CFS patients revealed a hypometabolic state strikingly consistent with a persistent CDR.R
Over 60 metabolic pathways were disrupted, with decreases in sphingolipids, phospholipids, and several amino acids.
The metabolic profile resembled dauer, a hibernation-like survival state seen in C. elegans worms under environmental stress.R
Roughly 80 percent of the measured metabolites were decreased rather than increased, a downshift rather than an inflammatory flare, and the signature was chemically consistent across patients even though the specific low metabolites differed by sex.R
The interpretation is that the body is not failing at metabolism, it is succeeding at a different goal, conservation and defense, at the expense of feeling well.
Independent metabolomics studies by Germain et al. and Tomas et al. confirmed similar disruptions in energy metabolism.RR
Long COVID
Long COVID presents a near-identical metabolic picture to ME/CFS in many patients.
SARS-CoV-2 directly damages mitochondria and activates purinergic signaling through multiple mechanisms, including spike protein interaction with P2X7.R
Viral persistence in tissue reservoirs (gut, brain, lung) provides an ongoing CDR trigger that prevents resolution.
The downstream measurements support a defended metabolic state, with long COVID patients showing impaired systemic oxygen extraction during exercise, consistent with mitochondria that are present but not producing energy normally.R
Their plasma carries signatures of mitochondrial dysfunction and impaired fatty acid metabolism, and measurably impaired mitochondrial function has been confirmed across several independent studies.RR
The overlap between Long COVID symptoms and CDR1/CDR2 stalling is significant: fatigue, brain fog, dysautonomia, exercise intolerance, and immune dysregulation.
CIRS / Mold Illness
CIRS (Chronic Inflammatory Response Syndrome) from water-damaged buildings is a textbook CDR trigger.
Mycotoxins directly poison mitochondrial electron transport chain complexes, forcing the cell into glycolytic defense.
Ongoing mold exposure provides a continuous CDR trigger that prevents any stage from resolving.
The characteristic lab findings in CIRS (elevated TGF-beta1, low alpha-MSH, elevated C4a, low VIP) map directly onto CDR1 persistence.
Autism Spectrum Disorder
Naviaux's suramin trial in boys with ASD demonstrated that purinergic signaling abnormalities may underlie some cases of autism.R
The maternal immune activation model proposes that prenatal infection or immune activation triggers a CDR in the developing fetal brain that persists postnatally.
This aligns with CDR3 failure, where the nervous system never fully recalibrates and social reintegration circuits remain impaired.
MCAS (Mast Cell Activation Syndrome)
Mast cells are key effectors of CDR1.
They release ATP, histamine, and inflammatory mediators when activated by purinergic danger signals.
MCAS may represent a stuck CDR1 state where mast cells remain hyperactivated because the extracellular ATP "danger" signal has not been cleared.R
ATP binding to P2X7 on mast cells triggers degranulation, which releases more ATP, creating a self-sustaining loop.
Additional CDR-Associated Conditions
Conditions potentially explained by a stuck CDR include: (not exclusive list)
- Fibromyalgia (central sensitization consistent with CDR1/CDR3 overlap)
- Gulf War Illness (chemical exposure as initial CDR trigger with persistent metabolic disruption)
- POTS (autonomic dysregulation consistent with CDR3 failure to recalibrate the nervous system)
How CDR Connects To Junction Dysfunction
If you have read the Junction Dysfunction (JD) framework on this site, the Cell Danger Response will feel familiar, because the two models describe the same stuck patient from different angles.
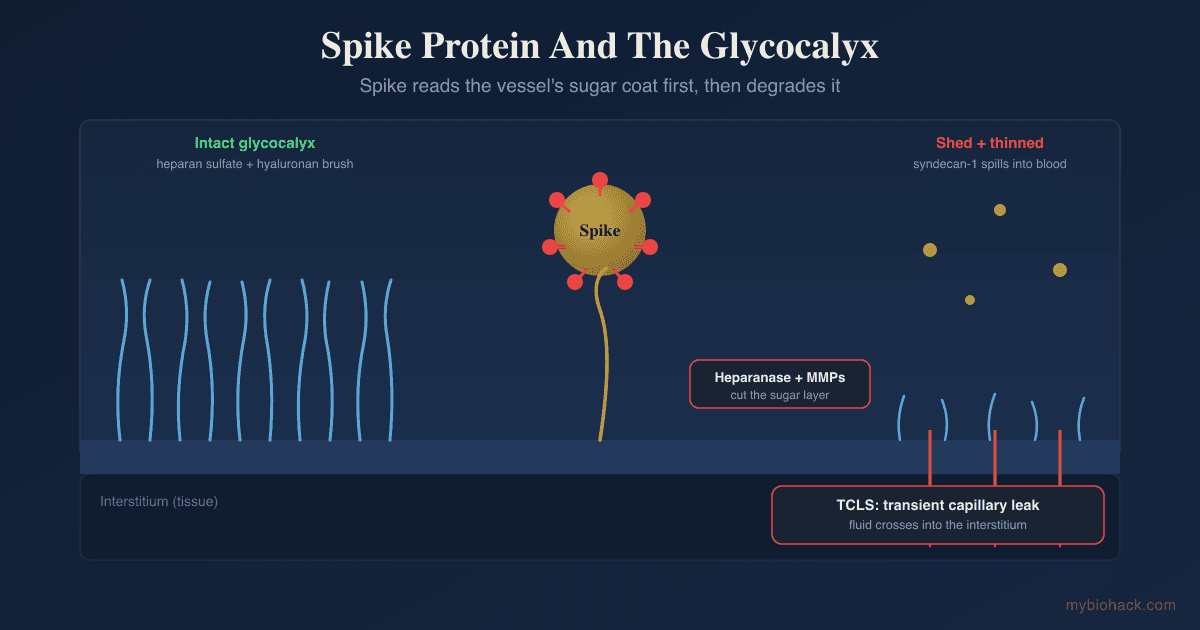
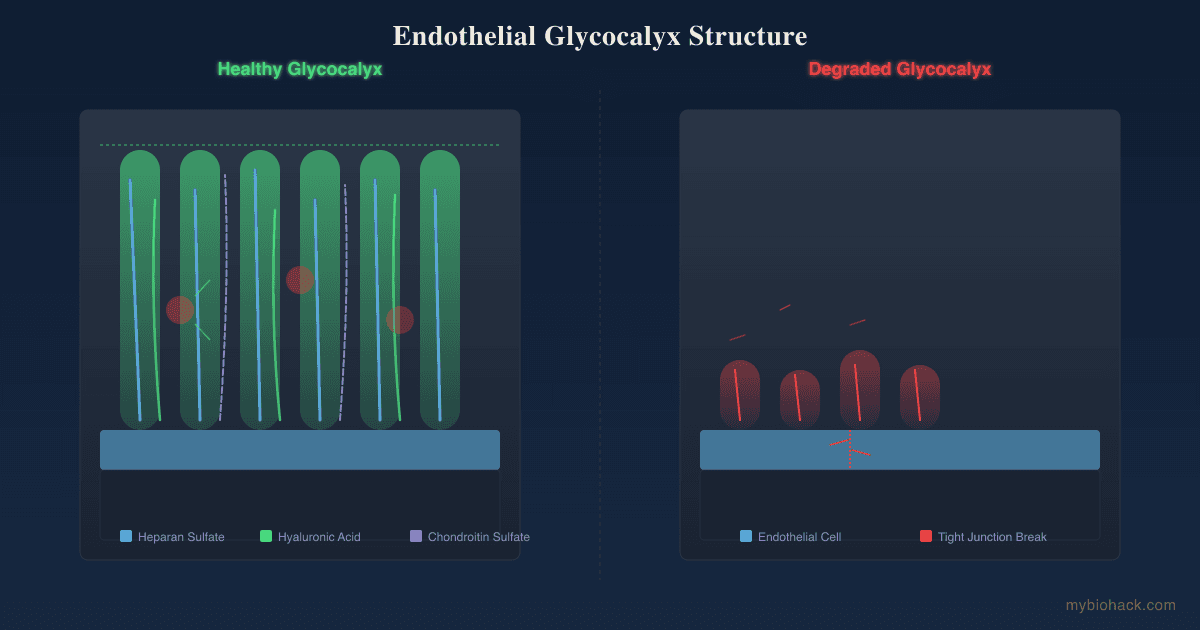
JD is the term I use for the umbrella pathology that begins when the glycocalyx, the protective sugar layer lining the blood vessels, becomes compromised.
Out of that degradation come two sub-pathologies I coined, Transient Capillary Leak Syndrome (TCLS) and Micro-Sepsis (MSS).
Here is where I think the CDR and JD interlock, and I want to be clear this is my hypothesis, not established science.
TCLS provides a continuous source of the danger signal that keeps the CDR switched on.
When fluid leaks at the microvascular level and cells sit in stagnant, hypoxic, electrolyte-disrupted tissue, they release ATP and generate the exact stress signals that hold P2X7 and the NLRP3 inflammasome active.
MSS supplies a second danger source, because endotoxin looping from a leaky gut keeps LPS and microbial patterns circulating, a separate parallel trigger for the same inflammasome that extracellular ATP drives.
In this framing, a degraded glycocalyx and the TCLS and MSS that follow are the upstream reason the CDR cannot get its "all clear," and the CDR is the metabolic program the body runs in response.
Naviaux's three phases also line up almost one to one with what I call Wound Healing Cycles (WHC), the staged healing sequence the body has to complete.R
People stuck in third-degree post-viral injury get parked in the hemostasis and inflammation stages and never reach proliferation and remodeling, which is the same failure as a CDR that cannot advance past CDR1.
This is also why I keep saying inflammation is not the root cause but the first stage of healing, and the CDR model says the same thing in its own vocabulary, that CDR1 is meant to be transient and the disease is the failure to leave it.
The mitochondrial and mast cell behavior I describe in mitochondria and mast cells in hypoxia is the JD-side view of the same mitochondrial switch the CDR describes.
For the post-viral treatment logic behind unsticking these triggers, see the best immunomodulators for post-viral illness and the chapter on latent viruses.
How To Support CDR Resolution
Supporting CDR resolution means helping the body complete the healing cycle rather than forcing any single stage.
The priority order matters: remove ongoing triggers first, then support mitochondrial recovery, then restore nervous system safety signaling.
1. Remove Ongoing Triggers
The CDR cannot resolve while the threat is still present.
Assess for and address ongoing exposures to mycotoxins, chronic infections, bioaccumulated toxins, and food-borne antigens.
Reduce LPS translocation from the gut by addressing dysbiosis and junction dysfunction.
Repair the glycocalyx, the protective sugar coating on cell surfaces that is degraded during CDR1 and must be restored for proper signaling.
2. Support Mitochondrial Recovery
Mitochondrial support is foundational because the CDR is fundamentally a mitochondrial program.
Supports electron transport chain Complex III, which is directly impaired during CDR.
Buffers the cellular energy charge so cells are less likely to dump ATP into the extracellular danger pool.
Replenishes the NAD+ pool that is depleted by PARP and CD38 activation during CDR.R
PQQ (Pyrroloquinoline Quinone):
Promotes mitochondrial biogenesis, which is needed during CDR2 to replace damaged mitochondria.
Transports fatty acids into mitochondria for beta-oxidation, supporting the metabolic shift back from glycolysis to oxidative phosphorylation.
Provides the sugar backbone for ATP synthesis, accelerating ATP pool recovery after CDR-driven depletion.
Acts as a mitochondrial antioxidant and cofactor for pyruvate dehydrogenase, the enzyme that channels glucose into the Krebs cycle instead of stopping at lactate.
3. Reduce Oxidative Stress
CDR1 intentionally generates ROS as a defense, but chronic ROS production damages the mitochondria themselves.
The master intracellular antioxidant that is profoundly depleted during sustained CDR.R
For a detailed overview of glutathione conjugation and Phase II detox pathways, see those dedicated posts.
A glutathione precursor that also modulates NMDA signaling and supports redox capacity in post-viral states.
A potent mitochondrial antioxidant that accumulates inside mitochondria at concentrations far exceeding plasma levels, scavenging ROS directly at the source.R
See the full melatonin post for dosing and safety considerations.
Activates SIRT1, which promotes mitochondrial biogenesis and supports the metabolic transition from CDR1 to CDR2.
4. Support Methylation And B Vitamins
Methylation is suppressed during CDR because the one-carbon metabolism that feeds the methyl cycle is redirected toward nucleotide synthesis for DNA repair and immune cell proliferation.R
Provides methylfolate, methylcobalamin, and P5P in their active forms, bypassing the common genetic polymorphisms (MTHFR, MTR, MTRR) that further impair methylation under CDR stress.
Required as a cofactor for over 300 enzymatic reactions, including multiple steps in the methyl cycle and ATP synthesis.
5. Restore Vagal Tone And Safety Signaling (CDR3)
CDR3 resolution requires the nervous system to shift from sympathetic defense back to parasympathetic restoration.
Vagal tone exercises, breathwork, and coregulation with safe people provide the biological "all clear" signal that CDR3 needs to complete.
This is not a psychological recommendation but a neurobiological requirement for completing the healing cycle.R
6. Pace To Avoid Re-Triggering CDR1
If exertion re-floods tissue with eATP and re-arms the inflammasome, then pacing is not laziness, it is keeping the danger signal below threshold long enough for cells to advance.
Stay under your post-exertional malaise threshold rather than pushing through it.
This is also why graded exercise in a defended metabolic state can deepen the problem rather than build capacity.
7. Fasting And Autophagy
Fasting and time-restricted eating stimulate autophagy, which is the central process of CDR2 that clears damaged organelles and allows new, healthy mitochondria to take their place.
Start conservatively with 12 to 14 hour overnight fasts and extend only as tolerated, because severely stuck CDR patients often have impaired gluconeogenesis and can crash from prolonged fasting.
8. NRF2 Activation (With Caution)
Sulforaphane and other NRF2 activators upregulate the antioxidant response element (ARE), boosting endogenous glutathione, superoxide dismutase, and catalase production.
Caution is warranted in CIRS patients, as discussed in the NRF2-CIRS post, because NRF2 activation can paradoxically increase inflammation in patients with active biotoxin exposure.
In a subset of very sensitive people NRF2 activation can backfire, so go slow and see why NRF2 activation can make you more sick before pushing it.
9. Circadian Alignment And Sunlight
Mitochondrial dynamics are circadian-regulated.
Morning sunlight exposure sets the master clock in the suprachiasmatic nucleus, which directly controls mitochondrial fission/fusion cycles and melatonin production timing.
Blue light at night disrupts this cycle and can perpetuate CDR by preventing the nighttime mitochondrial repair window.
10. Butyrate And Gut Barrier Support
Butyrate and other short-chain fatty acids produced by commensal bacteria fuel colonocyte mitochondria and strengthen the intestinal barrier.
A leaky gut continuously exposes the immune system to LPS and food antigens, providing an ongoing CDR trigger from the gut.
11. Community And Social Connection
This is not a motivational suggestion.
CDR3 explicitly requires social reintegration as a biological signal that the environment is safe.R
Isolation perpetuates CDR3 failure by maintaining the nervous system in a threat-detection mode.
What To Stay Away From
Things that can worsen or re-trigger CDR: (not exclusive list)
- Aggressive detox protocols (rapid mobilization of stored toxins without adequate binder and drainage support can re-trigger CDR1 as toxins redistribute)
- Excessive exercise (in a stuck CDR1/CDR2 state, high-intensity exercise generates massive ROS and ATP release, worsening the purinergic danger signal and causing post-exertional malaise)
- High-dose isolated antioxidants (ROS during CDR1 serve a defensive purpose, and completely quenching them prematurely can impair pathogen clearance)
- Ignoring ongoing mold exposure (no amount of supplementation will resolve CDR if the original trigger is still present in the living environment)
- Prolonged sympathetic stimulation (caffeine, stimulant medications, and chronic overwork keep the nervous system in threat-detection mode, blocking CDR3)
- Pushing through fatigue (fatigue during CDR is a protective signal that metabolic resources are depleted, and overriding it deepens the energy deficit)
Testing
There is no single "CDR test," but a combination of functional labs can reveal the metabolic signature of a stuck Cell Danger Response.
Blood And Urine Markers
Lactate and pyruvate can be elevated when cells lean on glycolysis instead of mitochondrial oxidation, a fingerprint of the defended metabolic state.R
Urinary organic acids reflect mitochondrial and microbial metabolism and can flag where the energy pathways are stalling.R
Mitochondrial Function And Organic Acids
The Cellular Zoomer (Vibrant Wellness) directly assesses mitochondrial function, organic acids, and oxidative stress markers, providing a snapshot of whether cells are in glycolytic defense or normal oxidative phosphorylation.
The Organic Acids panel (Vibrant Wellness) reveals disruptions in the Krebs cycle, fatty acid oxidation, and neurotransmitter metabolism that are hallmarks of CDR.
The Organic Acids Test (OAT) (Mosaic/Great Plains) is an alternative that also captures yeast and bacterial metabolites alongside mitochondrial markers.
Oxidative Stress
The Oxidative Stress panel (Vibrant Wellness) measures lipid peroxides, 8-OHdG (DNA damage), and antioxidant capacity, all of which are shifted during CDR1.
Immune And Inflammatory Markers
The Immune Zoomer (Vibrant Wellness) assesses cytokine panels, complement activation, and immunoglobulin patterns that reflect CDR1 immune activation.
Metabolic And Lipid Markers
The Cardio Zoomer (Vibrant Wellness) includes ceramide levels, which are elevated during CDR as part of the membrane-stiffening defense.R
Nutrient Depletion
The Nutrient Zoomer (Vibrant Wellness) captures the downstream nutrient deficiencies created by CDR, including B vitamins consumed by methylation demands, magnesium burned through by sympathetic activation, and antioxidants depleted by chronic ROS.
Toxin Burden
The Toxin Zoomer (Vibrant Wellness) screens for environmental chemicals that serve as ongoing CDR triggers (heavy metals, pesticides, phthalates, solvents).
The Mycotoxins Profile (RealTime Labs) is a focused alternative when mold is the suspected ongoing trigger.
Viral Reactivation
The Viral Infections Panel (Vibrant Wellness) checks for the latent viral reactivation that can keep danger signals flowing in post-viral CDR.
Gut And Microbiome
The Gut Zoomer (Vibrant Wellness) assesses dysbiosis, intestinal permeability, and pathogen presence, all of which contribute to CDR triggering via LPS translocation.
Methylation Genetics
The Methylation Genetics panel (Vibrant Wellness) identifies polymorphisms in MTHFR, MTR, MTRR, COMT, and other genes that impair the methylation cycle and make CDR resolution harder.
Comprehensive Baseline
The Foundation Zoomer (Vibrant Wellness) provides standard metabolic panels (CBC, CMP, thyroid, lipids) that can reveal the downstream metabolic effects of CDR (elevated cholesterol, low white blood cell subsets, thyroid suppression).
The Long COVID Bundle combines multiple relevant panels for patients with post-viral CDR presentation.
Provocation
A supervised cardiopulmonary exercise test can document the impaired oxygen extraction that defines the defended state, though it can provoke post-exertional malaise and should be approached cautiously.R
If you want help interpreting these results in the context of your own history, that is the kind of thing I work through on a consult.
Mechanisms Of Action
Simple:
- When a cell senses danger, it flips a metabolic switch from "grow and repair" to "defend and survive."
- The cell stops burning fuel efficiently and instead sends out chemical alarm signals (ATP) that tell every nearby cell to also go into defense mode.
- If the danger signal is never turned off, the body stays stuck in survival mode, which feels like chronic fatigue, pain, brain fog, and immune dysfunction.
- Recovery requires removing the original danger, restoring the cell's energy machinery, and then convincing the nervous system that it is safe.
Advanced:
- Mitochondrial Fission And Metabolic Switching DRP1-mediated mitochondrial fission fragments the network, reducing cristae surface area and shifting electron flow from Complex I/III/IV toward glycolysis and the pentose phosphate pathway, which generates NADPH for ROS production via NOX enzymes and ribose-5-phosphate for nucleotide synthesis needed for immune cell proliferation.R
- Purinergic Autocrine/Paracrine Loop Extracellular ATP activates P2X7 on the cell that released it (autocrine) and on neighboring cells (paracrine), triggering NLRP3 inflammasome assembly, gasdermin D pore formation, and IL-1beta/IL-18 maturation and release, while simultaneously driving potassium efflux that further destabilizes the cell membrane.RR
- Ectonucleotidase Resolution Switch CD39 (ENTPD1) and CD73 (NT5E) sequentially hydrolyze extracellular ATP to adenosine, converting a pro-inflammatory danger signal into an immunosuppressive, pro-healing adenosine signal, so impaired ectonucleotidase activity biases the system toward a persistent danger state.RR
- Kynurenine Pathway Diversion IDO1 (indoleamine 2,3-dioxygenase 1), upregulated by IFN-gamma during CDR1, diverts tryptophan from serotonin/melatonin synthesis into the kynurenine pathway, producing quinolinic acid (NMDA receptor agonist, neurotoxic) and depleting BH4 (tetrahydrobiopterin), which is required for monoamine neurotransmitter synthesis (dopamine, serotonin, nitric oxide).R
- Ceramide-Mediated Membrane Remodeling CDR1 activates acid sphingomyelinase, which cleaves sphingomyelin in the outer membrane leaflet to produce ceramide, creating rigid microdomains (lipid rafts) that cluster death receptors and restrict pathogen entry while simultaneously reducing receptor mobility needed for insulin signaling and neurotransmitter reuptake.R
- NAD+ Depletion Cascade PARP1 activation (for DNA repair) and CD38 upregulation (for immune calcium signaling) consume NAD+ at rates that exceed biosynthesis, collapsing the NAD+/NADH ratio, inhibiting SIRT1/SIRT3 deacetylase activity (which normally promotes mitochondrial fusion, fatty acid oxidation, and anti-inflammatory gene expression), and creating a self-reinforcing metabolic trap.R
- Sequential Salugenesis And The Integrated Stress Response Healing runs as ordered phases (CDR1, CDR2, CDR3) governed by distinct metabolic programs, and the integrated stress response (eIF2-alpha phosphorylation and ATF4 induction) is one of the conserved pathways that gates the transition out of the defended state.RR
Genetics
P2RX7 (P2X7 Receptor)
This gene encodes the P2X7 purinergic receptor, the primary sensor for extracellular ATP danger signaling.
Gain-of-function variants increase receptor sensitivity, meaning lower levels of extracellular ATP can trigger NLRP3 inflammasome assembly.
Loss-of-function variants impair the ability to mount an acute CDR, which may increase susceptibility to intracellular infections.
rs3751143 (Glu496Ala) is a loss-of-function variant that reduces P2X7 channel and pore activity and alters ATP-driven cytokine release, one reason individuals differ in how strongly they sustain the CDR.R
Polymorphisms in this gene are associated with:
NLRP3 (Inflammasome)
The NLRP3 gene encodes the sensor component of the inflammasome that is assembled downstream of P2X7 activation during CDR1.
Gain-of-function variants cause constitutive inflammasome activation, mimicking a permanently stuck CDR1.
These variants present clinically as cryopyrin-associated periodic syndromes (CAPS).
MTHFR And Methylation Genes
Variants in MTHFR (C677T, A1298C), MTR, and MTRR reduce methylation efficiency, which is already suppressed during CDR.
Patients with these polymorphisms under CDR stress experience compounded methylation deficiency, impairing DNA repair, neurotransmitter synthesis, and detoxification.
SOD2 (Manganese Superoxide Dismutase)
SOD2 encodes the primary mitochondrial antioxidant enzyme that converts superoxide (generated intentionally during CDR1) into hydrogen peroxide for safe disposal.
The Ala16Val polymorphism (rs4880) alters mitochondrial import efficiency and enzyme activity.
Reduced SOD2 activity during CDR allows superoxide to accumulate and damage mitochondrial DNA, creating a vicious cycle of CDR re-triggering.R
NT5E (CD73)
NT5E encodes CD73, the ectonucleotidase that completes the conversion of AMP to adenosine.
Reduced CD73 activity slows the switch from the ATP danger signal to the adenosine "calm and heal" signal.
Lower ectonucleotidase function is expected to bias the purinergic balance toward a persistent danger state.R
HLA-DR (Immune Recognition)
HLA-DR genes determine which antigens the adaptive immune system can recognize.
Certain HLA-DR haplotypes (notably 4-3-53, 11-3-52B, and others identified in the Shoemaker CIRS protocol) impair clearance of biotoxins, creating a genetic predisposition to CDR persistence from mold and other environmental triggers.
More Research
- Adenosine receptor signaling is the resolution arm of the purinergic system, and how A2A and A2B receptor tone shapes recovery from a stuck CDR is an open and clinically interesting question.R
- Ceramide accumulation during CDR contributes to insulin resistance independently of body composition, which may explain the metabolic syndrome overlap seen in many chronically ill patients.R
- Extracellular ATP acting through P2X7 receptors is a primary driver of neuroinflammation and has been implicated in Alzheimer's disease, multiple sclerosis, and neuropathic pain.R
- Impaired mitochondrial oxidative phosphorylation and increased glycolysis have been confirmed in peripheral blood mononuclear cells from ME/CFS patients using Seahorse metabolic flux analysis.R
- Naviaux argues that incomplete healing and a chronically engaged CDR contribute to aspects of biological aging, linking chronic illness and longevity biology under one mechanism.R
- Plasma metabolomics in ME/CFS patients revealed disturbances in phospholipid, sphingolipid, cholesterol, purine, microbiome, and pyrroline-5-carboxylate/proline pathways, all consistent with a coordinated CDR.R
- Purinergic signaling through P2 receptors regulates virtually every organ system, including the nervous, immune, cardiovascular, and gastrointestinal systems, making it a central hub for multi-system dysfunction.R
- Salugenesis as a drug target is the forward-looking idea, that the goal is not to suppress the CDR but to help it complete its sequence, and which levers safely accelerate CDR3 is largely unexplored.R
- Sex differences in the ME/CFS metabolome were a consistent finding, with men and women showing the same overall downshift through different specific metabolites, which has real implications for how testing and treatment should be personalized.R
- The healing cycle (CDR1 to CDR2 to CDR3 to health) is a sequential process where each stage must resolve before the next can begin, and therapeutic interventions that are beneficial in one stage can be harmful in another.R
- The metabolomic profile of ME/CFS patients matches a hypometabolic "dauer"-like state, with over 20 biochemical pathways showing decreases of 60 to 80 percent from healthy controls.R
- A single intravenous dose of suramin (20 mg/kg) produced measurable improvements in language, social interaction, and repetitive behaviors in boys with autism spectrum disorder, with effects lasting 5 to 8 weeks before wearing off.R
- For BDNF support during CDR3 neurological recovery, see the dedicated post on brain-derived neurotrophic factor strategies.
- For comprehensive baseline metabolic evaluation, I use the Foundation Zoomer alongside condition-specific panels.
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Glutathione (Liposomal)
500mg 2x/day
Activated Charcoal
500mg away from food/meds
NAC
600mg 2x/day