Glutamate Dysregulation, Neuroinflammation, And The Glymphatic Feedback Loop
By Jacob Gordon, INHC, FMT-CThis article contains affiliate links. As an Amazon Associate, MyBioHack earns from qualifying purchases at no extra cost to you. We only link products we research and stand behind.
Anxiety, an overactive brain, OCD, and sensory sensitivities often trace back to a single upstream problem: too much glutamate in the wrong places, for too long.
In this post, we will discuss how glutamate dysregulation, neuroinflammation, and glymphatic failure lock into a self-amplifying feedback loop, and how one common antidepressant prescribing error can quietly feed all three.

Basics Of Glutamate Dysregulation
Glutamate is the brain's primary excitatory neurotransmitter, and roughly 90% of neurons use it to fire.
It is not a villain.
The problem is not glutamate itself, it is glutamate that lingers in the synapse and the extracellular space instead of being cleared on time.
When extracellular glutamate stays elevated, N-Methyl-D-Aspartate receptors (NMDA receptors) stay open too long, calcium floods the neuron, and the cell shifts from "signaling" to "stressed." R
This is the state behind a brain that will not turn off.
The symptom cluster of chronic glutamate excess includes: (not exclusive list)
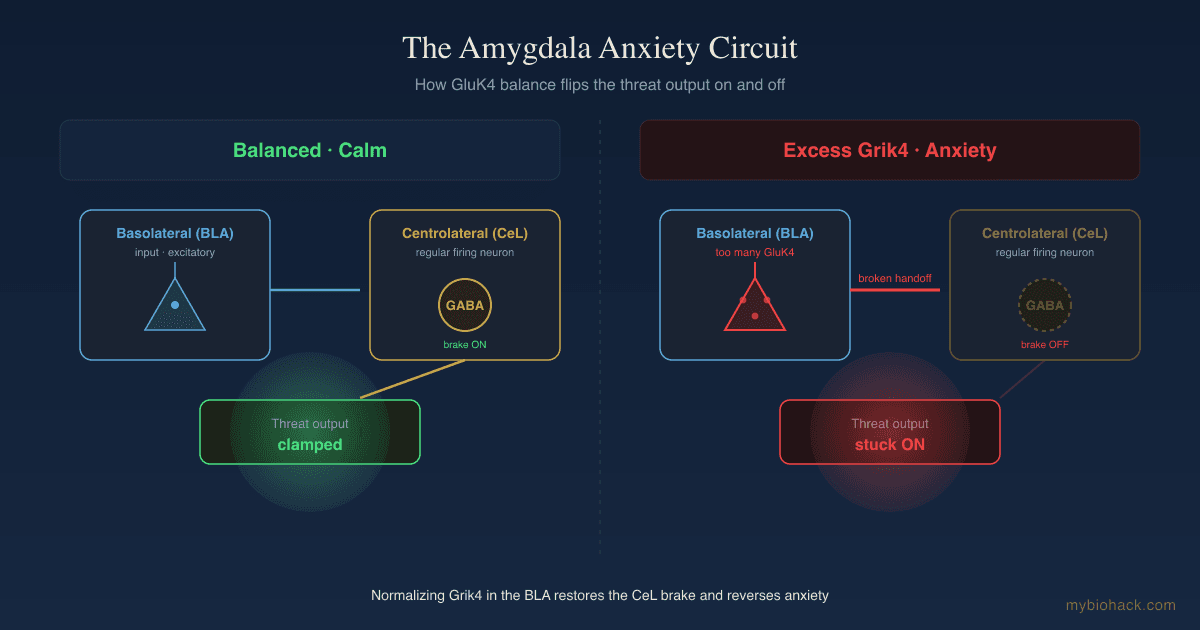
- Anxiety and inner restlessness (excess excitatory tone with insufficient GABA opposition) R
- OCD and intrusive looping thoughts (tonic-phasic glutamate dysregulation in cortico-striato-thalamo-cortical circuits) R
- Overactive, racing brain (reduced ability to gate and filter incoming signals)
- Sensory sensitivities (lowered threshold for sound, light, and touch from NMDA-driven hyperexcitability)
- Sleep-onset difficulty (an excitatory brain resists the descent into slow-wave sleep)
Unmedicated OCD patients show significantly elevated glutamate in cerebrospinal fluid compared to controls, and elevated glycine alongside it, which matters because glycine is a co-agonist at the NMDA receptor and the two together drive excess receptor activation. R R
Abnormal NMDA signaling during development is also implicated in autism spectrum conditions and ADHD, which is part of why the sensory and attentional features overlap so heavily. R
If you have read the tinnitus post, this is the same excitatory-inhibitory imbalance expressed in a different circuit.
The Glutamate And Neuroinflammation Loop
Here is where it stops being a static problem and becomes a self-feeding one.
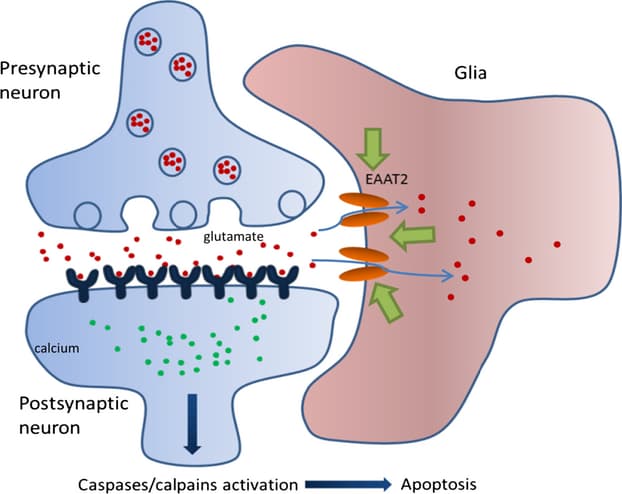
Glutamate clearance is mostly the job of astrocytes, which pull glutamate out of the synapse through transporters (chiefly EAAT2, also called GLT-1) and recycle it back into glutamine.
Neuroinflammation breaks that cleanup crew.
Inflammatory cytokines downregulate astrocytic glutamate uptake, so glutamate that should have been cleared in milliseconds instead accumulates. R
At the same time, activated microglia do something worse than fail to clean up: they actively export glutamate themselves. R
Glutamate released by activated microglia is directly excitotoxic to neurons, and blocking that microglial glutamate release is protective in injury models. R
So inflammation raises glutamate from both directions at once, less clearance and more release.
Now close the loop.
Excess glutamate and the calcium overload it causes are themselves pro-inflammatory, pushing microglia and astrocytes further into a reactive state. R
More inflammation, less glutamate clearance, more glutamate, more inflammation.
This is the engine described in the mood-disorder literature as the inflammation, glutamate, and glia trio, and it is why so many "psychiatric" symptoms behave like inflammatory ones. R
The astrocyte epigenetic memory post explains why this state can persist long after the original trigger is gone, and the tryptophan and quinolinic acid post covers a parallel inflammatory route that generates an NMDA agonist directly.
The Glymphatic System Runs On Norepinephrine
The brain has no classical lymphatic vessels inside the parenchyma, so it clears waste a different way.
The glymphatic system uses cerebrospinal fluid driven along perivascular channels to flush metabolic waste, used metabolites, and excess solutes out of the brain. R
This system is gated by norepinephrine (NE), and the gating is rhythmic, not constant.
The 2025 work from Hauglund and colleagues showed that during NREM sleep, tightly synchronized slow oscillations in norepinephrine, cerebral blood volume, and CSF are the strongest predictors of glymphatic clearance. R
Norepinephrine released from the locus coeruleus drives slow vasomotion, and that slow rhythmic squeezing of the vessels is the pump that moves CSF through the brain. R
The key word is rhythmic.
High, flat, sustained norepinephrine is the waking state, and in the waking state glymphatic clearance is largely suppressed. R
You need NE to oscillate down and up in slow waves, not to sit pinned high.
Anything that pins norepinephrine high, or flattens its slow oscillation, degrades the pump. R
For the anatomy of CSF flow, perivascular spaces, and the AQP4 water channels that make it work, see there is more to lymph than detoxing.
How Glymphatic Failure Joins The Loop
When the glymphatic pump underperforms, waste is not removed on schedule.
Among the solutes that accumulate when glymphatic clearance fails are lactate, reactive oxygen species, and glutamate itself. R
Impaired clearance also leaves inflammatory mediators sitting in the tissue, which feeds neuroinflammation, which degrades glymphatic architecture further through AQP4 mislocalization at astrocytic endfeet. R R
This is now described directly in the literature as a vicious cycle between inflammation, impaired glymphatic clearance, and neurodegeneration. R
A 2025 review goes further and argues that this clearance failure is a missing piece in psychiatric models built only on neurotransmitters, because inflammation that mislocalizes AQP4 also perturbs astrocytic glutamate handling directly. R
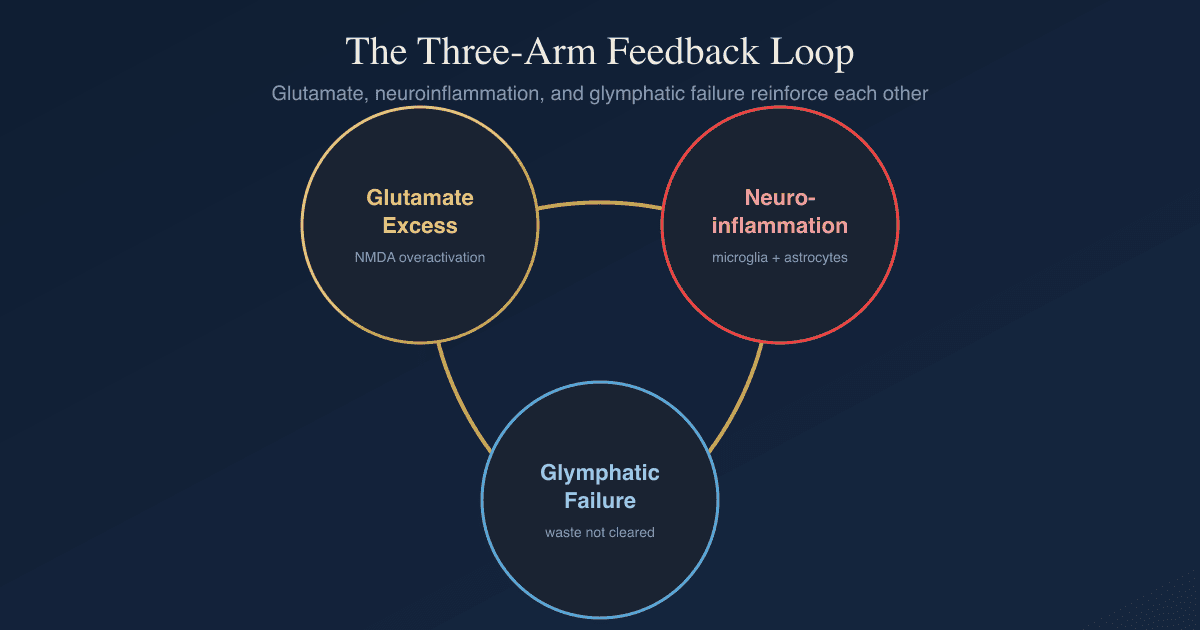
So glymphatic dysfunction is not a separate problem.
It is a third arm of the same loop: less clearance leaves more glutamate and more inflammatory debris, which drives more inflammation, which damages the clearance system, which leaves even more behind.
This is measurable in people.
Adults with ADHD show reduced glymphatic function on diffusion imaging (lower ALPS index), and the degree of dysfunction tracks with their cognitive performance. R
The brain fog, the sensory overload, and the racing mind are not three diseases.
They are three readouts of one feedback loop with three arms: glutamate, glia, and glymphatics.
A Case Study: Bupropion, CYP2D6, And The Locus Coeruleus
This is where a common prescribing pattern can quietly drive the entire loop.
Bupropion is a norepinephrine-dopamine reuptake inhibitor (NDRI), so by design it raises and sustains norepinephrine.
Two mechanisms make it relevant here, and both are underappreciated.

First, the metabolite.
Bupropion is primarily metabolized by CYP2B6 into hydroxybupropion (not by CYP3A4, which is a common misconception). R
Hydroxybupropion is the dominant active species in the body, it circulates at concentrations several-fold higher than the parent drug, and it is a more potent norepinephrine reuptake inhibitor, with the S,S enantiomer being roughly twice as potent at the norepinephrine transporter as racemic bupropion. R R
So most of the norepinephrine effect is actually coming from the metabolite, and it is strong.
A large, sustained increase in norepinephrine is exactly the signal that flattens the slow NE oscillations the glymphatic pump depends on, and over time the locus coeruleus downregulates its own signaling in response to chronic high tone. R
Pin the NE high, blunt the oscillation, and you blunt overnight glymphatic clearance.
Second, the interaction nobody checks.
Although bupropion is metabolized by CYP2B6, it is a potent inhibitor of a different enzyme, CYP2D6. R
The inhibition is strong enough that after starting bupropion, a meaningful fraction of normal CYP2D6 metabolizers test as poor metabolizers, and the effect is driven largely by the metabolites and their stereoisomers, with CYP2D6 also being downregulated, not just reversibly blocked. R R R
This means any drug, supplement, or compound that depends on CYP2D6 for clearance can stack up to unintended concentrations, even in someone with no CYP2D6 genetic variant at all.
My Biohack: When I was prescribed bupropion, before any of this research, nobody checked whether my other medications ran through a vulnerable metabolic pathway. I was already on an NDRI cleared by CYP2D6, and my own CYP2D6 status is intermediate, one working allele and one null allele. That was manageable on its own. But bupropion is a strong CYP2D6 inhibitor, so the concentration of the other NDRI climbed well past where it should have been. The result was a stack of norepinephrine signaling, from the bupropion metabolite, from the over-concentrated NDRI, and from a locus coeruleus that no longer had room to oscillate down at night. Sustained NE up top, suppressed glymphatic drainage underneath. If you are on bupropion, ask whether anything else you take is a CYP2D6 substrate before you assume your genetics protect you.
To be fair to the drug, there is a real MAYBE here.
Noradrenergic drugs are not uniformly harmful to the brain, and there is an active hypothesis that noradrenergic therapies may have broad benefit in slowing neurodegeneration, partly through anti-inflammatory effects. R
The concern in this post is specific: chronic, flat, elevated norepinephrine that erases the slow oscillation, combined with an unchecked CYP2D6 interaction that amplifies the load.
It is the pattern, not the molecule alone.
How To Calm The Loop
The loop has three arms, so the leverage points are: lower the excess glutamate, lower the neuroinflammation, and restore glymphatic clearance.
Because glymphatic restoration is its own deep topic, the full protocol for that arm lives in the companion post on improving the glymphatic system and AQP4, and this section focuses on the glutamate and inflammation arms.
1. Restore Astrocyte Glutamate Clearance
The fastest structural fix is helping astrocytes pull glutamate out of the synapse again.
N-Acetylcysteine (NAC): drives the cystine-glutamate antiporter and glutathione synthesis, and is one of the better-studied glutamate-modulating agents in OCD. R
2. Add Inhibitory Tone Without Sedation
You are trying to oppose excess excitation, not flatten the brain.
Theanine raises GABA and promotes alpha rhythms without sedation, which is why it takes the edge off an overactive brain without blunting it.
L-Theanine: the actionable supplement form, typically dosed 100 to 200 mg.
Magnesium L-Threonate: magnesium sits in the NMDA receptor channel as a voltage-dependent block, so adequate magnesium directly restrains NMDA overactivation, and the L-threonate form is the one shown to raise brain magnesium.
3. Lower The Neuroinflammation Driving The Loop
If inflammation is suppressing glutamate clearance, calming it lets the cleanup crew work again.
Omega-3 (high DHA): DHA is anti-inflammatory and also supports AQP4 polarization, so it acts on the inflammation arm and the glymphatic arm at once. R
Curcumin: broad suppression of microglial activation and NF-kB signaling.
4. Protect The Nightly Glymphatic Window
This is the arm most people miss, and it is where the bupropion problem lives.
Anything that keeps norepinephrine pinned high at night, late caffeine, late stimulants, screen-driven arousal, blocks the slow NE oscillation that powers overnight clearance. R
Melatonin supports sleep architecture and has its own glymphatic and amyloid-clearance signal in animal work.
Melatonin: start low, 0.3 to 1 mg, since the goal is rhythm, not sedation.
The deeper sleep-stage and positional levers are in the glymphatic biohacks post and my sleep experiments post.
What To Stay Away From
Compounds and habits that feed the loop: (not exclusive list)
- Alcohol (raises glutamate on the rebound and impairs glymphatic clearance)
- Chronic late-night stimulants (sustained norepinephrine flattens the oscillation that drives overnight clearance) R
- Glycine loading at night (glycine co-activates the NMDA receptor, and it is already elevated in some glutamate-excess states) R
- Monosodium glutamate sensitivity (a real subset of people react to dietary glutamate loads)
- Unchecked CYP2D6 stacking (starting a CYP2D6 inhibitor like bupropion on top of a CYP2D6 substrate without reviewing the interaction) R
Mechanisms Of Action
Simple:
- Glutamate is the brain's "go" signal, and when it is not cleared fast enough the brain cannot stop.
- Inflammation jams the cleanup crew that removes glutamate, so glutamate piles up.
- The piled-up glutamate causes more inflammation, which is the loop.
- The brain washes itself out at night using slow waves of norepinephrine, and drugs or habits that keep norepinephrine high all the time break that nightly wash.
- When the nightly wash fails, leftover glutamate and inflammatory junk stay in the brain and feed the loop again.
Advanced:
- Astrocytic EAAT2 downregulation Pro-inflammatory cytokines suppress the dominant glutamate transporter EAAT2/GLT-1, reducing synaptic and perisynaptic glutamate uptake and raising extracellular glutamate available for NMDA receptor over-activation. R R
- Microglial glutamate export Activated microglia release glutamate via the system xc- antiporter and gap-junction hemichannels at concentrations sufficient to cause excitotoxic neuronal injury, which is reversible by blocking that release. R R
- Locus coeruleus norepinephrine oscillation Phasic slow oscillations of locus coeruleus norepinephrine drive vasomotion and CSF influx during NREM sleep, and pharmacologically flattening or sustaining NE tone suppresses this clearance. R R
- AQP4 depolarization Neuroinflammation mislocalizes aquaporin-4 away from polarized astrocytic endfeet, degrading perivascular water transport and trapping solutes including glutamate and ROS in the interstitium. R R
- Bupropion metabolite pharmacology CYP2B6 converts bupropion to hydroxybupropion, the dominant circulating active species and a potent NET inhibitor, while bupropion and its stereoisomeric metabolites simultaneously inhibit and downregulate CYP2D6, amplifying co-administered CYP2D6 substrates. R R R
Genetics
CYP2D6
CYP2D6 encodes a liver enzyme that clears a large share of psychiatric drugs and many supplements.
Variants range from poor to ultrarapid metabolizers, and intermediate metabolizers carry one functional and one non-functional allele.
The clinically important point is that an inhibitor like bupropion can convert a normal metabolizer into a functional poor metabolizer regardless of genotype, so genotype alone does not tell you your real-world clearance once an inhibitor is on board. R R
CYP2B6
CYP2B6 encodes the enzyme that performs the main metabolic step on bupropion.
Reduced-function CYP2B6 variants shift the ratio of parent drug to hydroxybupropion, which changes how much norepinephrine-active metabolite you actually carry. R
SLC6A2 (NET)
SLC6A2 encodes the norepinephrine transporter, the exact target hydroxybupropion inhibits.
Reduced NET function or pharmacologic NET inhibition raises synaptic norepinephrine and sustained tone, which is the signal that blunts the slow glymphatic oscillation. R
AQP4
AQP4 encodes the water channel that makes glymphatic flow possible at astrocytic endfeet.
Variants and inflammation-driven mislocalization both reduce the polarized AQP4 distribution that clearance depends on. R
More Research
- Adults with ADHD show measurably reduced glymphatic function that correlates with cognitive performance, supporting the idea that clearance failure is part of the symptom picture, not just a consequence. R
- In mood disorders, the inflammation-glutamate-glia model predicts that anti-inflammatory and glutamate-modulating strategies should help a subset of treatment-resistant patients, which matches the NAC and ketamine literature. R R
- Sleep physiology can be deliberately targeted to modulate glymphatic clearance, meaning the nightly window is a real intervention point, not a fixed trait. R
- Reduced glymphatic function on diffusion imaging has now been documented across anxiety-adjacent and neurodevelopmental conditions including ADHD and autism, supporting a transdiagnostic clearance component rather than a single-disease finding. R R
For pharmacogenomic clearance status I use the Methylation Genetics panel alongside CYP-focused testing to understand which detox and drug-clearance pathways are running slow before stacking anything that competes for them.
For the systemic inflammatory and oxidative-stress side of the loop I use the Cellular Zoomer to assess organic acids, mitochondrial function, and oxidative markers.
If your situation involves multiple medications and a real interaction risk, this is the kind of complexity that warrants a practitioner reviewing the full stack rather than guessing, which is what a consultation is for.
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Lion's Mane
1000mg/day
Omega-3 (DHA)
2g/day
Phosphatidylserine
100mg 3x/day