HMB (Beta-Hydroxy-Beta-Methylbutyrate): Muscle Preservation, Sarcopenia, And The Free Acid Vs Calcium Debate
By Jacob Gordon, INHC, FMT-CThis article contains affiliate links. As an Amazon Associate, MyBioHack earns from qualifying purchases at no extra cost to you. We only link products we research and stand behind.
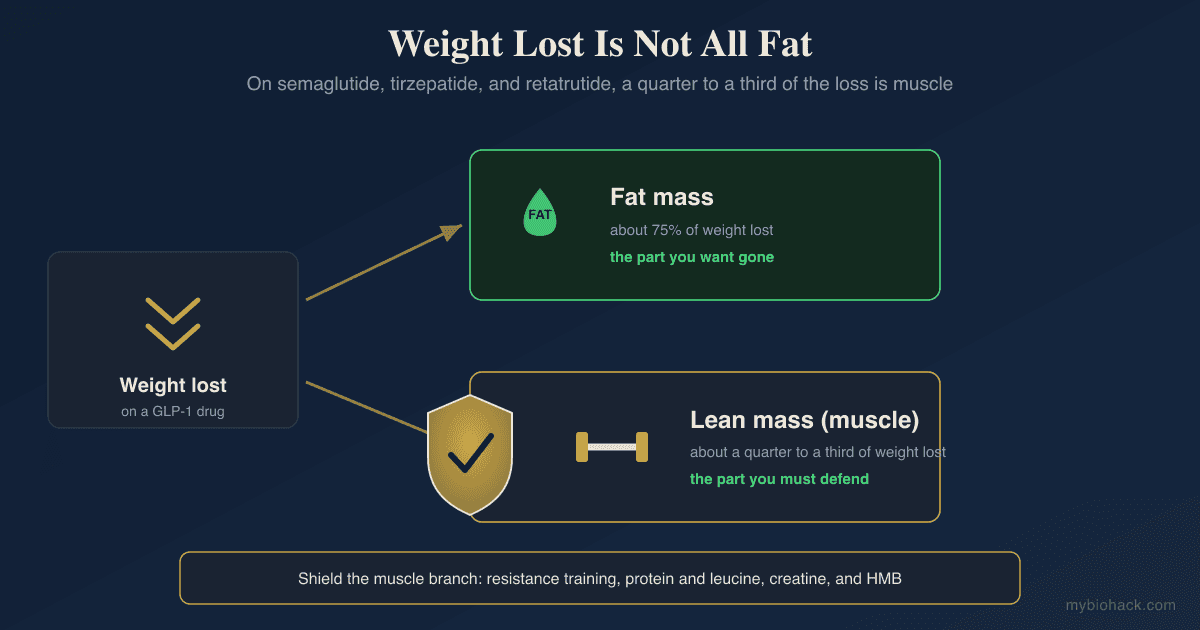
Beta-Hydroxy-Beta-Methylbutyrate (HMB) is a metabolite of the branched-chain amino acid leucine, and its usefulness depends heavily on who is taking it and in what form. It is excellent for preserving muscle during catabolic stress and modest for driving hypertrophy in already-trained athletes.
In this post, we will discuss how HMB is produced, the cellular signaling pathways it influences, the free acid versus calcium salt form debate and what the head-to-head trials actually show, who gets clinically meaningful benefit, how to dose it alongside protein and training, the natural sources, and the genetics that modify individual response.

Basics Of HMB
HMB is produced endogenously from leucine via the alpha-ketoisocaproate (KIC) intermediate through a minor branch of BCAA metabolism. R
Roughly 5 percent of ingested leucine is converted to HMB, which means a typical diet produces about 0.2 to 0.4 g of HMB per day, well below the 3 g doses used in clinical trials. R
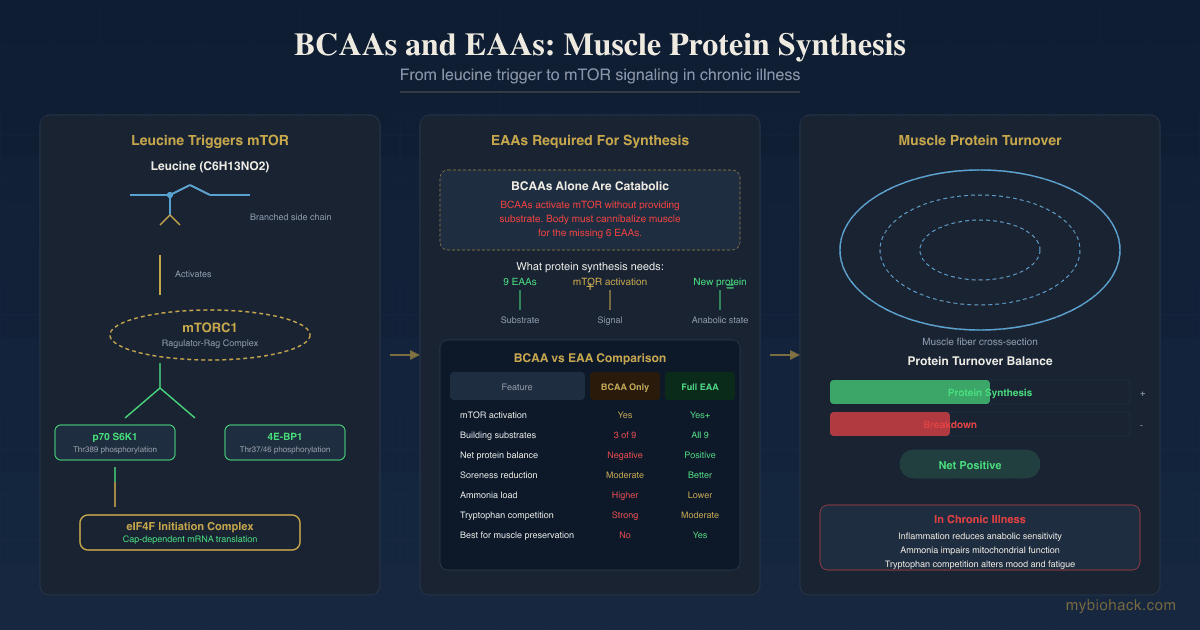
HMB has two primary effects on muscle tissue: it modestly activates mTOR-driven protein synthesis (via Rag GTPase signaling), and it more strongly inhibits the ubiquitin-proteasome-driven protein breakdown pathway.
The second effect is where most of the clinical benefit comes from and why HMB outperforms in catabolic states.
HMB was first commercially developed in the 1990s following research on leucine metabolism at Iowa State and has since accumulated over 100 randomized controlled trials across populations from elite athletes to ICU patients to nursing home residents. R
The pattern in that trial literature is consistent: large effect sizes in catabolic or untrained populations, modest and less consistent effects in well-trained athletes at protein sufficiency R.
How HMB Protects Muscle
The consistent findings across clinical trials and mechanistic studies are: (alphabetical)
- Attenuates atrogin-1 and MuRF1 (the two E3 ubiquitin ligases that tag muscle protein for proteasomal degradation, which is the dominant anti-catabolic mechanism)
- Increases satellite cell proliferation (supports repair after damage and during recovery from immobilization)
- Modestly activates mTORC1 (less powerfully than leucine itself but sufficient to support protein synthesis in combination with adequate protein intake) R
- Preserves membrane integrity via HMG-CoA precursor effects (HMB feeds a minor pool of HMG-CoA and cholesterol synthesis relevant to damaged myocyte membranes) R
- Reduces autophagy during catabolic stress (maintains muscle mass during prolonged catabolic states) R
- Reduces myostatin expression (removing a brake on muscle growth) R
- Suppresses caspase-8 and caspase-3 activation (reduces apoptotic muscle loss during bed rest, cachexia, and immobilization) R
The balance between synthesis and breakdown is the defining variable.
In a young, well-fed, training individual, synthesis is already near-maximal and breakdown is well-controlled, so HMB adds little.
In an older adult, a bed-rest patient, or a cachectic cancer patient, breakdown is dramatically elevated, and HMB's anti-catabolic action is clinically significant. R
HMB-CA Versus HMB-FA
Two forms of HMB are commercially available.
HMB calcium (HMB-CA) is the original form used in almost all early clinical studies and is cheaper to manufacture.
It peaks in plasma at roughly 60 minutes after ingestion and produces moderate bioavailability with a half-life of 2-3 hours. R
HMB free acid (HMB-FA) peaks at 30 minutes, produces higher peak plasma levels (roughly double those of HMB-CA for the same dose) R, and was developed specifically to address the pharmacokinetic limitations of the calcium form. R
The free acid form has been marketed aggressively as a meaningful upgrade, with some studies showing larger effect sizes.
There is a big MAYBE here.
Head-to-head studies in resistance-trained populations have not consistently demonstrated superior hypertrophy with HMB-FA over HMB-CA.
A well-controlled 12-week trial in resistance-trained men showed equivalent strength and hypertrophy gains from HMB-FA and HMB-CA when total daily dose was matched. R
The practical conclusion:
- For catabolic and clinical contexts where peak plasma matters and time-to-effect is important (peri-surgical, ICU, acute cachexia) R, HMB-FA may be preferable.
- For general preservation during training, caloric deficit, or sarcopenia prevention, HMB-CA is adequate and substantially cheaper.
- For peri-workout timing in resistance athletes, HMB-FA timing flexibility may offer modest convenience.
The marketing claims of 2x or greater hypertrophy with HMB-FA do not hold up in well-controlled replications. R
Who Actually Benefits
HMB shines when muscle is being actively lost and underperforms when hypertrophy is the goal in already-trained athletes at protein sufficiency.
Clear benefit groups: (alphabetical)
- Bed rest and immobilization (HMB reduces muscle loss during forced inactivity, with strong evidence for 10-28 day bed rest scenarios) R
- Burn and trauma recovery (HMB preserves lean mass during the hypercatabolic phase) R
- Cachexia (cancer, COPD, AIDS, heart failure) (improves lean mass, grip strength, and functional capacity, typically as part of multimodal nutrition) R
- Caloric deficit while training (preserves lean mass during cuts and competition prep)
- Hospitalized older adults (reduces the skeletal muscle loss of acute illness and hospitalization) R
- Post-surgical recovery (reduces protein catabolism in the immediate post-op period) R
- Sarcopenia in older adults (3 g daily improves strength, lean mass, and functional endpoints, particularly combined with vitamin D and resistance training) R
- Untrained and novice lifters (meaningful effect on early gains during initial adaptation period) R
Ambiguous or minimal benefit:
- Resistance-trained athletes targeting hypertrophy (effect is smaller and less consistent, and protein sufficiency plus training quality dominate the outcome variance) R
- Endurance athletes without catabolic stress (modest benefit on recovery markers, minimal effect on performance) R
- Body recomposition in well-trained, well-fed individuals
Dosing And Timing
The studied dose is 3 g per day, typically split into three 1 g doses taken with meals for HMB-CA.
For HMB-FA, a single 3 g dose 30-60 minutes before training is often used, though splitting works as well.
HMB-FA (Free Acid): fastest-acting form, useful in cachectic, peri-workout, and peri-surgical contexts.
HMB Calcium: cost-effective, adequate for most general sarcopenia prevention and muscle preservation during caloric deficit.
Doses above 3 g daily do not produce additional benefit in most trials.
Time to effect is 2-6 weeks for measurable strength and lean mass changes, with cumulative benefit over 12 weeks in older adults and cachexia.
Load-and-maintain approaches (6 g for the first week, then 3 g) are sometimes used peri-surgically but are not necessary for long-term supplementation.
Stack With Adequate Protein
HMB does nothing without sufficient protein substrate.
Target intake: 1.6 g/kg bodyweight for training adults, 1.2 g/kg for older adults aiming at sarcopenia prevention, 1.0-1.2 g/kg minimum during cachexia.
Protein distribution across meals (20-40 g per meal, 3-4 meals) matters more than total protein above a threshold.
Leucine content of 2.5-3 g per meal is the practical target for maximum mTOR stimulation. R
Stacking With Other Anabolic Inputs
HMB combines well with several other evidence-backed compounds.
Vitamin D3 with K2: in older adults, the combination of HMB plus vitamin D plus resistance training consistently outperforms any two alone for sarcopenia endpoints.
Creatine Monohydrate: different mechanism (phosphocreatine energy buffering) with no overlap, pairs well at 3-5 g daily. See the creatine post for full coverage.
Whey Protein Isolate: provides the leucine and total protein substrate that HMB builds on. R
Omega-3 EPA/DHA: adjunctive anti-catabolic effect in cachexia, sarcopenia, and recovery contexts via reduced muscle inflammation. R
BCAAs: marginal additional benefit if total protein is already adequate, otherwise redundant with whey.
Testosterone optimization where appropriate amplifies HMB's anti-catabolic effects in cachexia and aging. R
Resistance training is non-negotiable for getting the full benefit from HMB in any population, and HMB cannot substitute for training load.
Natural Sources
Whole-food HMB content is low, which is why supplementation is the practical route for reaching clinically studied doses.
The highest dietary sources are: (alphabetical)
- Alfalfa (the highest plant source)
- Asparagus
- Avocado
- Catfish
- Citrus fruits (small amounts)
- Grapefruit
Typical dietary intake is roughly 0.2 to 0.4 g per day from endogenous leucine conversion plus minor direct dietary HMB, which is below the 3 g supplemental target.
Reaching 3 g daily from food alone is not realistic.
Safety And Tolerance
HMB has an excellent safety profile across studied populations.
Long-term trials up to 12 months at 3 g daily have shown no consistent adverse effects on liver enzymes, kidney function, lipids, or glucose. R
Gastrointestinal tolerance is generally good at 3 g daily.
Higher doses (6+ g) have been used short-term without safety signals but without additional benefit.
HMB is not a banned substance in any major athletic governing body.
The calcium form provides roughly 200 mg calcium per 3 g dose, which is meaningful for individuals with calcium intake monitoring.
What To Stay Away From
- HMB alone without protein sufficiency (insufficient substrate for the anti-catabolic effect to matter)
- Marketing claims of 10-20 percent additional hypertrophy in trained lifters (not replicated in rigorous trials)
- Using HMB to replace resistance training (HMB is adjunct, not substitute)
- Proprietary blends with undisclosed HMB dose (many products contain sub-therapeutic doses below 1 g)
- Stacking multiple expensive proprietary formulas claiming synergy without evidence (HMB, adequate protein, vitamin D, and training do the bulk of the work)
Testing
Functional Markers
HMB benefit is best tracked functionally, not biochemically.
Useful metrics include: (alphabetical)
- DEXA lean mass tracked at 3-6 month intervals
- Gait speed in older adults (4-meter walk test)
- Grip strength via handheld dynamometer
- One-rep max progression in resistance-trained populations
- Short Physical Performance Battery (SPPB) in older adults
- Sit-to-stand test (5x or 30-second variants)
- Time-to-exhaustion in cachectic or endurance populations
Blood Markers
Creatine kinase can reflect muscle turnover during heavy training blocks.
Serum 25-OH vitamin D should be above 40 ng/mL for optimal HMB response, available via the Nutrient Zoomer (Vibrant Wellness).
IGF-1 and free testosterone to characterize anabolic tone via the Hormone Zoomer (Vibrant Wellness).
BUN, creatinine, and eGFR for kidney function baseline in older adults.
Functional Lab Panels
I use the Nutrient Zoomer (Vibrant Wellness) to assess amino acid status, vitamin D, and the minerals (zinc, magnesium, selenium) that modulate muscle protein synthesis.
The Hormone Zoomer (Vibrant Wellness) captures testosterone, DHEA, IGF-1, and cortisol rhythm relevant to overall anabolic tone.
The Cellular Zoomer (Vibrant Wellness) identifies mitochondrial limitations that would blunt HMB's anabolic signal.
Imaging
DEXA scan quantifies lean mass, fat mass, and bone density, which is the meaningful timescale for HMB endpoints (3-6 months).
Ultrasound muscle thickness (rectus femoris, vastus lateralis) is a practical office-based tracking tool.
Mid-arm muscle circumference is a low-cost bedside tool in cachexia populations.
Mechanisms Of Action
Simple:
- HMB comes from the amino acid leucine and tells muscle to hold onto itself.
- It blocks the breakdown pathways more than it boosts the building pathways.
- It works best in older adults, during illness, or when you are losing muscle, and less clearly in already-trained young lifters who are already near their ceiling.
- It does nothing without adequate protein and training.
Advanced:
- Ubiquitin-proteasome suppression. HMB downregulates atrogin-1 (FBXO32) and MuRF1 (TRIM63), the E3 ligases that tag sarcomeric proteins for proteasomal degradation. This is the dominant anti-catabolic mechanism and explains why HMB's largest effects appear in states of elevated catabolism. R
- mTORC1 activation via Rag GTPases. HMB activates mTORC1 via upstream Rag GTPase signaling, supporting 4E-BP1 phosphorylation and S6K1-driven protein synthesis, though with less amplitude than leucine itself. R
- HMG-CoA precursor role. A minor fraction of HMB feeds into HMG-CoA and cholesterol synthesis, supporting membrane repair in damaged muscle. This is particularly relevant in statin-induced myopathy contexts where HMB partially offsets the mevalonate pathway blockade. R
- Apoptosis suppression. HMB attenuates caspase-8 and caspase-3 activation in disuse and cachexia models, reducing apoptotic loss of myonuclei, which is critical because lost myonuclei are difficult to recover. R
- Myostatin downregulation. HMB reduces myostatin expression in several models, which removes a brake on muscle growth and partially overlaps with creatine's mechanism. R
- Autophagy modulation. HMB reduces excessive autophagic muscle breakdown during prolonged catabolic states without suppressing the basal autophagy required for cellular health. R
- Satellite cell activation. HMB supports satellite cell proliferation and differentiation, which is relevant for recovery from muscle damage and for maintaining myonuclear pool in older adults. R
- Reduced exercise-induced muscle damage. HMB modestly reduces creatine kinase elevation and delayed-onset muscle soreness after eccentric exercise, supporting a peri-workout protective role. R
Genetics
ACTN3
Encodes alpha-actinin-3, a fast-twitch muscle fiber protein.
rs1815739 R577X — X allele homozygotes lose ACTN3 expression and may show slightly different anti-catabolic responsiveness to HMB, though data are preliminary and the overall effect size is small.
MSTN (Myostatin)
Encodes the negative regulator of muscle growth.
Loss-of-function variants produce hypermuscular phenotypes (double-muscling) in animals and humans.
HMB has been shown to reduce myostatin expression in several models R, providing one pathway for the anti-catabolic effect.
VDR (Vitamin D Receptor)
Modulates the synergy between vitamin D status and HMB response in sarcopenia populations.
rs2228570 (FokI) variants affect receptor activity and pair with the observation that HMB works best with adequate vitamin D.
rs7975232 (ApaI) and rs731236 (TaqI) variants are associated with altered lean mass and muscle function in older adults. R
IGF1
Encodes insulin-like growth factor 1, a dominant anabolic signal.
Promoter variants affect baseline IGF-1 levels and may modify HMB responsiveness in sarcopenia contexts. R
MTHFR
rs1801133 (C677T) — affects methylation and amino acid metabolism indirectly, relevant to leucine-to-HMB conversion efficiency in some individuals. See the methylation guide.
BCAT2
Encodes branched-chain aminotransferase 2, the enzyme that converts leucine to alpha-KIC.
Variants affecting BCAT2 activity modulate the rate of endogenous HMB production from dietary leucine. R
More Research
- A double-blind trial of 3 g HMB daily in older adults preserved lean mass over 10 days of bed rest without confounders, showing the strongest clinical signal is during acute catabolism. R
- For biomarker testing I use the Nutrient Zoomer to assess the amino acid and vitamin D context that determines HMB responsiveness.
- HMB combined with vitamin D and protein produces larger effects on strength and function in sarcopenia than HMB alone, which is the clinical protocol most trials now follow. R
- HMB supplementation reduces muscle damage markers in untrained individuals starting a resistance program, supporting its use during novice training adaptation. R
- In cachexia populations (cancer, COPD), HMB as part of multimodal nutrition improves lean mass and quality of life endpoints, with larger effects when combined with omega-3 and adequate protein. R
- HMB reduces exercise-induced autophagy during prolonged catabolic exercise, preserving muscle mass in extreme training and endurance contexts. R
- Mechanistic studies show mTORC1 activation by HMB through Rag GTPase signaling, explaining the modest protein synthesis enhancement. R
- Randomized trials in resistance-trained young adults consistently show smaller effect sizes than in untrained or catabolic populations, which should calibrate expectations for already-lean athletes. R
- Recent meta-analyses confirm significant benefit in cachexia and sarcopenia populations and suggest smaller but real effects in healthy older adults. R
- The HMB-FA pharmacokinetic advantage over HMB-CA does not consistently translate to superior hypertrophy or strength outcomes in head-to-head trials. R
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Quercetin
500mg 2x/day
Vitamin D3 + K2
5000 IU + 200mcg/day
Magnesium Glycinate
400mg at bedtime