Bartonella (Bartonellosis): The Overlooked Chronic Vector-Borne Infection
By Jacob Gordon, INHC, FMT-CThis article contains affiliate links. As an Amazon Associate, MyBioHack earns from qualifying purchases at no extra cost to you. We only link products we research and stand behind.
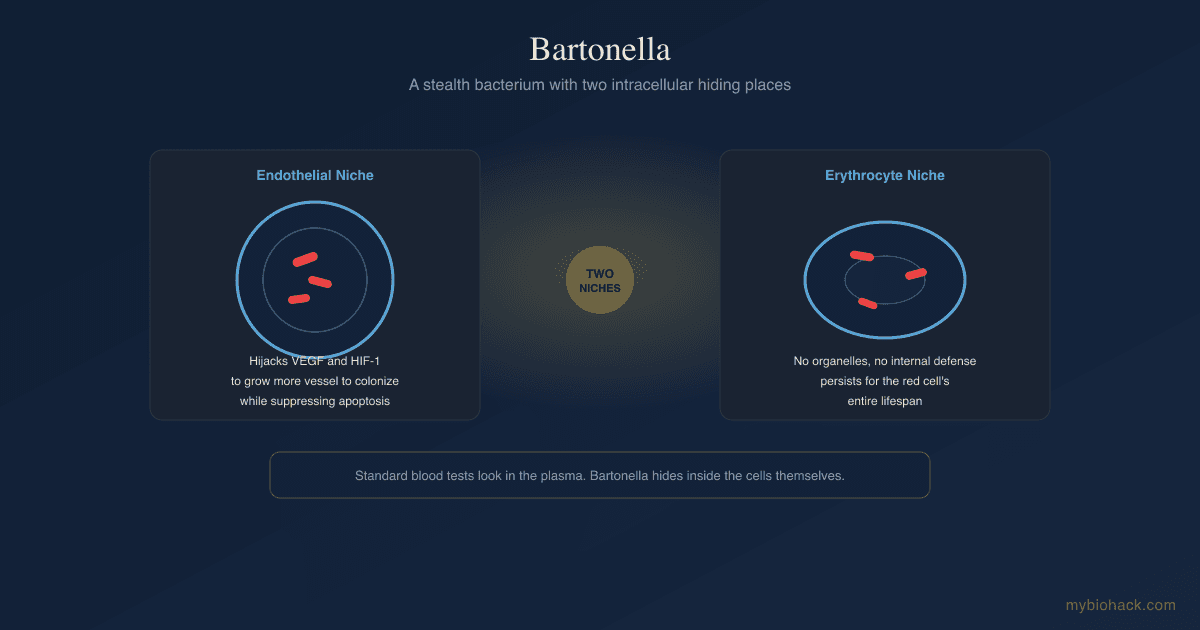
Bartonella is a stealth bacterium that lives inside your endothelial cells and red blood cells, evades standard testing, and drives vascular and neurological symptoms that get misdiagnosed as anxiety, dysautonomia, or psychiatric illness.
In this post, we will discuss what Bartonella species are, how they hide intracellularly, why they are so often missed, how they overlap with Lyme disease and other chronic conditions, their role in vascular and endothelial dysfunction, and evidence-based approaches to address them.

Basics Of Bartonella
Bartonella is a genus of fastidious, gram-negative, facultative intracellular bacteria that infect red blood cells and the cells lining your blood vessels. R
More than 45 Bartonella species have been identified, and at least 12 are linked to human disease. R
The three species most associated with human illness are Bartonella henselae, Bartonella quintana, and Bartonella bacilliformis. R
Bartonella henselae is the agent of cat scratch disease, and it also causes culture-negative endocarditis, bacillary angiomatosis, and peliosis hepatis. R
Bartonella quintana caused trench fever in soldiers during World War I, and it still causes chronic bacteremia, bacillary angiomatosis, and endocarditis, especially in people living in crowded or unsanitary conditions. R
Bartonella bacilliformis is endemic to the Andean valleys of South America, is transmitted by sandflies, and causes Carrion disease, which has an acute hemolytic phase (Oroya fever) and a chronic vasoproliferative phase (verruga peruana). R
Cat scratch disease is common: US insurance data estimate roughly 12,000 diagnoses per year, with the highest incidence in children aged 5 to 9 and in the southern states. R
What makes Bartonella clinically important is not the acute illness most doctors learn about.
It is the chronic, low-grade, relapsing form that colonizes your vasculature for months to years and produces a symptom picture that rarely gets connected back to an infection.
Bartonella has been associated with disease of the skin, liver, heart, eyes, blood, and brain. R
The classic ocular form is neuroretinitis, optic disc swelling paired with a star-shaped pattern of macular exudates, and Bartonella is one of the most common infectious causes of it. R
What Causes Bartonellosis
Bartonella is a vector-borne and animal-associated infection.
The classic route is a cat scratch or bite, because cats are the main reservoir for Bartonella henselae and can carry it in their blood for months without symptoms. R
Fleas transmit the bacteria between cats, and flea feces on the claws is thought to be a major inoculation route, since B. henselae replicates in the flea gut and is shed in viable form in flea feces for the life of the flea. R
Bartonella quintana is transmitted by the human body louse. R
The more contested route, and the one that matters most for the chronic illness community, is tick transmission alongside Lyme disease.
Vectors and exposures associated with Bartonella (not an exclusive list):
- Cat scratches and bites (primary route for B. henselae) R
- Fleas and flea feces R
- Human body lice (B. quintana) R
- Sandflies (B. bacilliformis) R
- Ticks, as a suspected co-vector with Borrelia (contested) R
The tick question is genuinely unsettled.
Bartonella DNA has been detected in ticks, and patients with chronic Lyme symptoms frequently report Bartonella co-infection, but mainstream reviews argue there is limited direct evidence that ticks are a competent vector. R
There is a big MAYBE here.
The honest position is that tick transmission of Bartonella is plausible and clinically suspected but not definitively proven, and you should not assume a tick bite is the only way to acquire it.
How Bartonella Hides In The Body
This is where Bartonella becomes fascinating and why it is so hard to catch.
It has two intracellular niches that essentially make it invisible to the immune system and to standard blood tests.
The erythrocyte niche
Bartonella is one of the few bacteria that lives inside your red blood cells. R
The bacteria adhere to the erythrocyte surface, deform the membrane, invade, and then replicate to a stable number that persists for the entire lifespan of that red blood cell. R
Adhesion to red cells is mediated by the Trw type IV secretion system, a surface apparatus that determines which host species a given Bartonella strain can infect. R
Because mature red blood cells have no organelles and cannot mount an internal defense, the bacteria sit in an immunologically privileged compartment that is ideal for transmission by a blood-feeding insect. R
This intraerythrocytic phase is also why the infection relapses so readily, since the red cell reservoir is shielded from most antibiotics. R
The endothelial niche
Bartonella's second home is the endothelium, the single-cell layer lining every blood vessel in your body.
The bacteria invade endothelial cells either as single organisms inside a Bartonella-containing vacuole that avoids fusion with lysosomes, or as large aggregates engulfed through a structure called the invasome. R
Once inside, Bartonella actively suppresses endothelial cell apoptosis, keeping its host cell alive so it has a place to live. R
It then does something almost no other bacterium does.
It hijacks the vascular growth machinery to make more endothelium to colonize.
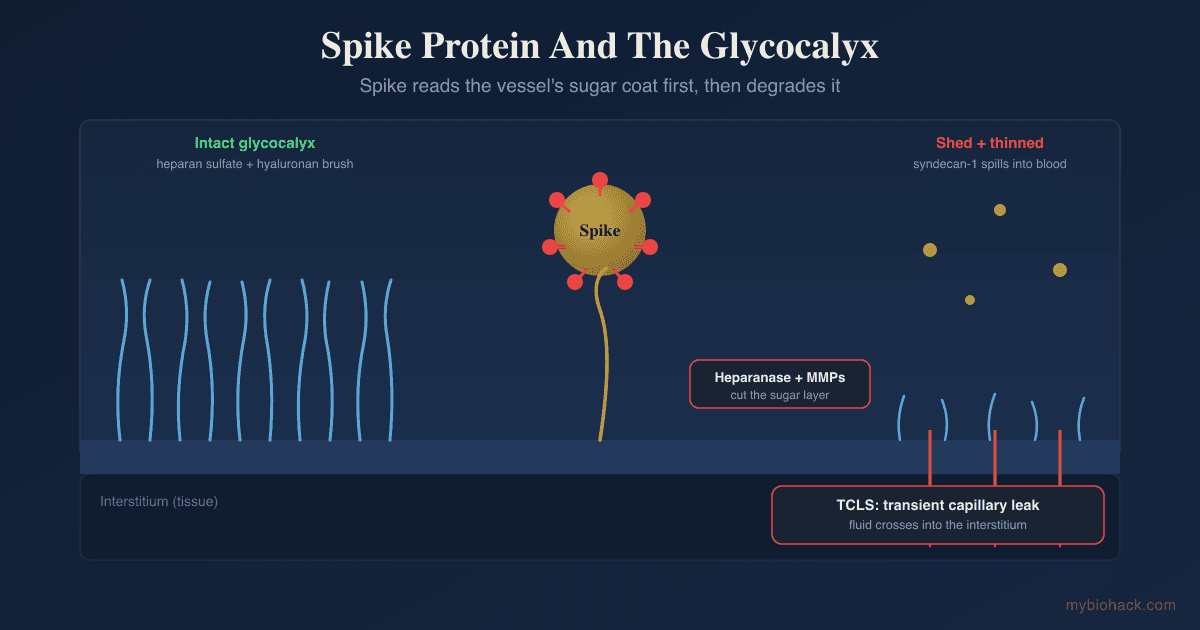
Bartonella activates hypoxia-inducible factor-1 (HIF-1) inside infected cells, which drives expression of vascular endothelial growth factor (VEGF) and produces the vasoproliferative lesions seen in bacillary angiomatosis. R
A bacterial autotransporter protein called BafA directly engages VEGF receptor-2 to switch on angiogenesis. R
The adhesin Bartonella adhesin A (BadA) mediates strong attachment and also triggers a pro-angiogenic host response. R
This VEGF and HIF-1 exploitation is worth sitting with, because these are the same adaptive pathways the body uses to rebuild vasculature after injury.
As I discuss in VEGF: Why You Should Not Reflexively Try To Lower It, VEGF is not a villain, and Bartonella is essentially borrowing a healing signal for its own survival.

The immune evasion trick
Here is the counterintuitive part that reframes how Bartonella fits into chronic illness.
Most gram-negative bacteria drive inflammation through their lipopolysaccharide (LPS), which activates Toll-like receptor 4 (TLR4) and floods the system with inflammatory cytokines.
Bartonella does the opposite.
Its LPS has very low endotoxicity and is poorly recognized by TLR4. R
The LPS of Bartonella quintana actually acts as a potent TLR4 antagonist, meaning it can blunt the inflammatory signal rather than trigger it. R
This is a masterclass in stealth, since the bacterium avoids the alarm system entirely and establishes persistent infection under the radar. R
Bartonella also builds biofilms, which further shields it from antibiotics and immune clearance. R
The Junction Dysfunction connection
Bartonella is a near-perfect example of the vascular pathology at the center of my Junction Dysfunction framework.
Junction Dysfunction is my hypothesis that a huge range of chronic conditions share a common root: damage to the glycocalyx, the sulfated sugar coating on the endothelium, which then drives capillary leak and a chronic sub-lethal immune state I call Micro-Sepsis (MSS).
Bartonella lives exactly where that damage happens, inside the endothelium and the red blood cells, and it directly manipulates vascular remodeling.
There is an interesting nuance, and I want to flag it as my hypothesis rather than settled science.
Because Bartonella evades TLR4 instead of activating it, it may not drive the classic endotoxin-based Micro-Sepsis picture the way ordinary gut-derived LPS does.
Instead, my working model is that Bartonella contributes to Junction Dysfunction through the other door: direct endothelial colonization, VEGF and HIF-1 hijacking, biofilm persistence, and red cell parasitism that alters flow and immune surveillance.
The deeper glycocalyx and capillary-leak mechanics are covered in the JD guide, including The Endothelial Glycocalyx and Microcapillaries And Vascular POTS.
I also lean toward the terrain view that many of these stealth organisms, Bartonella included, are pleomorphic and express their most pathogenic behavior in a toxic internal environment, which is why removing the terrain matters as much as killing the organism.
Bartonella And Overlapping Conditions
Bartonella rarely travels alone, and its symptoms overlap heavily with the conditions this site covers.
Chronic Lyme and tick-borne co-infection
Among patients with chronic Lyme symptoms, co-infections are extremely common, and Bartonella is one of the most frequently reported. R
Like Borrelia and Babesia, Bartonella can shift into slow-growing and biofilm-embedded forms that resist standard antibiotic courses. R
This is why single-agent, short-duration antibiotic treatment so often fails and the infection relapses. R
Dysautonomia and POTS
Because Bartonella colonizes the microvasculature and manipulates VEGF-driven vascular remodeling, it belongs in the differential for unexplained dysautonomia.
In my framework I rename vasoadaptive POTS as Vaso-Adaptive Disorder (VAD), and any organism that damages or remodels the microcapillary bed can plausibly contribute to it.
The mechanistic detail is in Microcapillaries And Vascular POTS and my post on POTS.
Neuropsychiatric illness
This is the overlap that surprises people most.
A well-documented case reported a 14-year-old who developed sudden psychotic behavior diagnosed as schizophrenia, remained ill for 18 months through multiple hospitalizations, and then improved substantially once Bartonella henselae was identified in his blood and treated with antimicrobials. R
Bartonella bloodstream infection has been proposed as a contributor to pediatric acute-onset neuropsychiatric syndrome in a subset of patients. R
A crowd-sourced investigation found an association between Bartonella-associated skin lesions and neuropsychiatric symptoms. R
Neurobartonellosis is increasingly recognized as an under-appreciated cause of neurological and psychiatric presentations. R
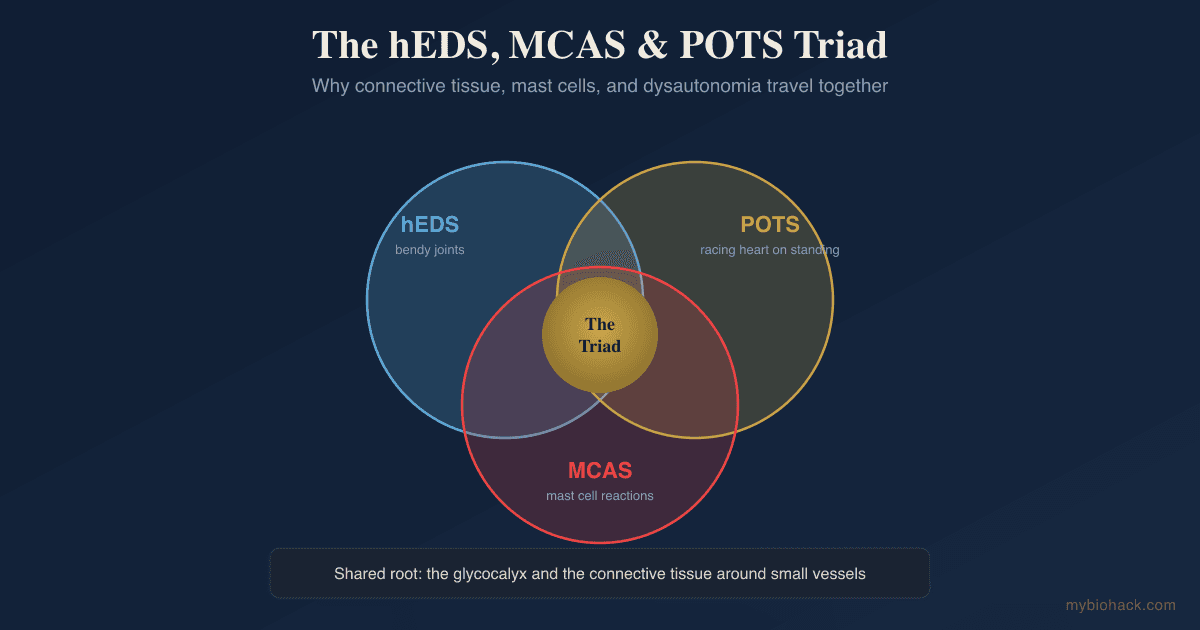
CIRS, mold, and mast cell overlap
Bartonella symptoms overlap so heavily with CIRS and mold illness that it is easy to attribute everything to one cause when several are present.
The same is true for histamine intolerance and mast cell activation, since a chronic vascular infection is a legitimate mast cell trigger.
The practical lesson is to think in terms of total load rather than a single culprit, which is why I test broadly and address bioaccumulation and terrain rather than chasing one organism.
Endocarditis
Bartonella is a leading cause of blood-culture-negative endocarditis, and it is often diagnosed late because it does not grow on standard cultures, which raises mortality. R
Anyone with unexplained heart murmur, embolic events, or persistent inflammatory illness deserves to have Bartonella considered.
How To Address Bartonella
I want to be clear up front that chronic Bartonella is a serious infection, and the antibiotic questions (which drug, how long, which combination) belong with an experienced physician.
What follows is the terrain-first, evidence-informed foundation I focus on, not a replacement for medical care.
The conventional antibiotic backbone for serious Bartonella infection is doxycycline combined with a rifamycin, often for six weeks or more, because monotherapy relapses. R
If you need personalized guidance, this is exactly the kind of complex, multi-system case I work through on a consultation.
1. Antimicrobial botanicals with real in vitro data
Several herbs have been tested directly against Bartonella henselae in the laboratory, including its hard-to-kill stationary phase.
A 2021 screen identified five botanicals with strong activity against stationary-phase Bartonella henselae. R
The same herbs also show activity against the persister forms of Borrelia burgdorferi, which is why they are used across tick-borne co-infections. R
The most active botanicals from that work, in alphabetical order:
- Chinese Skullcap (Scutellaria baicalensis) R
- Cryptolepis sanguinolenta (one of the most potent against stationary phase) R
- Black Walnut (Juglans nigra) R
- Barbed Skullcap (Scutellaria barbata) R
- Japanese Knotweed (Polygonum cuspidatum) R
One important caveat on Japanese Knotweed.
It is a major source of resveratrol, and in the Junction Dysfunction context I am cautious with resveratrol because it can enhance IDO activity, which shunts tryptophan down the kynurenine pathway and may worsen neuroinflammation in an already-inflamed nervous system. R
If you have significant neurological symptoms, weigh that trade-off rather than dosing knotweed reflexively.
2. Biofilm disruption
Because Bartonella persists in biofilms, biofilm disruption makes the antimicrobial phase more effective. R
I go deep on this in Biofilms, Quorum Sensing, And EPS.
Commonly used agents, alphabetically:
- Black Cumin Seed (Nigella sativa)
- Lumbrokinase (fibrinolytic enzyme that helps break biofilm matrix)
- N-Acetyl Cysteine (NAC, disrupts biofilm and supports glutathione) R
3. Support the endothelium and glycocalyx
Since Bartonella is fundamentally a vascular infection, protecting the endothelial lining is not optional.
The full logic is in The Endothelial Glycocalyx and Improving The Glycocalyx.
Foundational vascular support:
- Berberine (antimicrobial and endothelial support)
- Fucoidan (sulfated polysaccharide for glycocalyx repair)
- Pycnogenol (pine bark, ROS and RNS scavenger with endothelial benefit)
4. Modulate the immune system
Bartonella survives by evading and dysregulating immune signaling, so immune modulation is more useful than blunt immune suppression.
Low-Dose Naltrexone (LDN) is worth discussing with your doctor as an immune modulator in chronic infection, covered in my dedicated post.
Broader immune balancing tools are in NRF2, CIRS, And Sensitivities.
5. Address the terrain and the nervous system
Killing the organism without fixing the environment that let it thrive tends to fail.
That means addressing toxin load, gut health, and detox capacity, which I cover in bioaccumulation and biotoxin detox.
It also means limbic and nervous system work, because I rarely see people fully recover from chronic vector-borne illness on antimicrobials alone.
The cell danger response framing is useful here, because a nervous system stuck in threat mode keeps the whole healing cycle from completing.
What To Stay Away From
Do not rely on a single negative blood test to rule Bartonella out, because the standard assays miss it constantly (covered in Testing below). R
Do not expect short antibiotic monotherapy to clear it, since the erythrocyte and biofilm reservoirs drive relapse. R
Avoid aggressive die-off protocols without drainage and terrain support in place, because killing large amounts of any stealth organism at once can produce a rough Herxheimer reaction.
Be cautious with high-dose L-arginine and blind nitric oxide boosters in the setting of chronic vascular infection, because in a compromised endothelium nitric oxide can be pushed toward peroxynitrite, and arginine can reactivate latent herpesviruses you may also be carrying, since herpes simplex depends on arginine for replication and lysine antagonizes it. R
Do not ignore new cardiac or neurological symptoms, since Bartonella endocarditis and neurobartonellosis are real and require medical evaluation. R
Testing
Testing for Bartonella is genuinely difficult, and understanding why protects you from a false all-clear.
The organism causes intermittent bacteremia, seroconversion can take up to three months, commercial antibody assays have poor sensitivity, and standard PCR frequently misses low-level infection. R
In one documented case, a patient did not reach a diagnostic antibody titer until day 90 after inoculation, so serology would have read negative for three months of active infection. R
Negative serology does not rule out Bartonella, and combining methods improves detection. R

Blood And Urine Markers
Bartonella IFA antibody titers (IgG and IgM) are the common first-line serology, but low sensitivity means a negative result is not reassuring on its own. R
Bartonella PCR detects bacterial DNA and is more useful in immunocompromised patients where antibodies may be falsely negative, though a single draw can still miss intermittent bacteremia. R
Specialty tick-borne labs offer enrichment culture and droplet-digital PCR aimed specifically at improving Bartonella detection, which is worth pursuing when suspicion is high and standard tests are negative.
Functional Lab Panels
I use the Viral And Vector-Borne Infections Panel (Vibrant Wellness) to assess immune reactivity to stealth pathogens including tick-borne organisms.
I use the Gut Zoomer (Vibrant Wellness) to evaluate the gut terrain, dysbiosis, and permeability that let opportunistic infections take hold.
I use the Toxin Zoomer (Vibrant Wellness) to quantify the mycotoxin and environmental chemical load that degrades immune competence and keeps stealth infections active.
For a broad inflammatory and organ baseline, I use the Foundation Panel (Vibrant Wellness) to check CBC, metabolic markers, and immune signals.
Because Bartonella overlaps so heavily with other tick-borne illness, the Mold Illness bundle and a comprehensive workup often make more sense than testing a single organism in isolation.
Provocation And Clinical Correlation
Bartonella-associated skin striae (the reddish or purplish streaks that resemble stretch marks) can be a visible clue and have been correlated with neuropsychiatric symptoms in patient cohorts. R
Given the testing limitations, diagnosis is often a clinical judgment that weighs exposure history, symptom pattern, and multiple test modalities together, which is where working with an experienced practitioner matters.
Mechanisms Of Action
Simple:
- Bartonella hides inside your red blood cells and blood vessel walls, where your immune system and most blood tests cannot see it.
- Instead of setting off inflammatory alarms like most bacteria, it quiets them, so it can live in you for years without being noticed.
- It tricks your body into growing new blood vessels for it to colonize, using the same growth signals your body uses for healing.
Advanced:
- Intraerythrocytic persistence. Bartonella adheres to erythrocytes via the Trw type IV secretion system, deforms and invades the membrane, and replicates to a stable intracellular load that lasts the lifespan of the red cell, creating an immune-privileged reservoir and the basis for relapsing bacteremia. R R
- Endothelial invasion and anti-apoptosis. The bacterium enters endothelial cells within a non-acidified Bartonella-containing vacuole or via the aggregate invasome, then inhibits endothelial apoptosis to preserve its host cell niche. R R
- VEGF and HIF-1 hijacking. Bartonella stabilizes HIF-1 and upregulates VEGF, and the autotransporter BafA engages VEGFR-2 while the adhesin BadA drives a pro-angiogenic response, producing the vasoproliferative lesions of bacillary angiomatosis. R R
- TLR4 evasion and antagonism. Bartonella LPS has very low endotoxicity and is poorly recognized by TLR4, and B. quintana LPS acts as an active TLR4 antagonist, allowing the organism to avoid the innate inflammatory response that would normally clear it. R R
- Biofilm persistence. Bartonella forms biofilms whose extracellular matrix limits antibiotic penetration and supports tolerant persister subpopulations, contributing to treatment failure and relapse. R
Genetics
Human genetic susceptibility to Bartonella is not as well characterized as it is for many other infections, and the single strongest determinant of disease severity is overall immune competence rather than any one variant. R
People with impaired cellular immunity progress to systemic and vasoproliferative disease far more often than immunocompetent people. R
That said, the innate receptors that recognize Bartonella are a reasonable place to look.
TLR2
Toll-like receptor 2 encodes a pattern-recognition receptor on immune cells.
Bartonella is recognized primarily through TLR2 rather than TLR4, so TLR2 signaling is central to the early host response. R
Variants that reduce TLR2 function could plausibly blunt early recognition and favor persistence, though direct human data specific to Bartonella remain limited.
TLR4
Toll-like receptor 4 is the classic sensor for gram-negative LPS.
Bartonella LPS evades and can even antagonize TLR4, which means an already low-responding TLR4 genotype would offer little help against this particular organism. R
Comparative work in rodent reservoirs has linked polymorphisms in TLR1, TLR4, and TLR10 to Bartonella susceptibility, which supports the general relevance of innate receptor genetics even though the human picture is still being worked out. R
For readers pursuing the broader Junction Dysfunction genetic workup, the redox and detox variants I prioritize (SOD2, SUOX, CBS, and the RAGE and angiotensin-axis genes) matter here too, because they shape how well your endothelium and immune system tolerate a chronic vascular infection.
More Research
Bartonella research is moving quickly, and several threads are worth watching.
Antibiotic persistence and relapse remain the central clinical problem, driven by the intraerythrocytic reservoir and biofilm formation, and this is why combination and longer-course strategies outperform monotherapy. R
Drug-repurposing screens from the same laboratories that tested botanicals have flagged several existing agents with anti-persister activity against Bartonella, and this is an active area rather than established protocol, so I mention it as a research direction, not a recommendation. R
Neurobartonellosis is emerging from obscurity, and the association between Bartonella and neuropsychiatric presentations, while still built largely on case reports and cohort correlations, is strong enough that infection deserves a place in the differential for sudden or treatment-resistant psychiatric illness. R R
The tick-transmission question is genuinely unresolved, and I would treat confident claims in either direction with some skepticism until better vector-competence data arrive. R
For biomarker and infection testing I use the Viral And Vector-Borne Infections Panel, the Gut Zoomer, and the Toxin Zoomer to build a full-terrain picture rather than chasing one organism, because in my experience chronic Bartonella is almost never the only thing going on.
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Glutathione (Liposomal)
500mg 2x/day
Activated Charcoal
500mg away from food/meds
NAC
600mg 2x/day