BCAAs And EAAs For Muscle Health In Chronic Illness
By Jacob Gordon, INHC, FMT-CThis article contains affiliate links. As an Amazon Associate, MyBioHack earns from qualifying purchases at no extra cost to you. We only link products we research and stand behind.
Muscle loss accelerates during chronic illness from a combination of inactivity, systemic inflammation, mitochondrial dysfunction, and anabolic resistance that conventional protein recommendations do not account for.
In this post, we will discuss what branched-chain amino acids (BCAAs) and essential amino acids (EAAs) are, how they differ from complete protein sources, their specific benefits and risks for the chronic illness population, natural food sources, dosing and safety considerations, mechanisms of action including mTOR signaling and the leucine trigger hypothesis, relevant genetics, and a practical protocol for muscle preservation during bed rest or reduced activity.

What Are BCAAs And EAAs
Amino acids are the building blocks of protein.
Nine of the 20 standard amino acids are classified as essential, meaning the human body cannot synthesize them and they must come from diet.
The branched-chain amino acids (BCAAs) are three of those nine: leucine, isoleucine, and valine, named for their branched side-chain structure.
BCAAs are unique among amino acids because they are metabolized primarily in skeletal muscle rather than the liver, and they play direct signaling roles in protein synthesis beyond their role as structural substrates. R
The essential amino acids (EAAs) include all nine: histidine, isoleucine, leucine, lysine, methionine, phenylalanine, threonine, tryptophan, and valine.
A complete protein source (whey, egg, meat, soy) contains all nine EAAs in ratios sufficient to support protein synthesis.
Taking BCAAs alone is fundamentally different from taking a complete EAA mixture or eating a whole protein, and this distinction matters greatly for clinical outcomes. R
Why The Distinction Matters
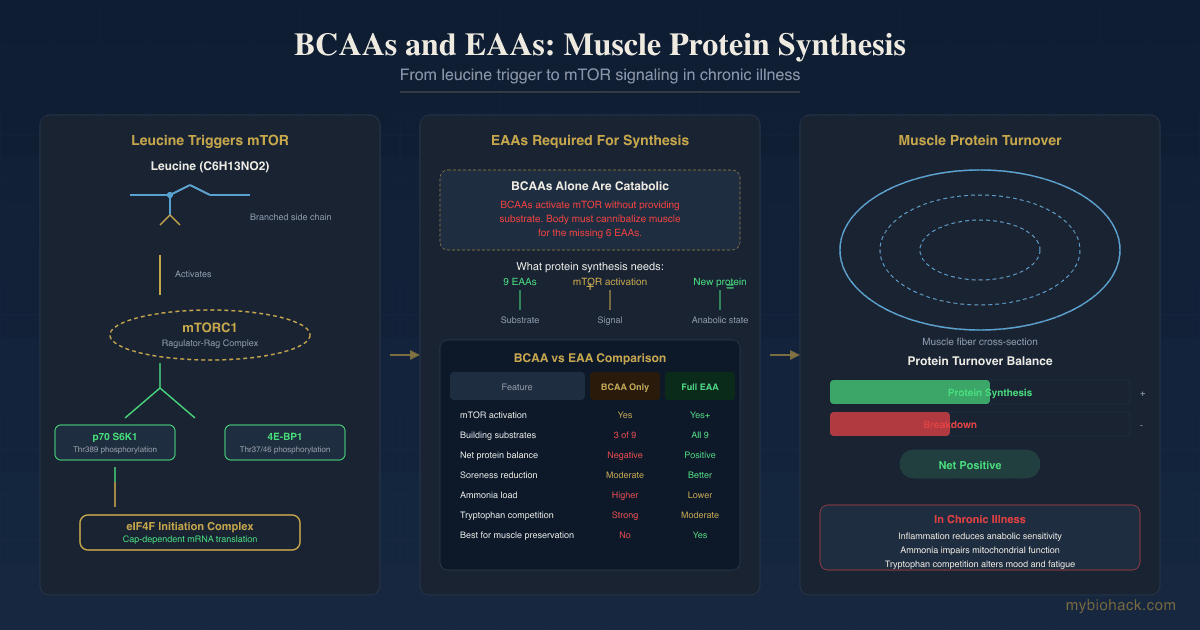
BCAAs activate the mammalian target of rapamycin (mTOR) signaling pathway and stimulate translation initiation, which is why they are marketed as anabolic. R
However, protein synthesis requires all nine EAAs as substrate.
If you take BCAAs without the other six EAAs, the remaining required amino acids must come from muscle protein breakdown, meaning you cannot create a net anabolic state with BCAAs alone. R
Two intravenous infusion studies in humans found that BCAAs alone actually decreased muscle protein synthesis while also decreasing protein breakdown, and the catabolic state (breakdown exceeding synthesis) persisted. R
A complete EAA mixture or intact protein source is required to achieve a net positive protein balance.

Benefits For Muscle Health In Chronic Illness
1. Leucine Triggers Muscle Protein Synthesis During Inactivity
Leucine is the primary EAA responsible for activating mTOR complex 1 (mTORC1) signaling and initiating translation of mRNA into protein.
A randomized, double-blind, placebo-controlled trial in middle-aged adults (52 +/- 1 years) found that leucine supplementation (0.06 g/kg per meal) during 14 days of bed rest partially protected knee extensor strength, endurance, and muscle quality, and reduced whole-body lean mass loss during the first 7 days. R
The protective effect was driven by a blunted reduction in muscle protein synthesis: the leucine group lost only 10% of postabsorptive synthetic capacity compared to 30% in controls. R
A separate bed rest study in older adults (67.8 years) found that 3-4 g leucine per meal reduced leg lean mass loss by more than half compared to controls (423 g vs. 1035 g lost). R
The effect appears greatest in people who are physically inactive and consuming less than approximately 1.0 g protein per kg per day. R
2. EAAs May Improve Muscle Mass And Strength In Sarcopenia And Chronic Conditions
A systematic review and meta-analysis of 39 randomized controlled trials in malnourished, frail, sarcopenic, and chronically ill older adults found that protein and EAA supplementation improved fat-free mass, muscle strength, and physical function, with EAA mixtures producing the largest effect on strength (SMD 0.82). R
A meta-analysis of 35 studies on BCAA-rich supplementation in older adults found small but significant improvements in muscle mass (SMD 0.25) and strength (SMD 0.35). R
These effects are relevant to the chronic illness population, where sarcopenia is common and driven by inflammation, reduced physical activity, and poor nutrient intake.
3. BCAAs May Reduce Muscle Breakdown During Catabolic States
BCAA infusion in postoperative patients improved nitrogen balance and reduced protein catabolism, as measured by 3-methylhistidine excretion. R
In a home-based bodyweight resistance exercise study, an EAA formulation (9 g EAAs including 3 g leucine) reduced urinary 3-methylhistidine by 32% compared to placebo, and was significantly more effective at attenuating myofibrillar protein breakdown than leucine-matched BCAAs alone. R
This reinforces the point that complete EAAs outperform isolated BCAAs for reducing muscle breakdown.
4. BCAAs May Reduce Muscle Soreness And Damage After Exertion
A systematic review and meta-analysis of 18 randomized controlled trials found that BCAA supplementation significantly reduced creatine kinase levels immediately and 72 hours after exercise-induced muscle damage, and reduced delayed onset muscle soreness from 24 to 96 hours post-exercise. R
For chronic illness patients who experience post-exertional malaise (PEM), this effect may help manage the recovery burden from even minimal activity, although the data come primarily from healthy athletes and may not translate directly to ME/CFS populations.
5. BCAAs Have A Therapeutic Role In Hepatic Encephalopathy
Liver cirrhosis alters BCAA metabolism and reduces circulating BCAA levels.
A Cochrane review of 16 randomized trials including 827 participants with hepatic encephalopathy found that BCAA supplementation improved encephalopathy manifestations (RR 0.73), with high-quality evidence. R
An updated 2026 Cochrane review of 18 trials (934 participants) confirmed that BCAAs likely reduce hepatic encephalopathy development or worsening. R
BCAAs also improved muscle mass (SMD 0.21) and albumin levels in cirrhosis patients according to a separate meta-analysis. R
However, a 12-month randomized controlled trial of 30 g daily BCAA versus equicaloric whey protein in cirrhosis patients found no significant difference in grip strength or lean mass, suggesting BCAAs are not superior to complete protein for sarcopenia in this population. R
6. BCAAs Compete With Tryptophan For Brain Transport (Relevant To Fatigue)
BCAAs and tryptophan share the same large neutral amino acid (LNAA) transporter at the blood-brain barrier.
Raising plasma BCAA levels reduces tryptophan uptake into the brain, which in turn reduces serotonin synthesis. R
This mechanism has been investigated for central fatigue during exercise, with mixed results.
One study found that BCAA supplementation during a 30 km cross-country race improved performance on complex cognitive tasks by 3-7%. R
However, another study found no effect of BCAA or tryptophan ingestion on exercise time to exhaustion. R
In rats, BCAA supplementation reduced both brain serotonin and catecholamine synthesis, and the reduction in catecholamines (dopamine, norepinephrine) may explain why BCAAs do not consistently improve physical performance despite reducing serotonin. R
For the chronic illness population, this mechanism has clinical relevance because serotonin dysregulation is implicated in fatigue, mood disorders, and gut-brain axis dysfunction.
Lowering brain serotonin through BCAA supplementation could theoretically worsen mood in susceptible individuals, although data in chronic illness populations are absent.
7. High-Protein BCAA Diets May Prevent Inactivity-Induced Insulin Resistance
A 60-day bed rest study in healthy women found that a high-protein diet enriched with BCAAs (1.6 g protein per kg per day including 11.4 g leucine) prevented the decline in insulin-mediated glucose uptake that occurred in the control group. R
This is relevant for chronic illness patients who often develop metabolic dysfunction from inactivity.
Natural Sources
BCAAs and EAAs are abundant in animal protein sources.
Animal proteins (meat, poultry, fish, eggs, dairy) provide complete EAA profiles with higher leucine content per gram than plant proteins. R
Primary dietary sources of BCAAs include:
- Beef and red meat
- Chicken and turkey
- Eggs
- Fish and shellfish
- Greek yogurt and milk
- Pork
- Tuna
In a Brazilian population study, the main contributors to BCAA intake were unprocessed red meat (22%), poultry (9.5%), bread and toast (6.5%), beans (5.9%), and rice (5.5%). R
Plant sources such as legumes, soy, nuts, and seeds also provide BCAAs but in lower concentrations per gram of protein.
For chronic illness patients with compromised appetite or digestive function, animal-based complete proteins are generally the most efficient way to maintain EAA intake.
See also: Organ Meats And Organ Supplements for nutrient-dense animal protein sources.
Dosage And Safety
General BCAA Dosage
The World Health Organization recommends daily intakes of 39 mg per kg body weight for leucine, 20 mg per kg for isoleucine, and 26 mg per kg for valine in healthy adults. R
Supplemental BCAA doses in research typically range from 3 g to 20 g per day, often in a 2:1:1 ratio of leucine to isoleucine to valine.
A meta-analysis of BCAA for exercise recovery found effective daily doses ranging from 3.15 g to 29.3 g per day, with higher total doses and longer supplementation periods producing better outcomes. R
For bed rest or inactivity, 3-4 g leucine per meal (approximately 0.06 g per kg per meal) has shown partial protection against muscle loss. R
Safety Guidelines
The German Federal Institute for Risk Assessment (BfR) has proposed guidance values for supplemental daily intake in isolated form: leucine 4.0 g, isoleucine 2.2 g, valine 2.0 g, total BCAAs 8.2 g per day. R
These apply to intake in addition to dietary protein.
Side effects reported in studies include gastrointestinal discomfort, nausea, tiredness, and in some cases, diarrhea. R
Amino acid supplements can also cause transient water retention and muscle cramps. R
Higher intakes (750-1000 mg per kg leucine) caused gastrointestinal discomfort in some individuals. R
Important Cautions
BCAAs without other EAAs can be net catabolic. Taking BCAAs alone, especially on an empty stomach or between meals, can lower circulating levels of other EAAs because the body uses them for substrate while the BCAAs activate mTOR signaling without providing the full amino acid pool needed for synthesis. R
This is known as BCAA antagonism, where excess leucine reduces plasma concentrations of the other EAAs. R
The solution is to take BCAAs alongside a complete protein source or as part of a full EAA mixture.
BCAA metabolism produces ammonia. In skeletal muscle, BCAA transamination generates glutamate, which is then deaminated to produce ammonia and alpha-ketoglutarate. R
Under normal conditions, the liver detoxifies ammonia through the urea cycle.
In hyperammonemic states such as liver cirrhosis, BCAA supplementation may enhance ammonia production from glutamine breakdown in the intestine and kidneys, potentially exerting harmful effects. R
However, in cirrhosis, the benefits for encephalopathy appear to outweigh this risk. R
Maple syrup urine disease (MSUD) is a rare autosomal recessive disorder caused by deficiency of the branched-chain alpha-ketoacid dehydrogenase complex, which prevents BCAA catabolism.
In MSUD, BCAAs and their ketoacids accumulate to neurotoxic levels, causing encephalopathy, seizures, and brain damage if untreated. R
This condition illustrates that BCAA metabolism must be functional for supplementation to be safe.
In people with normal BCAA metabolism, there is no evidence that supplemental BCAAs cause the same pathology, but the MSUD model demonstrates the neurotoxic potential of BCAA accumulation at extreme levels.
BCAAs reduce both serotonin and catecholamine synthesis by competing with tryptophan and tyrosine for brain transport.
In rats, BCAA supplementation induced anxiety-like behavior that was reversed by tryptophan supplementation but not by a selective serotonin reuptake inhibitor. R
The authors concluded the behavioral changes were independent of the serotonergic pathway and involved kynurenic acid, another tryptophan metabolite.
Whether this translates to humans at supplemental doses is unknown, but it warrants caution in individuals with mood disorders.
Recommended Approach For Chronic Illness
For muscle preservation during reduced activity or recovery from illness, complete protein or EAA supplementation is preferable to isolated BCAAs.
If BCAAs are used, they should be taken with a complete protein source or full EAA mixture, not alone.
A practical baseline for muscle preservation during inactivity is 1.2-1.6 g protein per kg body weight per day, with at least 2.5-3 g leucine per meal. R
See also: HMB (Beta-Hydroxy-Beta-Methylbutyrate) for a leucine metabolite that may preserve muscle during catabolic stress.
See also: Creatine for another muscle-supporting compound with distinct mechanisms.
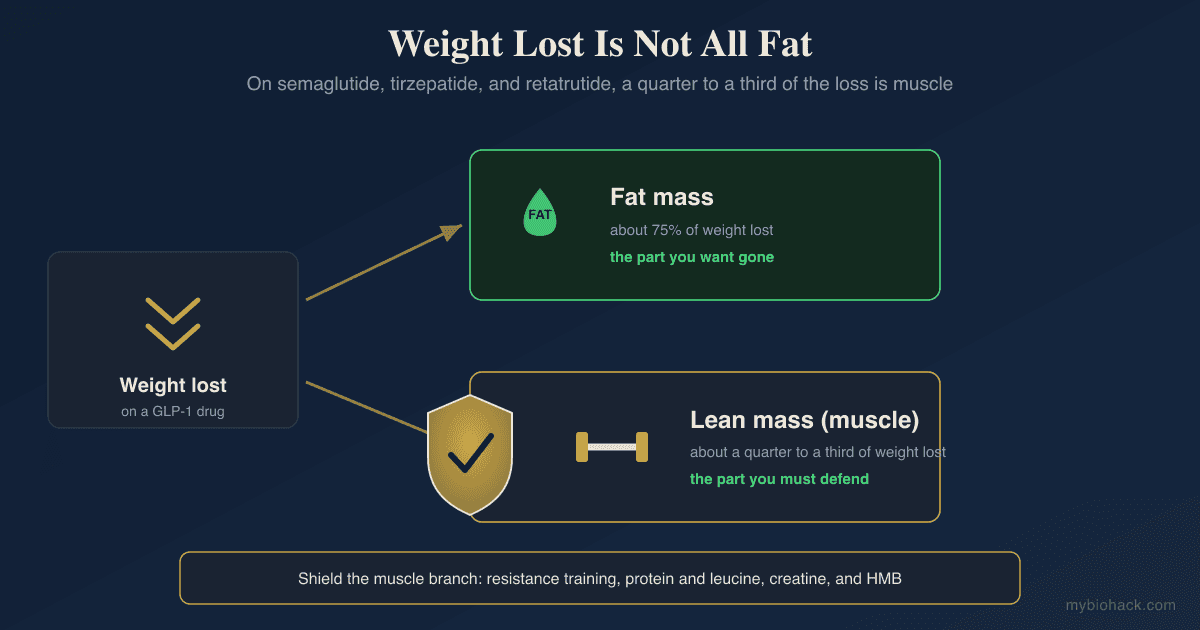
See also: Keeping Muscle On GLP-1 Drugs for a related protocol on muscle preservation during weight loss.
Mechanisms Of Action
Simple:
- BCAAs, particularly leucine, signal to your muscle cells to start building protein, like a key turning an engine on, but the engine still needs all nine essential amino acids as fuel to run.
- If you supply only the three BCAAs, your body must break down existing muscle tissue to get the other six essential amino acids needed for new protein, which defeats the purpose.
- BCAAs compete with tryptophan at the blood-brain barrier, which means taking BCAAs can reduce serotonin production in the brain, potentially affecting mood, fatigue, and appetite.

Advanced:
- mTORC1 Activation By Leucine: Leucine activates mechanistic target of rapamycin complex 1 (mTORC1) through a mechanism involving the Ragulator-Rag complex, which recruits mTORC1 to the lysosomal surface where it interacts with the GTPase Rheb (Ras homolog enriched in brain). R Leucine promotes mTOR translocation to the cell periphery, enhancing co-localization with the lysosome and subsequent phosphorylation of downstream effectors including p70 S6 kinase 1 (S6K1) at Thr389 and 4E-binding protein 1 (4E-BP1) at Thr37/46. R Phosphorylation of 4E-BP1 releases eukaryotic initiation factor 4E (eIF4E), allowing formation of the eIF4F initiation complex and the initiation of cap-dependent mRNA translation. R The presence of the other EAAs enhances S6K1 phosphorylation by 60-75% beyond the effect of leucine alone. R
- BCAA Transamination And Ammonia Production: In skeletal muscle, BCAAs are transaminated with alpha-ketoglutarate by branched-chain aminotransferase (BCAT) to generate branched-chain ketoacids (BCKAs) and glutamate. R Glutamate can then be deaminated by glutamate dehydrogenase to produce alpha-ketoglutarate and ammonia (NH3), or used for glutamine synthesis via glutamine synthetase. R The ammonia is normally detoxified in the liver via the urea cycle, but in hyperammonemic states, this pathway contributes to the ammonia load and to cataplerosis (drain of TCA cycle intermediates). R
- BCAA Antagonism On Other EAAs: Excess leucine intake activates key enzymes in BCAA catabolism, including BCAT and the branched-chain alpha-ketoacid dehydrogenase complex (BCKDC), which increases leucine oxidation and can lower plasma concentrations of the other BCAAs and EAAs. R This effect, termed BCAA antagonism, means that isolated BCAA supplementation without other EAAs may reduce the availability of methionine, phenylalanine, threonine, and other essential amino acids needed for protein synthesis. R
- LNAA Competition At The Blood-Brain Barrier: BCAAs, tryptophan, tyrosine, phenylalanine, methionine, and threonine are all transported across the blood-brain barrier by the L-type amino acid transporter 1 (LAT1, encoded by SLC7A5). R When plasma BCAA concentrations rise, they competitively inhibit tryptophan and tyrosine uptake into the brain, reducing the synthesis of serotonin and catecholamines (dopamine, norepinephrine), respectively. R This mechanism underlies both the potential anti-fatigue effects and the potential mood-disrupting effects of BCAA supplementation.
- Anabolic Resistance In Inflammation And Endotoxin Exposure: In rats, lipopolysaccharide (LPS) administration disrupts the leucine signaling pathway, blunting leucine-induced phosphorylation of mTOR, S6K1, 4E-BP1, and ribosomal protein S6 in skeletal muscle. R This effect was not explained by changes in insulin or IGF-I and was independent of glucocorticoid signaling, suggesting that systemic inflammation directly impairs the muscle's ability to respond to leucine. R This has direct relevance to chronic illness, where low-grade endotoxemia from intestinal permeability (a core feature of the Junction Dysfunction framework) may create leucine resistance even when protein intake is adequate.
- BCAA Catabolism In ME/CFS: Proteomic analysis of ME/CFS patient-derived lymphoblasts found elevated levels of BCKDHA and BCKDHB, the catalytic subunits of the BCKDC, indicating increased BCAA catabolism. R This suggests that ME/CFS metabolism is shifted toward using BCAAs as an alternative oxidative substrate, which could contribute to reduced BCAA availability for muscle protein synthesis and may partially explain the muscle wasting and fatigue seen in this population. R
- Leucine And Insulin Secretion: Leucine stimulates insulin secretion from pancreatic beta-cells by allosterically activating glutamate dehydrogenase, which increases ATP production from glutamate oxidation. R Leucine also potentiates glucose-stimulated insulin secretion and can stimulate GLP-1 release from intestinal L-cells. R This insulinotropic effect may contribute to the improved glucose homeostasis observed with high-protein BCAA diets during bed rest. R
Genetics
BCKDHA
The BCKDHA gene encodes the E1-alpha subunit of the branched-chain alpha-ketoacid dehydrogenase complex, the rate-limiting enzyme in BCAA catabolism.
Loss-of-function mutations cause maple syrup urine disease (MSUD), characterized by accumulation of BCAAs and their ketoacids to neurotoxic levels. R
rs112518703: a rare loss-of-function variant that reduces BCKDC activity; heterozygous carriers may have altered BCAA clearance, though population impact is minimal. R
SLC7A5
SLC7A5 encodes the L-type amino acid transporter 1 (LAT1), which transports BCAAs, tryptophan, tyrosine, and other LNAAs across cell membranes and the blood-brain barrier.
This transporter determines the ratio of BCAAs to aromatic amino acids available for neurotransmitter synthesis.
rs137854577: a missense variant in SLC7A5 that reduces transport capacity; may alter brain tryptophan availability and serotonin synthesis, potentially affecting mood and fatigue susceptibility (preliminary data).
BCAT2
BCAT2 encodes mitochondrial branched-chain aminotransferase, which catalyzes the first step in BCAA catabolism by transferring the amino group to alpha-ketoglutarate.
rs11548193: an intronic variant associated with altered circulating BCAA levels in genome-wide association studies; may influence BCAA clearance rate and muscle protein synthesis efficiency. R
PPARGC1A
PPARGC1A encodes PGC-1alpha, a master regulator of mitochondrial biogenesis and oxidative metabolism that also regulates BCAA catabolism through transcriptional control of BCAT2 and BCKDH.
rs8192678 (Gly482Ser): a common variant associated with reduced PGC-1alpha activity; carriers may have impaired mitochondrial adaptation to inactivity and reduced capacity for BCAA oxidation, potentially increasing the risk of muscle loss during chronic illness. R
More Research
- BCAA supplementation in heart failure remains controversial with conflicting data on whether it helps or harms outcomes, due to the complex interplay between BCAA metabolism, ammonia production, and cardiac energy metabolism. R
- BCAA levels are consistently associated with insulin resistance and type 2 diabetes in population studies, though whether elevated BCAAs are causal or a consequence of impaired catabolism remains debated. R
- Leucine's anabolic effect appears to wane over time during prolonged bed rest, with protection against lean mass loss observed at 7 days but not sustained at 14 days in some studies. R This suggests a transient desynchronization effect where chronic supplementation may upregulate BCAA catabolic enzymes and reduce effectiveness.
- The ketone body beta-hydroxybutyrate may partially mediate leucine's effects through shared metabolic intermediates, as leucine is ketogenic and produces acetoacetate and acetyl-CoA. For biomarker testing of metabolic status, I use the Cellular Zoomer (Vibrant Wellness) to assess organic acids, mitochondrial function, and BCAA catabolic markers.
- BCKA supplementation (branched-chain ketoacids) may offer advantages over BCAAs in hyperammonemic states by supplying the carbon skeletons without the nitrogen load, potentially reducing ammonia production and cataplerosis. R
- Taurine is another conditionally essential amino acid with muscle-protective and metabolic effects that operates through distinct mechanisms from the BCAAs. See also: Taurine.
- The carnivore diet eliminates plant-based antinutrients and provides highly bioavailable complete protein, but its role in muscle preservation during chronic illness is underexplored.
- Methylation status influences BCAA metabolism through the methionine cycle, as methionine is one of the EAAs that becomes limiting when BCAA antagonism reduces plasma EAA levels. See also: Methylation.
- Glutamate dysregulation from enhanced BCAA transamination may contribute to neuronal excitotoxicity and glymphatic dysfunction in susceptible individuals. See also: Glutamate Dysregulation And Neuroinflammation.
- Mitochondrial function determines how efficiently BCAAs are used for energy versus protein synthesis; impaired oxidative phosphorylation shifts BCAAs toward transamination and ammonia production. See also: Mitochondrial Psychobiology.
Protocol: Muscle Preservation During Bed Rest Or Reduced Activity
1. Prioritize Total Protein Intake
Aim for 1.2-1.6 g protein per kg body weight per day, distributed across 3-4 meals.
Each meal should contain at least 25-30 g protein with 2.5-3 g leucine to trigger mTOR activation. R
Animal-based proteins (whey, egg, beef, chicken, fish) provide the most efficient EAA profile per gram.
2. Consider EAA Supplementation If Appetite Is Low
If whole food intake is insufficient, a complete EAA supplement (containing all nine EAAs) is superior to isolated BCAAs for preserving muscle.
Dose: 10-15 g EAAs per serving, containing at least 3 g leucine, taken between meals or with meals.
Look for formulations that include all nine EAAs rather than just the three BCAAs.
3. Use BCAAs Strategically, Not In Isolation
If BCAAs alone are used (e.g., for reducing post-exertional soreness), take them alongside or shortly after a complete protein source.
Do not take BCAAs between meals on an empty stomach as a stand-alone supplement.
The 2:1:1 ratio (leucine to isoleucine to valine) is the most common and most studied.
4. Address Inflammation And Anabolic Resistance
Leucine resistance is driven by systemic inflammation, endotoxemia, and mitochondrial dysfunction. R
Supporting the glycocalyx, reducing intestinal permeability, and managing endotoxin burden may improve the muscle's ability to respond to amino acid signals.
See also: Improving And Rebuilding The Glycocalyx, see also: TCLS And Junction Dysfunction
5. Combine With Mechanical Loading When Possible
Even minimal contractile activity (isometric contractions, neuromuscular electrical stimulation) enhances the muscle's sensitivity to amino acid stimulation.
Bed rest alone blunts the EAA-induced increase in mTORC1 signaling and amino acid transporter expression. R
Any tolerable movement, even if not conventional exercise, improves the anabolic response to protein.
6. Monitor Serum Ammonia If Liver Function Is Compromised
For patients with known liver disease or elevated ammonia, BCAA doses should be supervised and ammonia levels monitored, as BCAA catabolism contributes to the ammonia pool. R
The benefit-risk balance favors BCAA use in hepatic encephalopathy, but individual monitoring is warranted. R
7. Consider HMB As An Alternative Or Adjunct
Beta-hydroxy-beta-methylbutyrate (HMB) is a leucine metabolite that inhibits muscle protein breakdown and may be more effective than leucine alone in some catabolic states. R
See also: HMB (Beta-Hydroxy-Beta-Methylbutyrate)
BCAA Supplement: Consider formulations with a 2:1:1 leucine to isoleucine to valine ratio.
EAA Supplement: A complete EAA powder provides all nine essential amino acids and is preferable to isolated BCAAs for muscle preservation.
Whey Protein Isolate: A complete, rapidly absorbed protein source that naturally contains all EAAs and BCAAs in optimal ratios.
HMB Supplement: The leucine metabolite with direct anti-catabolic effects on muscle tissue.
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Quercetin
500mg 2x/day
Vitamin D3 + K2
5000 IU + 200mcg/day
Magnesium Glycinate
400mg at bedtime