8-OHdG: The DNA Damage Biomarker That Tells You How Fast You Are Aging At The Cellular Level
By Jacob Gordon, INHC, FMT-CThis article contains affiliate links. As an Amazon Associate, MyBioHack earns from qualifying purchases at no extra cost to you. We only link products we research and stand behind.
Every cell in your body produces oxidative damage to its own deoxyribonucleic acid (DNA) every day, and the rate at which that damage accumulates and gets repaired determines your long-term cancer risk, aging trajectory, and chronic disease susceptibility.
In this post, we will discuss what 8-hydroxy-2'-deoxyguanosine (8-OHdG) is, how it forms, why guanine is uniquely vulnerable to oxidation, the three-enzyme repair system that keeps it in check, what elevated levels predict in terms of disease, how to measure it, what drives it up, and what actually lowers it.

Basics: What 8-OHdG Is And Where It Comes From
8-OHdG is the abbreviated form of 8-hydroxy-2'-deoxyguanosine, also written as 8-oxodG (8-oxo-7,8-dihydro-2'-deoxyguanosine).
Both terms refer to the same molecule: the oxidized nucleoside form of guanine that is produced when reactive oxygen species (ROS) attack the guanine base in deoxyribonucleic acid (DNA). R
The distinction in naming is technical: 8-OHdG refers to the hydroxyl tautomer and 8-oxodG to the keto tautomer, but they are interconvertible and both are used in the clinical literature to describe the same oxidative lesion.
8-OHdG is produced by two routes:
The first is direct in situ oxidation of guanine already incorporated into nuclear or mitochondrial DNA by hydroxyl radicals (OH•) and other ROS attacking the C8 position of guanine. R
The second is incorporation of oxidized nucleotides from the nucleotide pool during DNA replication: free deoxyguanosine triphosphate (dGTP) in the cytoplasm is oxidized to 8-oxo-dGTP, which DNA polymerase can then insert into the growing DNA strand opposite adenine (A) rather than cytosine (C), directly introducing errors during replication. R
Free deoxyribonucleoside triphosphate (dNTP) pool molecules in the cytoplasm are up to 13,000-fold more susceptible to oxidative damage than bases in duplex DNA, making the nucleotide pool a particularly important source of incorporated 8-oxodG. R
After DNA repair enzymes remove 8-OHdG from damaged DNA, the excised nucleoside is water-soluble and cannot be reincorporated into genomic DNA (deoxynucleotide kinase activity converting it back to 8-oxo-dGTP is very low). R
It crosses cell membranes and enters blood and urine, which is why urinary 8-OHdG is a reliable, non-invasive measure of whole-body oxidative DNA damage rates. R
8-OHdG is the most widely studied oxidative DNA lesion in human medicine, used as a biomarker for cancer risk, cardiovascular disease, diabetes, neurodegeneration, occupational toxin exposure, and aging. R
Why Guanine Is The Most Oxidizable DNA Base
DNA contains four bases: adenine (A), cytosine (C), guanine (G), and thymine (T).
Guanine has the lowest redox potential of the four, meaning it gives up electrons more readily than A, C, or T. R
This makes guanine the preferred target for oxidative attack by ROS, particularly the hydroxyl radical (OH•), which is generated through the Fenton reaction when hydrogen peroxide (H2O2) reacts with ferrous iron (Fe2+). R
The C8 position of guanine is especially reactive, and oxidation there yields 8-oxoguanine (8-oxoG), the base lesion found in DNA, or its nucleoside form 8-OHdG when found in the nucleotide pool or after repair excision. R
8-OHdG is considered one of the predominant forms of free radical-induced oxidative lesions in both nuclear and mitochondrial DNA. R
Mitochondrial DNA is particularly vulnerable because mitochondria are the primary site of cellular ROS production (through oxidative phosphorylation) and mitochondrial DNA lacks the histone packaging that partially protects nuclear DNA from oxidative attack. R
The Mutation Problem: G:C To T:A Transversions
The reason 8-OHdG matters biologically is its mutagenic potential.
Normal guanine pairs with cytosine (C) in the Watson-Crick double helix.
8-Oxoguanine (8-oxoG) has a different electronic structure that allows it to pair with adenine (A) as well as cytosine. R
When DNA polymerase encounters 8-oxoG during replication and inserts A opposite it, the next round of replication produces a T:A pair where G:C should be.
This G:C to T:A transversion is one of the most frequent somatic mutations found in human cancers. R
If the transversion strikes a tumor suppressor gene like TP53 or an oncogene codon at a critical position, one oxidative lesion in the wrong place at the wrong time can initiate a cancerous clone.
Guanine oxidation also tends to occur preferentially in GC-rich regulatory regions of the genome rather than randomly across coding sequence, meaning 8-oxoG lesions can affect gene expression even when they do not cause classic mutations. R
Accumulation of 8-oxoG in the promoter regions of pro-inflammatory genes facilitates recruitment of sequence-specific transcription factors such as nuclear factor kappa B (NF-κB) and Sp1, and 8-oxoguanine DNA glycosylase 1 (OGG1) recognition of these lesions can trigger gene expression changes that drive inflammatory cascades. R
This means 8-oxoG is not only a passive lesion to be repaired, but also functions as an epigenetic signal that can alter transcriptional programs in response to oxidative stress. R
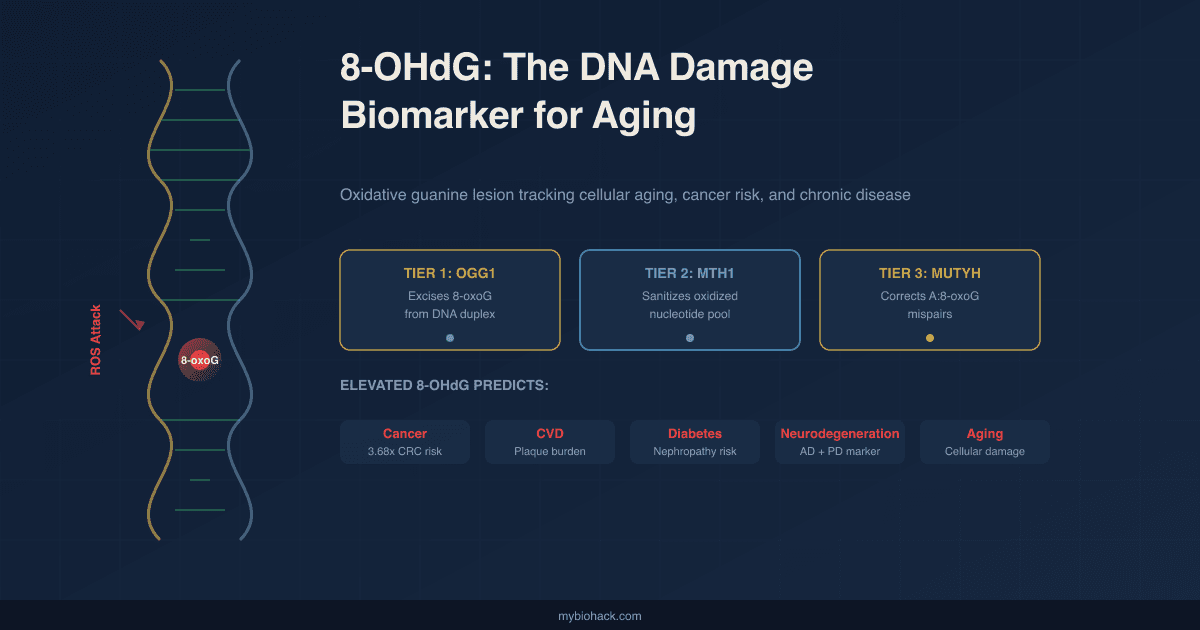
The Three-Tier Repair System: OGG1, MTH1, And MUTYH
Cells maintain three distinct enzymes to prevent 8-oxoG accumulation, collectively called the GO (guanine oxidation) repair system in bacteria and its eukaryotic equivalent in mammals. R
Tier 1: OGG1 Removes 8-oxoG From DNA
OGG1 (8-oxoguanine DNA glycosylase 1) is a bifunctional base excision repair (BER) glycosylase that is the primary repair enzyme for 8-oxoG lesions in duplex DNA. R
When OGG1 encounters 8-oxoG paired opposite cytosine (C) in the DNA strand, it recognizes the lesion, excises the damaged base by hydrolyzing the glycosidic bond, and creates an apurinic/apyrimidinic (AP) site.
Apurinic/apyrimidinic endonuclease 1 (APE1) then processes the 3' end of the resulting strand break, and DNA polymerase fills the gap with an undamaged cytosine. R
OGG1 also has a role in gene regulation: OGG1-substrate interactions at regulatory DNA regions cause conformational changes that affect chromatin structure and transcription factor recruitment, linking DNA repair directly to inflammatory gene expression. R
The 8-OHdG excised by OGG1 (and by nucleotide excision repair (NER)) then enters blood and urine as the freely circulating nucleoside that can be measured clinically. R
Tier 2: MTH1 Sanitizes The Nucleotide Pool
MTH1 (also known as NUDT1, nudix hydrolase 1) is the nucleotide pool sanitizing enzyme.
It hydrolyzes 8-oxo-dGTP and 8-oxo-dATP in the cytoplasm to the monophosphate form (8-oxo-dGMP), which cannot be incorporated into DNA by polymerase. R
MTH1 prevents the secondary source of genomic 8-oxoG accumulation, namely erroneous incorporation of oxidized nucleotides during replication. R
MTH1 expression is elevated in many cancer types compared with adjacent normal tissue, which has driven interest in MTH1 inhibitors as anti-cancer agents, although the clinical significance of this approach remains controversial. R
Tier 3: MUTYH Corrects Mispairs
MUTYH (MutY DNA glycosylase, the human homolog of bacterial MutY) addresses the case where 8-oxoG has already mispaired with adenine in the DNA duplex during replication.
MUTYH recognizes the 8-oxoG:A mispair, excises the adenine (A) from the undamaged strand, and allows DNA polymerase to insert cytosine (C) opposite 8-oxoG instead. R
OGG1 can then remove the 8-oxoG from the corrected duplex, completing the repair cycle. R
Why all three tiers matter:
Mice deficient in both OGG1 and MUTYH develop spontaneous cancers in multiple organs, whereas single knockouts show milder phenotypes. R
The triple knockout of OGG1, MTH1, and MUTYH produces significantly increased G:C to T:A mutagenesis that neither single nor double knockouts alone manifest at the same level. R
This three-layered redundancy reflects how evolutionarily critical 8-oxoG management is for genome stability.
What Elevated 8-OHdG Predicts: Disease Associations
Urinary 8-OHdG reflects whole-body oxidative DNA damage rates and has been studied as a biomarker across a broad range of chronic and degenerative conditions.
Cancer:
Elevated urinary 8-OHdG has been detected in patients with multiple cancer types including lung, colorectal, breast, prostate, and ovarian cancer. R
Individuals with urinary 8-OHdG concentrations above 1.5 nmol/mmol creatinine face approximately 3.68-fold higher colorectal cancer risk compared with those with lower levels. R
8-OHdG is consistently higher in cancer tissue compared with adjacent normal tissue in multiple tumor types, and levels rise with cancer progression and metastasis. R
Cardiovascular disease:
Elevated 8-OHdG levels have been detected in human atherosclerotic plaques. R
A systematic review of 18 studies found elevated 8-OHdG consistently associated with atherosclerosis, heart failure, and stroke. R
Urinary 8-OHdG levels in coronary artery disease (CAD) patients were significantly higher than controls before coronary artery bypass grafting (CABG) surgery, and spiked further in the 5-day post-surgical period before declining toward normal at 6 months post-surgery. R
The 8-OHdG levels correlated with urinary 8-isoprostane F2-alpha (8-isoPGF2α), a lipid peroxidation marker, confirming both are capturing the same underlying oxidative burden. R
Diabetes:
Elevated urinary 8-OHdG is found in diabetic patients with hyperglycemia. R
The level of urinary 8-OHdG in diabetes correlates with the severity of diabetic nephropathy and retinopathy, suggesting it tracks microvascular complication risk. R
8-OHdG rises even in prediabetes, before formal diabetes diagnosis, making it potentially more sensitive for early oxidative metabolic dysfunction than standard glycemic markers. R
Neurodegeneration:
Elevated 8-OHdG is found in cerebrospinal fluid (CSF) and brain tissue in Alzheimer's disease and Parkinson's disease. R
Old monkey substantia nigra (the region lost in Parkinson's disease) shows higher 8-OHdG than young monkey substantia nigra, directly linking oxidative DNA damage to age-related neuronal vulnerability in the relevant brain region. R
Inflammatory bowel disease:
8-OHdG levels are elevated in ulcerative colitis (UC), and both OGG1 and MTH1 expression increase in UC-associated carcinoma, reflecting a repair system under sustained oxidative demand that eventually fails to prevent malignant transformation. R
Non-alcoholic steatohepatitis (NASH):
Serum 8-OHdG distinguishes non-alcoholic steatohepatitis (NASH) from non-alcoholic fatty liver (NAFL) and serves as a diagnostic marker for the more dangerous inflammatory form of fatty liver disease. R
Aging:
8-OHdG levels increase with age in both animal and human studies, consistent with the established hypothesis that cumulative oxidative DNA damage is a driver of the aging phenotype. R
Elderly individuals with elevated plasma 8-OHdG face increased risk of motoric cognitive risk syndrome, suggesting it tracks motor-cognitive functional decline independent of overt disease. R
What Drives 8-OHdG Up
Smoking:
Smoking is the most consistently identified factor elevating urinary 8-OHdG across human studies. R
Tobacco smoke delivers both direct ROS and activates inflammatory cascades that generate endogenous oxidants, compounding genomic guanine oxidation. R
Hyperglycemia:
High blood glucose drives the glycation of proteins, advanced glycation end products (AGEs), and activation of NADPH oxidase (NOX) complexes, all of which increase ROS production and guanine oxidation in proportion to glucose levels. R
Chronic inflammation:
Macrophages in active inflammatory states produce large quantities of ROS and reactive nitrogen species (RNS) via inducible nitric oxide synthase (iNOS) and NOX, attacking not only invading pathogens but also nearby tissue DNA. R
Inflammatory bowel disease, rheumatoid arthritis, and other chronic inflammatory conditions consistently show elevated 8-OHdG. R
Heavy metals:
Cadmium, arsenic, chromium, and other heavy metals generate ROS, deplete glutathione (GSH), and impair DNA repair enzyme function simultaneously, producing compounding increases in 8-OHdG. R
Polycyclic aromatic hydrocarbons (PAHs) and particulate matter:
Occupational and environmental exposure to PAHs (from combustion, industrial processes, and cooking fumes) and fine particulate matter (PM2.5) elevates urinary 8-OHdG. R
Obesity:
8-OHdG levels are higher in obese individuals, reflecting elevated oxidative stress from excess adipose-tissue-derived ROS production and mitochondrial dysfunction. R
Excessive acute exercise:
Exhaustive exercise increases ROS production and 8-OHdG in the short term, particularly at high intensities. R
This is a MAYBE area: the increase is transient and modest with moderate exercise, and regular aerobic training over time lowers resting 8-OHdG by improving antioxidant enzyme capacity. R
Shift work and sleep disruption:
Long working hours, shift work, and sleep deprivation are associated with elevated urinary 8-OHdG, likely through circadian disruption of antioxidant enzyme expression and melatonin production. R
Ionizing radiation:
Medical imaging procedures, radiotherapy, and occupational radiation exposure all elevate 8-OHdG in proportion to the dose received. R
How To Lower 8-OHdG
1. Foundational: Reduce The Sources
The most impactful interventions are upstream: removing the inputs that drive ROS production.
Smoking cessation, blood glucose control, reduction of heavy metal exposures, air quality improvement (especially PM2.5), and management of chronic inflammatory conditions will lower 8-OHdG more reliably than any supplement. R
2. Antioxidant Nutrients That Reduce 8-OHdG
Dietary antioxidant interventions at higher-than-typical intake levels produce measurable reductions in leukocyte 8-OHdG in human studies. R
NAC is the primary substrate for glutathione resynthesis, providing cysteine (the rate-limiting amino acid for glutathione (GSH) production). R
Glutathione directly neutralizes hydroxyl radicals and H2O2, preventing them from reaching DNA and oxidizing guanine. R
Alpha-lipoic acid (ALA) is a cofactor for mitochondrial enzymes and a direct antioxidant that regenerates other antioxidants including vitamin C, vitamin E, and glutathione. R
Vitamin C is the primary water-soluble antioxidant in plasma, intercepting aqueous ROS before they reach DNA. R
Vitamin C supplementation reduces 8-OHdG levels in sperm DNA in human studies. R
Vitamin E (mixed tocopherols):
Alpha-tocopherol is the primary lipid-phase chain-breaking antioxidant, intercepting lipid peroxyl radicals in cell membranes before they generate secondary ROS that reach DNA. R
See the tocopherols post for why a mixed tocopherol formula with high gamma and delta fractions is superior to isolated alpha-tocopherol for anti-inflammatory and anti-oxidative purposes.
Glutathione (liposomal or reduced form):
Directly replenishes the most important intracellular antioxidant without requiring enzymatic synthesis.
Optimal for situations where the GSH synthesis pathway is compromised, such as in heavy metal or mycotoxin burden. R
3. Regular Moderate Exercise
Regular aerobic exercise at moderate intensity consistently lowers resting 8-OHdG levels over time by upregulating endogenous antioxidant enzyme expression including superoxide dismutase (SOD), catalase, and glutathione peroxidase (GPx). R
A 10-day intense military field training study demonstrated a 23% decline in plasma 8-OHdG after the training course, accompanied by a 175% rise in reduced glutathione (GSH), demonstrating that even severe physiological stress combined with adaptation produces a net antioxidant adaptation. R
Avoid excessive acute exhaustive exercise without adequate antioxidant nutritional support, as this transiently spikes 8-OHdG before adaptation occurs. R
4. Diet Modification
A diet rich in antioxidant nutrients (fruits, vegetables, and whole grains above typical Western intake levels) produced a 22% reduction in leukocyte 8-OHdG in a controlled human dietary intervention, with a significant downward trend throughout the intervention period. R
Diets high in processed meats, refined carbohydrates, and seed oils high in oxidized polyunsaturated fatty acids (PUFAs) drive ROS generation and elevate 8-OHdG.
Blood glucose control through low-glycemic eating patterns removes one of the primary endogenous drivers of guanine oxidation.
5. Sleep And Circadian Alignment
Shift work and disrupted sleep consistently elevate urinary 8-OHdG. R
Melatonin is a direct antioxidant that reaches the mitochondrial matrix, protecting mitochondrial DNA from guanine oxidation during sleep.
Prioritizing consistent sleep timing and adequate duration supports both melatonin production and the circadian regulation of DNA repair enzyme expression.
Testing: How And Where To Measure It
Measurement Methods
Urinary 8-OHdG is the standard non-invasive measurement method and reflects whole-body oxidative DNA damage flux (damage rate minus repair rate). R
Results are typically expressed as nanograms per milligram (ng/mg) creatinine to correct for urine concentration.
The established ELISA-derived reference range for urinary 8-OHdG is approximately 43.9 ± 42.1 ng/mg creatinine for females and 29.6 ± 24.5 ng/mg creatinine for males, with women showing significantly higher baseline values. R
Important caveat on measurement: 8-OHdG shows circadian variation, with day-night differences documented in continuous sampling studies, meaning single-spot urine measurements should be collected at consistent times (morning first void is standard) and interpreted accordingly. R
Serum and leukocyte DNA 8-OHdG are also measured but are less standardized than urinary measurement.
High-performance liquid chromatography with electrochemical detection (HPLC-ECD) is the gold-standard method for laboratory measurement, with sensitivity down to the femtomolar range. R
Enzyme-linked immunosorbent assay (ELISA) is widely used in clinical and research settings as a more accessible method, though prone to higher inter-laboratory variability. R
Functional Lab Panels
I use the Cellular Zoomer (Vibrant Wellness) to assess organic acids and mitochondrial function markers that contextualize 8-OHdG levels, since mitochondrial dysfunction is a primary driver of guanine oxidation.
I use the Toxin Zoomer (Vibrant Wellness) to assess heavy metals, mycotoxins, and environmental chemicals that drive 8-OHdG elevation through ROS induction and DNA repair suppression.
The Nutrient Zoomer assesses glutathione, vitamins C and E, and other antioxidant micronutrients that determine the body's capacity to prevent guanine oxidation.
Urinary 8-OHdG is offered as a standalone test through several functional medicine labs. For direct clinical interpretation of urinary 8-OHdG alongside other oxidative stress markers, ask your practitioner about ordering through Genova Diagnostics or Doctor's Data, which offer validated urinary organic acid and oxidative damage panels.
Mechanisms Of Action
Simple:
- ROS attack the C8 position of guanine in DNA, producing 8-OHdG, because guanine has the lowest electron-donating potential of the four DNA bases and is most easily oxidized.
- 8-OHdG can pair with adenine instead of cytosine during DNA replication, causing G:C to T:A transversion mutations that are among the most frequent somatic mutations in human cancers.
- OGG1 is the primary repair enzyme that recognizes and excises 8-oxoG from DNA, creating an abasic site that is filled with undamaged cytosine; the excised 8-OHdG enters urine.
- MTH1 sanitizes the nucleotide pool by hydrolysing oxidized dGTP before it gets incorporated into DNA, preventing a second route of 8-oxoG accumulation.
- MUTYH corrects 8-oxoG:adenine mispairs that escape MTH1 prevention, excising the wrongly inserted adenine and giving OGG1 a second chance at removing 8-oxoG.
- The amount of 8-OHdG appearing in urine reflects the net balance between how fast ROS are being generated and how efficiently OGG1-BER is excising lesions.
Advanced:
- Hydroxyl radical attack at C8: The hydroxyl radical (OH•) is the most reactive ROS species for DNA damage. It adds to the C8 of guanine in a radical addition reaction, producing an 8-hydroxyguanosyl radical that is then oxidized (by O2 or other oxidants) or reduced to yield 8-oxoG. R The electron affinity gradient across the four bases (G < A < C < T) means long-range electron transfer through the DNA pi-stacking also concentrates oxidative damage preferentially at guanine runs, particularly G-quadruplex-forming sequences in promoters. R
- OGG1-BER cascade: OGG1 is a bifunctional glycosylase with both glycosylase activity (cleaving the N-glycosidic bond between 8-oxoG and deoxyribose) and beta-lyase activity (cleaving the phosphodiester backbone 3' to the abasic site). R The AP site generated by glycosylase cleavage is processed by APE1 (apurinic/apyrimidinic endonuclease 1), which incises the phosphodiester backbone 5' to the AP site, leaving a 3'-OH group. R DNA polymerase beta then fills the one-nucleotide gap with undamaged dCMP and DNA ligase seals the nick. R Beyond direct repair, OGG1 binding to 8-oxoG in gene regulatory regions activates mitogen and stress-activated kinase 1 (MSK1), which promotes phosphorylation of RelA/p65 at Ser276, increasing expression of NF-κB target genes including pro-inflammatory cytokines. R
- MTH1 nucleotide pool sanitization: MTH1 is a Nudix hydrolase that cleaves the pyrophosphate bond of 8-oxo-dGTP, yielding 8-oxo-dGMP and inorganic pyrophosphate (PPi). R 8-oxo-dGMP cannot be phosphorylated efficiently back to 8-oxo-dGTP by deoxynucleotide kinase, effectively removing it from the replication-competent nucleotide pool. R Cancer cells frequently overexpress MTH1 to survive their own elevated ROS production, which makes MTH1 a drug target; however, MTH1 inhibitor efficacy as an anticancer strategy has been inconsistent across tumor types, suggesting context-specific dependency. R
- MUTYH mispair correction: MUTYH recognizes the distorted helical geometry of the 8-oxoG:A mispair, inserts a wedge residue into the DNA minor groove, and flips the adenine out of the helix into its active-site pocket where N-glycosidic bond cleavage occurs. R After adenine excision, the remaining 8-oxoG:AP site undergoes OGG1-initiated BER. Heterozygous germline mutations in MUTYH cause MUTYH-associated polyposis (MAP), an autosomal recessive condition with markedly elevated colorectal cancer risk due to accumulation of G:C to T:A transversions in the APC (adenomatous polyposis coli) gene. R
- Glutathione-mediated protection: The glutathione redox cycle involves glutathione peroxidase (GPx) reducing H2O2 and lipid hydroperoxides using reduced glutathione (GSH) as electron donor, producing oxidized glutathione (GSSG). R Glutathione reductase then regenerates GSH from GSSG using NADPH (nicotinamide adenine dinucleotide phosphate). R The total antioxidant capacity of the cell depends on maintaining an adequate GSH pool. NAC bypasses the rate-limiting step of GSH synthesis by directly providing cysteine for gamma-glutamylcysteine synthetase, driving GSH production even under conditions of cysteine depletion. R
Genetics
OGG1: Ser326Cys (rs1052133)
OGG1 encodes 8-oxoguanine DNA glycosylase 1, located on chromosome 3p26. R
The most studied functional polymorphism is rs1052133, a C/G substitution at position 1245 bp in exon 7 that causes an amino acid change from serine to cysteine at codon 326 (Ser326Cys).
The Cys326 variant has lower enzymatic activity for 8-oxoG recognition and excision than the Ser326 wild type. R
A large meta-analysis of 152 case-control studies found significant associations between OGG1 Ser326Cys polymorphism and overall cancer susceptibility in multiple genetic models. R
In stratified analysis by cancer type, significantly increased risk was observed in digestive system cancer, head and neck cancer, lung cancer, and gynecologic cancers. R
A meta-analysis of 27 studies found significant association between the Cys/Cys genotype and lung adenocarcinoma risk. R
For colorectal cancer specifically, results are contradictory across studies, with some meta-analyses finding a significant association in Caucasian populations and others finding no overall association when all ethnic groups are pooled. R
The Ser326Cys finding is therefore a MAYBE for many individual cancer types and a modest but real signal for overall cancer susceptibility in aggregate.
rs1052133 Ser326Cys: Cys/Cys homozygotes have reduced OGG1 repair capacity and modestly elevated risk for lung adenocarcinoma and digestive cancers; Ser/Ser wild type has highest repair capacity. R
MUTYH: Gln324His (rs3219489) And Pathogenic Variants
MUTYH encodes the adenine glycosylase that corrects 8-oxoG:A mispairs.
The common polymorphism Gln324His (rs3219489) is associated with increased colorectal cancer risk (odds ratio approximately 1.42 in case-control studies). R
Biallelic loss-of-function mutations in MUTYH cause MUTYH-associated polyposis (MAP), an autosomal recessive condition characterized by multiple colorectal adenomas and substantially elevated colorectal cancer risk due to unrepaired G:C to T:A transversions in APC. R
MAP is one of the clearest human genetic demonstrations that impaired 8-oxoG repair directly drives carcinogenesis.
XRCC1: Arg399Gln (rs25487)
XRCC1 (X-ray repair cross-complementing protein 1) is a scaffold protein critical for BER efficiency.
The Arg399Gln variant is associated with elevated 8-oxoG levels in leukocytes and significantly increased colorectal cancer risk (odds ratio approximately 2.48 in case-control studies). R
The XRCC1 Arg399Gln finding is one of the strongest BER-related cancer risk associations, stronger than OGG1 Ser326Cys in the studies that measured both. R
More Research
- Guanine oxidation accumulates preferentially at G-rich regulatory sequences in the genome rather than distributing randomly across all guanines, meaning 8-oxoG may function as an epigenetic switch that alters inflammatory gene expression in response to oxidative stress, independent of its mutagenic potential. R
- The normal range for urinary 8-OHdG is significantly different between males and females (females ~44 ng/mg creatinine vs. males ~30 ng/mg creatinine), which has been attributed to hormonal differences in estrogen-related ROS production and antioxidant capacity. R Sex-specific reference ranges are therefore necessary for clinical interpretation.
- Urinary 8-OHdG shows circadian rhythm with day-night variation, meaning single-timepoint measurements may systematically overestimate or underestimate 24-hour damage rates depending on collection timing; 24-hour pooled collections or consistent morning first-void collections improve reliability for longitudinal monitoring. R
- OGG1 expression increases in many tumor types compared with adjacent normal tissue, which at first seems paradoxical but reflects the cancer cell's adaptive strategy to survive its own elevated ROS production by upregulating repair capacity. R Targeting this adaptive OGG1 upregulation as an anti-cancer strategy is an active research area.
- MAP (MUTYH-associated polyposis) is inherited in an autosomal recessive pattern: heterozygous carriers have only mildly elevated cancer risk, but biallelic carriers develop 10 to hundreds of colorectal adenomas starting in the third and fourth decade, with very high colorectal cancer penetrance by age 60. Genetic testing for MUTYH is recommended for anyone with multiple adenomas without an identified dominant polyposis gene (APC mutation).
For biomarker testing I use the Cellular Zoomer and Nutrient Zoomer to contextualize oxidative DNA damage alongside mitochondrial function and antioxidant micronutrient status.
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Quercetin
500mg 2x/day
SPM Active (Pro-resolving Mediators)
2 softgels/day
Curcumin (Liposomal)
500mg 2x/day