Babesia (Babesiosis): The Malaria-Like Tick-Borne Infection In Chronic Lyme
By Jacob Gordon, INHC, FMT-CThis article contains affiliate links. As an Amazon Associate, MyBioHack earns from qualifying purchases at no extra cost to you. We only link products we research and stand behind.
Babesia is a protozoan tick-borne parasite that infects red blood cells and causes hemolytic anemia, flu-like symptoms, air hunger, and night sweats, and it commonly co-infects people who already have Lyme disease or other vector-borne infections.
In this post, we will discuss the basics of Babesia, what causes babesiosis, its symptoms and overlapping conditions, testing options, treatment approaches including both pharmaceutical and botanical options, what to avoid, mechanisms of action, and relevant genetics.

Basics Of Babesia
Babesia is a genus of protozoan parasites belonging to the phylum Apicomplexa, the same phylum that includes Plasmodium (the cause of malaria). R
These are piroplasms that exclusively infect erythrocytes (red blood cells) and replicate asexually inside them before bursting out to invade new cells. R
Over 100 species of Babesia have been identified worldwide, but only a handful are known to cause human disease. R
The most important human-infecting species are Babesia microti (the primary cause in the United States, especially the Northeast and upper Midwest), Babesia duncani (found on the West Coast), Babesia divergens (the primary cause in Europe), and Babesia venatorum (found in Europe and Asia). R
Babesia is transmitted primarily by Ixodes scapularis ticks (the same vector that carries Borrelia burgdorferi which causes Lyme disease), though Dermacentor albipictus has been implicated as a vector for B. duncani. R
Transmission can also occur through blood transfusion, organ transplantation, and vertical transmission from mother to fetus during pregnancy. R
The parasite's life cycle involves both a vertebrate host (rodents, deer, cattle, humans) and the tick vector, where sexual reproduction occurs. R

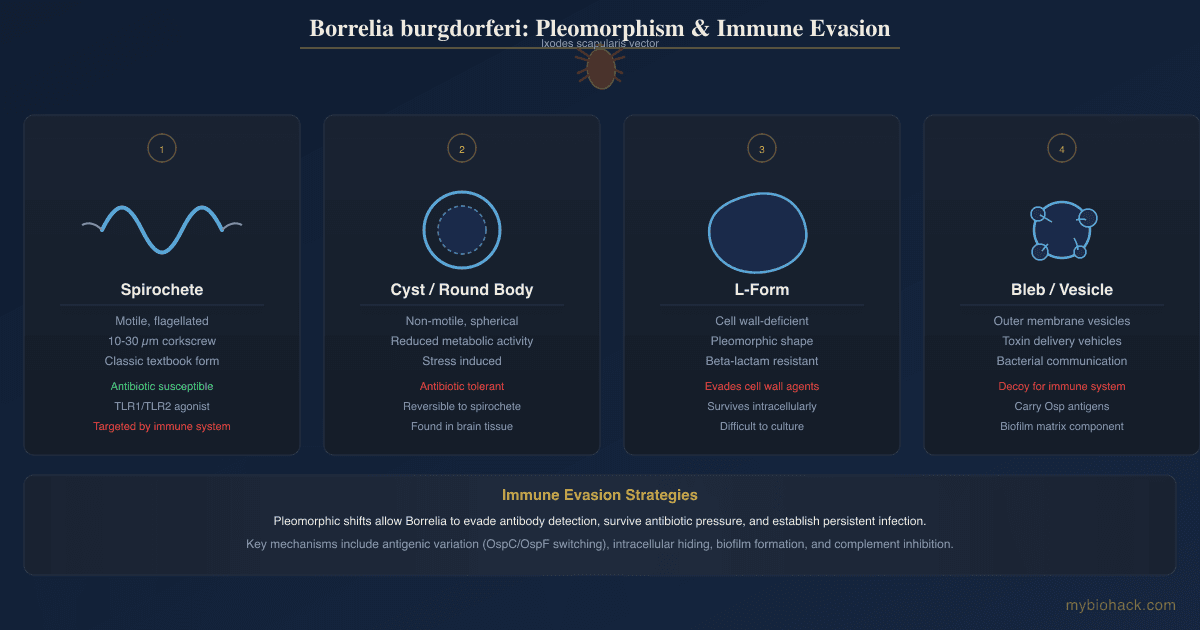
Pleomorphism And Terrain
Jacob's framing: Babesia, like other tick-borne pathogens, pleomorphs in response to its environment. R
The terrain of the host determines whether the infection remains subclinical, becomes acute, or establishes a persistent low-grade state.
This is consistent with the Bechamp-leaning view that pathogenicity is not fixed but emerges from the relationship between the microbe and its environment.
In the context of Junction Dysfunction (JD), the presence of Micro-Sepsis (MSS), glycocalyx damage, and immune dysregulation creates a terrain that allows Babesia to persist and evade clearance.
What Causes Babesiosis
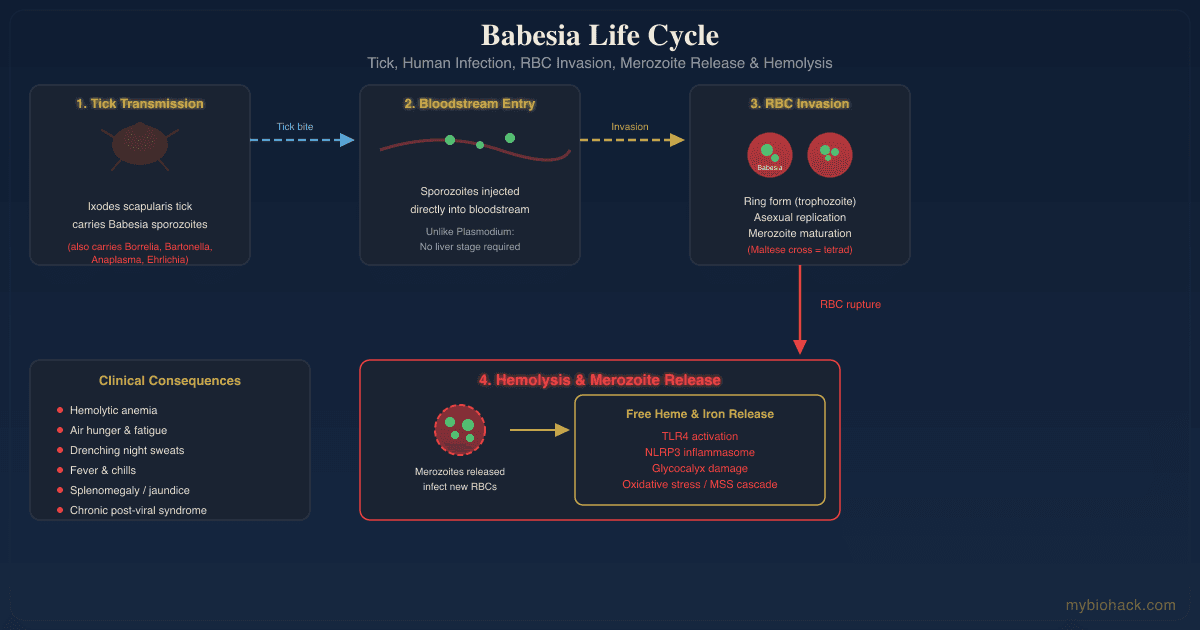
Babesiosis is caused by the inoculation of Babesia sporozoites into the bloodstream through the bite of an infected tick. R
The sporozoites enter red blood cells directly (unlike Plasmodium, which first passes through the liver) and begin asexual reproduction. R
Within the erythrocyte, the parasite matures from a trophozoite (ring form) into a merozoite, which then ruptures the cell and infects new red blood cells. R
This cycle of invasion, replication, and rupture drives the hemolytic anemia and systemic inflammation that characterize the disease. R
Risk Factors
Asplenia (surgical or functional): The spleen is critical for clearing Babesia-infected red blood cells.
Asplenic patients develop severe, often fatal disease. R
Immunosuppression: HIV/AIDS, rituximab therapy, B-cell malignancies, organ transplantation, and chemotherapy all increase risk of severe and relapsing babesiosis. R
Advanced age: Older adults (over 50) have higher risk of severe disease due to age-related immune decline. R
Co-infection with Lyme disease: Up to 23% of babesiosis patients also have concurrent Lyme disease, and co-infected patients experience more symptoms for longer duration than either infection alone. R
Blood transfusion: Babesia is the most commonly reported transfusion-transmitted parasite in the United States. R
Living or traveling in endemic areas: The Northeast (Nantucket, Martha's Vineyard, Cape Cod, Long Island, Connecticut), upper Midwest (Wisconsin, Minnesota), and West Coast (California) in the US, plus parts of Europe and Asia. R
The Acute Presentation
Acute babesiosis resembles malaria: high fever, chills, sweats, headache, myalgia, fatigue, and hemolytic anemia. R
Symptoms typically appear 1 to 4 weeks after a tick bite, though many patients do not recall a bite. R
Severe cases can involve jaundice, dark urine, splenomegaly, hepatomegaly, acute respiratory distress syndrome, disseminated intravascular coagulation, and death. R
The Chronic / Persistent Presentation
Chronic babesiosis is far more common in the functional medicine and chronic Lyme population than mainstream infectious disease acknowledges.
Patients may have low-grade or intermittent parasitemia that produces ongoing symptoms without meeting the threshold for acute diagnosis. R
Persistent parasitemia after acute babesiosis has been documented, with Babesia DNA detectable by PCR for months after treatment. R
Immunocompromised patients are at highest risk for relapsing and persistent infection, but immunocompetent individuals can also carry subclinical parasitemia. R
This persistent low-grade state drives ongoing hemolysis, oxidative stress, and immune activation that contributes to the JD cascade.
Babesia, Hemolytic Anemia, And The Glycocalyx
The hemolytic anemia in babesiosis has two components: direct parasite-mediated RBC lysis and secondary immune-mediated hemolysis.
Warm Autoimmune Hemolytic Anemia (wAIHA) has been increasingly recognized as a complication of Babesia infection. R
Babesia-triggered AIHA requires corticosteroids in addition to antiparasitic therapy for resolution. R
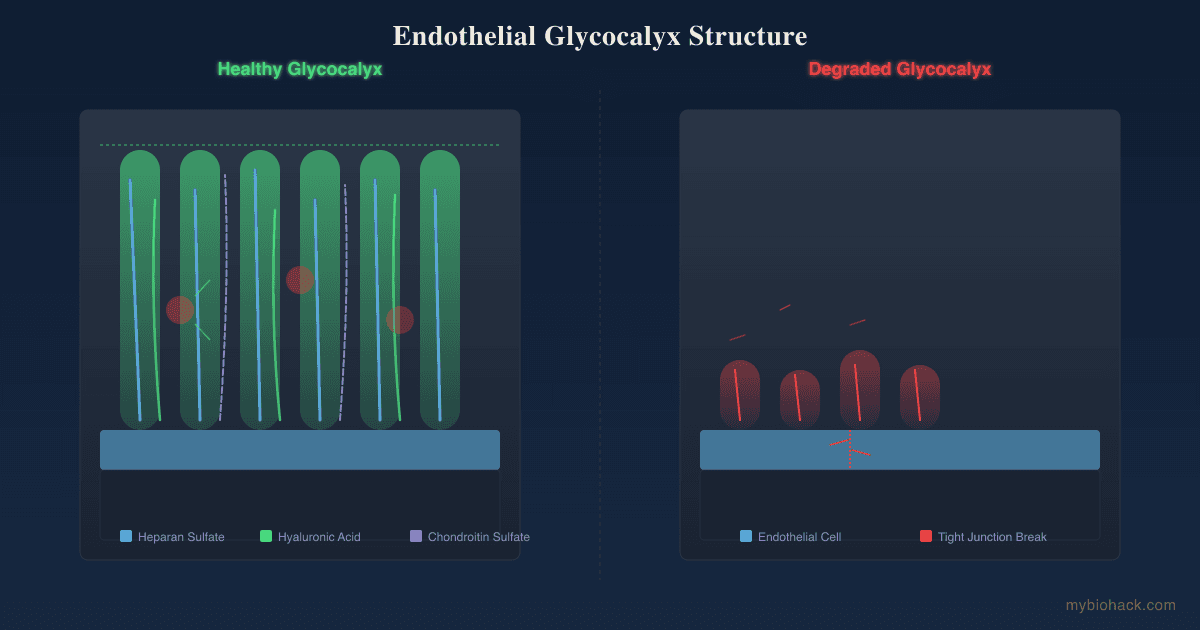
From the JD perspective, the hemolysis from Babesia generates massive oxidative stress in the form of free heme and iron release, which directly damages the glycocalyx.
Free heme activates TLR4 signaling and drives NLRP3 inflammasome activation, both of which are core mechanisms in MSS. R
The oxidized RBC debris also activates neutrophils to release Neutrophil Extracellular Traps (NETs), which Jacob hypothesizes is the true source of the "herx" reaction during treatment.
This creates a vicious cycle: Babesia causes hemolysis, hemolysis feeds oxidative stress, oxidative stress degrades the glycocalyx, glycocalyx loss impairs immune surveillance, and impaired clearance allows Babesia to persist.
Symptoms Of Babesiosis
Symptoms (not exclusive list):
- Air hunger / shortness of breath (from anemia and reduced oxygen-carrying capacity)
- Chills and sweats (often drenching, drenching night sweats are a hallmark)
- Dark urine (from hemoglobinuria, indicating intravascular hemolysis)
- Fatigue (often severe and disproportionate, similar to ME/CFS)
- Fever (intermittent or continuous, can reach 104F or higher)
- Headache (frontal or global, often severe)
- Jaundice (from bilirubin overload from RBC breakdown)
- Malaise (generalized sick feeling)
- Muscle and joint pain (myalgia and arthralgia)
- Nausea, vomiting, abdominal pain (from splenic congestion or liver involvement)
- Relative bradycardia (temperature-pulse dissociation, a clinical clue) R
- Splenomegaly (palpable spleen on exam)
- Tachycardia (compensatory for anemia)
- Thrombocytopenia (low platelets, common on CBC)
In chronic low-grade babesiosis, the symptom picture overlaps heavily with:
- ME/CFS (post-exertional malaise, brain fog, unrefreshing sleep)
- POTS / VAD (dizziness on standing, inappropriate tachycardia)
- MCAS (histamine intolerance, flushing, food sensitivities)
- Internal tremors and body buzzing (common in tick-borne illness clusters)
Babesia And Overlapping Conditions
Lyme Disease (Borrelia burgdorferi)
Babesia is the most common co-infection in Lyme disease patients, with co-infection rates estimated at 10 to 23% in endemic areas. R
Co-infected patients experience more severe symptoms and longer duration of illness than those with Lyme alone. R
Babesia should be suspected when a Lyme patient does not respond to standard antibiotic therapy or has atypical symptoms like night sweats, air hunger, or hemolytic anemia. R
See our full post on Lyme co-infections and Bartonella for more detail.
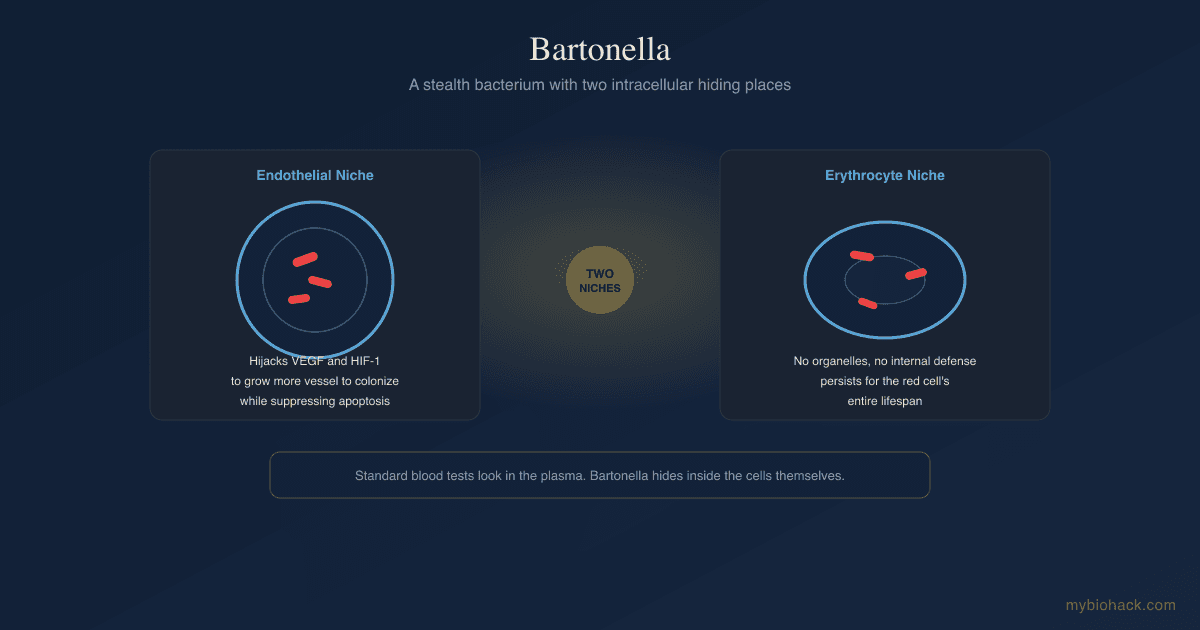
Bartonella
Babesia and Bartonella frequently co-occur, especially in patients with chronic, non-specific illness and extensive animal contact. R
A 2024 pilot study found Babesia odocoilei and Bartonella spp. co-infections in six of seven patients with chronic illness. R
This suggests that the two pathogens share transmission vectors and that testing for one should prompt testing for the other.

ME/CFS And Long COVID
Babesia infection has been linked to ME/CFS presentations. R
A study of 50 ME/CFS patients found Babesia, Bartonella, or both in 23 of 50 participants via qPCR. R
The symptom overlap is substantial: post-exertional malaise, brain fog, unrefreshing sleep, orthostatic intolerance, and immune dysfunction are common to both conditions.
From the JD perspective, both conditions share TCLS, MSS, and glycocalyx degradation as downstream mechanisms.
The hemolytic oxidative stress from Babesia feeds directly into this cascade.
For more on these mechanisms, see our posts on Long COVID natural treatment and body buzzing and internal tremors.
Mast Cell Activation Syndrome (MCAS)
Babesia-driven hemolysis releases free heme, which activates mast cells via TLR4 and the alternative complement pathway. R
Hypoxia from anemia also triggers mast cell degranulation as mast cells attempt to re-oxygenate tissues with histamine.
This bidirectional relationship means that treating Babesia can improve MCAS symptoms and vice versa.
See our post on mast cells, substance P, and neurogenic inflammation for more detail.
Iron Overload And Hemolysis
Babesia-induced hemolysis releases free iron and heme, which can create a functional iron overload state even when ferritin looks normal. R
This free iron drives Fenton chemistry, generating hydroxyl radicals that damage the glycocalyx, mitochondria, and cellular membranes.
In patients with HFE mutations (hereditary hemochromatosis), this effect is amplified.
See our post on iron overload, ferritin, and HFE hemochromatosis for more.
Biofilms
Babesia does not form biofilms itself (it is an intracellular parasite, not a bacterium), but it thrives in the same MSS environment where bacterial biofilms flourish. R
The immune dysfunction and oxidative stress from Babesia infection create conditions that allow bacterial biofilms to persist and resist treatment.
For more on this topic, see our post on biofilms and quorum sensing inhibition.
Treatment Approaches
Treatment of babesiosis depends on severity, immune status, co-infections, and whether the presentation is acute or chronic.
Pharmaceutical First-Line Therapy
The standard of care for mild-to-moderate babesiosis is a combination of Atovaquone (750 mg twice daily) plus Azithromycin (500 to 600 mg on day 1, then 250 to 600 mg daily), taken for 7 to 10 days minimum. R
This combination was shown to be as effective as the older regimen of clindamycin plus quinine but with significantly fewer side effects. R
Severe Disease
For severe babesiosis (high parasitemia over 5%, significant hemolysis, organ compromise), the recommended regimen is Clindamycin (600 mg every 6 hours) plus Quinine (650 mg every 8 hours), typically given intravenously. R
Exchange transfusion is a potentially life-saving intervention for patients with high parasitemia, severe anemia, or renal/pulmonary compromise. R
Persistent And Relapsing Infection
Immunocompromised patients often require prolonged treatment (weeks to months) and may need multiple drug combinations. R
Atovaquone-Proguanil (Malarone) has been used successfully as salvage therapy in relapsing cases. R
Tafenoquine, an 8-aminoquinoline antimalarial, has shown promise for resistant babesiosis, especially in combination with atovaquone. R
Combination therapies for resistant cases may include atovaquone plus azithromycin plus clindamycin, or atovaquone plus proguanil. R
Botanical And Herbal Therapies
Several botanical medicines have demonstrated in vitro activity against Babesia duncani, with IC50 values comparable to or better than standard pharmaceuticals. R
Cryptolepis sanguinolenta (cryptolepis): The 90% ethanol extract showed potent activity against B. duncani with no regrowth after 6 days of subculture at 2x, 4x, and 8x IC50. R
Its active alkaloid cryptolepine had an IC50 of 3.4 uM, which is lower than quinine (10 uM) and clindamycin (37 uM). R
Artemisia annua (sweet wormwood / artemisinin): Artemisinin and its derivatives artesunate (IC50 7.4 uM) and artemether (IC50 7.8 uM) showed good activity against B. duncani. R
Note that Babesia is less sensitive to artemisinin than Plasmodium is, likely because Babesia does not produce hemozoin (the haem polymer that artemisinin targets in malaria). R
Scutellaria baicalensis (Chinese skullcap): The 90% ethanol extract showed 84% inhibition against B. duncani, and its active compound baicalein had an IC50 of 12 uM. R
Polygonum cuspidatum (Japanese knotweed): Showed inhibitory activity against B. duncani in the same Johns Hopkins screening study. R
Sida acuta: This herb, traditionally used for malaria, is included in many herbal Babesia protocols such as the CSA tincture (Cryptolepis, Sida acuta, Alchornea cordifolia). R
Clinical protocols often combine cryptolepis with Sida acuta and Alchornea when cryptolepis alone is insufficient.
Clinical Protocol Integration
In the functional medicine and LLMD (Lyme-literate medical doctor) community, treatment is often layered:
An initial course of atovaquone plus azithromycin for 4 to 6 weeks is followed by or combined with herbal antimicrobials for sustained clearance.
Cryptolepis is considered the most reliable herbal Babesia agent, effective in approximately 75% of clinical cases according to experienced practitioners.
Artemisinin is typically pulsed (3 days on, 11 days off) to reduce the development of resistance, since the liver upregulates clearance enzymes after a few days of continuous use.
Supportive therapies include Low Dose Naltrexone (LDN) for immune modulation, iron management to reduce oxidative burden, and glycocalyx support during the kill phase.
Biofilm disruption with enzymes and herbal agents is often necessary since Babesia persists in the same MSS terrain where biofilms protect co-infecting bacteria.
JD-Focused Support During Treatment
During Babesia treatment, the hemolytic release of RBC debris and free heme amplifies the MSS cascade.
Supporting the glycocalyx during and after treatment is critical to prevent the TCLS worsening that often accompanies aggressive antiparasitic therapy.
Glycocalyx support strategies include HMW and LMW sulfated polysaccharides (fucoidans, chondroitin sulfate), antioxidants that quench free heme and peroxynitrite, and BH4 support to prevent eNOS uncoupling.
See the JD chapter on improving the glycocalyx for the full protocol.
What To Stay Away From
Monotherapy with atovaquone: Atovaquone used alone rapidly selects for cytochrome b resistance mutations (M134I, Y272C) in Babesia. R
Short treatment courses: The standard 7 to 10 day course is often insufficient for chronic or immunocompromised patients.
Relapse is common without extended therapy. R
Exclusive reliance on artemisinin: Artemisinin alone has limited efficacy against Babesia compared to Plasmodium because Babesia does not produce hemozoin. R
Blind iron supplementation: Hemolytic anemia from Babesia is not iron-deficiency anemia.
Iron supplementation feeds the parasite and amplifies Fenton chemistry oxidative stress.
Test iron status before supplementing.
L-arginine or NO boosters during active infection: The elevated oxidative state from Babesia hemolysis means NO will react with superoxide to form peroxynitrite (ONOO-), which damages the glycocalyx.
Testing
Blood Smear Microscopy
Giemsa-stained thin blood smear: This is the traditional gold standard for diagnosing acute babesiosis.
Babesia appears as intraerythrocytic ring forms that resemble Plasmodium, but without hemozoin pigment.
The classic tetrad formation (Maltese cross) is pathognomonic but rare. R
Limitations: Sensitivity is poor when parasitemia is low (under 1%), which is common in chronic cases.
Expertise is required to distinguish Babesia from malaria. R
PCR Testing
Polymerase chain reaction (PCR) is the most sensitive and specific method for detecting Babesia DNA in blood.
PCR can detect parasitemia at levels far below what microscopy can see. R
Quantitative PCR (qPCR) has shown 96.2% sensitivity relative to FISH and microscopy combined. R
I use the Tickborne Diseases 2.0 panel from Vibrant Wellness to assess for Babesia and other tick-borne pathogens.
This panel uses qPCR and serology to detect Babesia microti, Babesia duncani, and other species.
For a broader infectious assessment, I also use the Viral Infections Panel to evaluate concurrent viral reactivation that often accompanies tick-borne illness.
FISH Testing
Fluorescent In Situ Hybridization (FISH) detects Babesia ribosomal RNA in intact red blood cells, indicating viable, active infection.
FISH has good correlation with PCR (96% concordance). R
FISH is offered by specialty labs like IGeneX and can detect active infection even when serology is negative.
Serology (Antibody Testing)
Indirect Fluorescent Antibody (IFA) testing detects IgM and IgG antibodies to Babesia.
IgM titers rise in the first 2 to 4 weeks and decline over 6 to 12 months.
IgG titers below 160 may indicate a resolving infection. R
ImmunoBlot testing improves specificity by detecting antibodies against multiple Babesia antigens, reducing cross-reactivity issues. R
Serology alone cannot distinguish active from past infection.
Antibodies can persist for months after clearance.
Positive serology should be confirmed with PCR or FISH.
Comprehensive Tick-Borne Panels
I use the Tickborne Diseases 1.0 panel for initial screening and the more comprehensive Tickborne Diseases 2.0 for patients with high clinical suspicion or prior negative testing.
These panels include PCR, serology, and species typing for Babesia microti, Babesia duncani, and cross-reactive detection of other Babesia species.
Supportive Lab Markers
Complete Blood Count (CBC): Look for anemia (low hemoglobin and hematocrit), thrombocytopenia (low platelets), and elevated reticulocyte count (indicating bone marrow compensation for hemolysis).
LDH: Elevated lactate dehydrogenase is a marker of hemolysis and cell turnover.
Haptoglobin: Low or undetectable haptoglobin indicates intravascular hemolysis.
Bilirubin: Elevated indirect (unconjugated) bilirubin from RBC breakdown.
Ferritin: May be elevated in chronic hemolysis due to iron redistribution, not iron overload.
These markers are included in the Foundation Zoomer panel (CBC, CMP, liver function) and the Cellular Zoomer (oxidative stress markers).
For assessing the oxidative burden from chronic hemolysis and its impact on detox capacity, I use the Toxin Zoomer panel.
Mechanisms Of Action
Simple:
Babesia invades red blood cells, feeds on hemoglobin, and replicates until the cell bursts, releasing more parasites and free heme into circulation.
This triggers fever, chills, and inflammation as the immune system tries to clear the infected cells.
The ongoing destruction of red blood cells causes anemia, which starves tissues of oxygen, producing air hunger, fatigue, and tachycardia.
The free heme and iron from lysed cells generate oxidative stress that damages blood vessels and impairs immune function.
Advanced:
- Atovaquone Mechanism: Atovaquone is a specific inhibitor of the cytochrome bc1 complex (Complex III) in the mitochondrial electron transport chain of Babesia. It binds to the Qo site of cytochrome b, blocking electron transfer from ubiquinol to cytochrome c1, collapsing the mitochondrial membrane potential, and halting ATP synthesis. This selective toxicity exploits the difference between parasite and mammalian mitochondrial electron transport. R
- Azithromycin Synergy: Azithromycin binds to the 50S ribosomal subunit (specifically the L4 ribosomal protein, RPL4) of the Babesia apicoplast, inhibiting protein translation. This creates a two-hit strategy: atovaquone starves the parasite of energy while azithromycin blocks its ability to synthesize essential proteins. Resistance mutations in RPL4 (R86H, R86C, S73L) reduce azithromycin binding affinity. R
- Clindamycin And Quinine: Clindamycin also targets the apicoplast ribosome (50S subunit) by blocking peptide bond formation. Quinine interferes with heme metabolism in the parasite's digestive vacuole, though Babesia lacks the hemozoin formation pathway that makes quinine so effective against Plasmodium. This explains why clindamycin plus quinine is less well tolerated but still effective, especially in severe cases. R
- Artemisinin Activation: Artemisinin is activated by iron-dependent cleavage of its endoperoxide bridge, generating free radicals that alkylate parasite proteins. Babesia's lower sensitivity to artemisinin (compared to Plasmodium) is attributed to the absence of hemozoin formation. Babesia handles free heme differently than Plasmodium, resulting in less iron-dependent artemisinin activation. R
- Cryptolepine Intercalation: Cryptolepine, the active alkaloid in Cryptolepis sanguinolenta, intercalates with DNA and inhibits topoisomerase II, blocking parasite replication. It also modulates the immune response through NF-kB inhibition, reducing the inflammatory cytokine storm that accompanies Babesia die-off. R
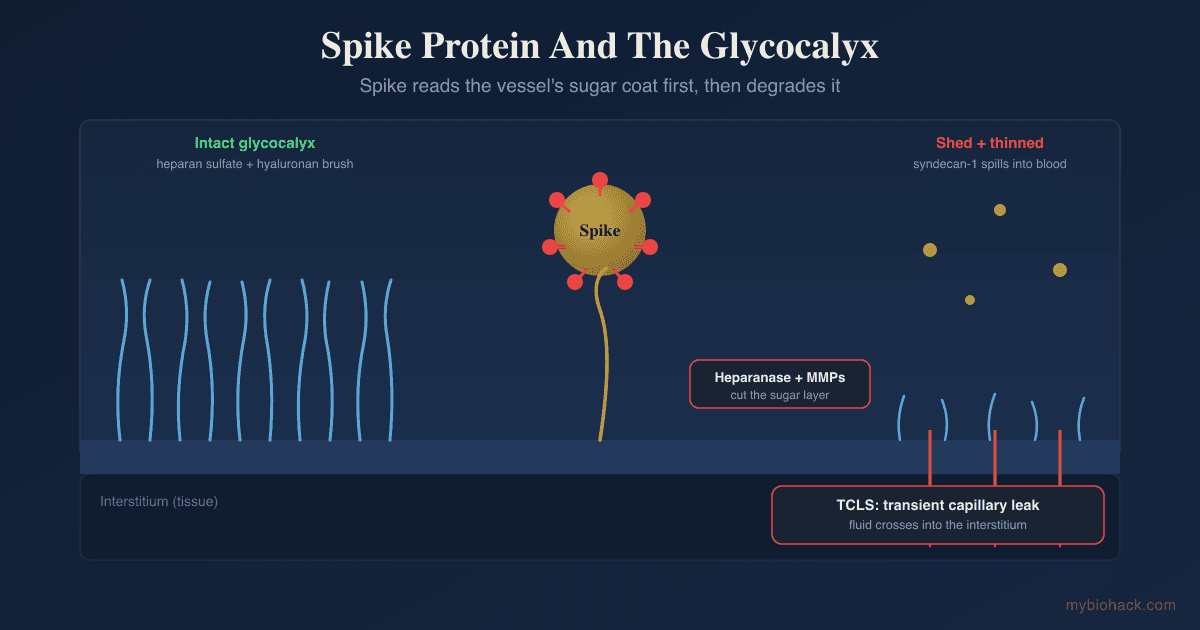
- Hemolysis And The MSS Cascade: Babesia rupture releases free heme, hemoglobin, and RBC membrane debris into circulation. Free heme activates TLR4 on macrophages and endothelial cells, triggering NF-kB translocation and proinflammatory cytokine release (TNF-a, IL-1b, IL-6). Heme also activates the NLRP3 inflammasome via ROS production, amplifying the MSS cascade. The combination of TLR4 activation, inflammasome activation, and oxidative stress directly degrades the glycocalyx via heparanase and MMP release, worsening TCLS and creating terrain favorable to persistent infection.
- Antibody As Cleanup (Jacob's Framing): The warm autoantibodies that appear in Babesia-associated AIHA are not an autoimmune attack. They are opsonins tagging damaged RBC membrane fragments for clearance by the spleen. The positive direct antiglobulin test (Coombs test) reflects this cleanup process. In Jacob's framing, the body produces these antibodies because the spleen cannot keep up with the rate of RBC damage. Suppressing the antibodies with corticosteroids is treating the smoke, not the fire. The fire is the ongoing parasitemia and hemolysis, which must be addressed with antiparasitic therapy.
Genetics
G6PD
Glucose-6-phosphate dehydrogenase (G6PD) is the rate-limiting enzyme in the pentose phosphate pathway, which generates NADPH for antioxidant defense in red blood cells.
G6PD deficiency (X-linked, most common in African, Mediterranean, and Asian populations) increases the risk of severe hemolytic anemia during Babesia infection and also increases the risk of drug-induced hemolysis from quinine, primaquine, and tafenoquine.
G6PD testing should be performed before using any 8-aminoquinoline drugs (primaquine, tafenoquine) for Babesia treatment.
HFE
The HFE gene regulates iron absorption.
The C282Y and H63D mutations are associated with hereditary hemochromatosis (iron overload).
In Babesia infection, excess free iron from hemolysis combines with HFE-driven iron absorption to amplify Fenton chemistry and oxidative stress.
rs1800562 (C282Y): homozygous mutation causes hemochromatosis, increasing oxidative burden during Babesia-induced hemolysis
rs1799945 (H63D): milder variant, but still amplifies iron-driven oxidative stress during infection
CYTB (Babesia microti mitochondrial cytochrome b)
While not a human gene, the Babesia cytochrome b gene is clinically relevant because mutations here determine atovaquone resistance.
M134I (Methionine to Isoleucine at codon 134): reduces atovaquone binding affinity at the Qo site of cytochrome bc1 R
Y272C (Tyrosine to Cysteine at codon 272): another atovaquone resistance mutation identified in relapsing patients R
These mutations are selected by subtherapeutic atovaquone exposure, monotherapy, or short treatment courses in immunocompromised hosts.
CR1 (Complement Receptor 1)
CR1 on red blood cells binds complement-opsonized immune complexes and transports them to the spleen and liver for clearance.
Polymorphisms in CR1 affect the efficiency of RBC immune complex clearance, which may influence susceptibility to Babesia infection and the severity of hemolysis.
NRF2 (NFE2L2)
NRF2 is the master transcription factor for antioxidant response enzymes (AREs).
It controls the expression of glutathione, SOD, catalase, and HO-1.
In Babesia infection, the oxidative stress from hemolysis activates NRF2, but chronic activation can lead to NRF2 exhaustion and impaired antioxidant defense.
rs6721961: reduced NRF2 expression, associated with lower antioxidant capacity during oxidative stress
SOD2
Superoxide dismutase 2 is the mitochondrial antioxidant enzyme that converts superoxide to hydrogen peroxide.
SOD2 sits on the glycocalyx surface and is the first line of defense against oxidative damage to endothelial cells.
rs4880 (Ala16Val): the Val variant reduces SOD2 import into mitochondria, which Jacob observes is common in clients with redox imbalances.
Impaired SOD2 function amplifies the peroxynitrite damage from Babesia-induced oxidative stress.
More Research
Babesia odocoilei as an emerging human pathogen: Originally considered a deer pathogen, Babesia odocoilei has now been molecularly confirmed in humans with chronic illness, often co-infecting with Bartonella species. R
Tafenoquine plus atovaquone for radical cure: A 2024 study showed that the combination of tafenoquine and atovaquone achieved radical cure with no recrudescence in both B. microti and B. duncani mouse models, and conferred sterile immunity to subsequent challenge. R
Pulse-dosed atovaquone to prevent resistance: Animal studies with ELQ-334 (an endochin-like quinolone targeting the same Qi site of cytochrome bc1) combined with atovaquone showed that dual Qo-Qi inhibition prevents resistance emergence.
This dual-target approach may eventually translate to human therapy. R
For biomarker testing I use the Tickborne Diseases 2.0 panel to assess Babesia infection, the Cellular Zoomer to evaluate oxidative stress from hemolysis, and the Toxin Zoomer to measure environmental toxin burden that impairs immune clearance.
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Quercetin
500mg 2x/day
SPM Active (Pro-resolving Mediators)
2 softgels/day
Curcumin (Liposomal)
500mg 2x/day