CJC-1295 And Ipamorelin: How The GHRH And Ghrelin Peptide Stack Works, DAC vs No-DAC, And The Honest Evidence
By Jacob Gordon, INHC, FMT-CCJC-1295 and Ipamorelin are two research peptides stacked to raise your own growth hormone, and the marketing around them runs well ahead of the human evidence.
In this post, we will discuss what each peptide is, how a GHRH analog and a ghrelin mimetic create a synergistic growth hormone pulse, the difference between the DAC and no-DAC versions of CJC-1295, honest dosing and safety, and the genetics that shape who responds.

What CJC-1295 And Ipamorelin Are
CJC-1295 is a synthetic analog of Growth Hormone Releasing Hormone (GHRH), the hypothalamic peptide that tells the pituitary to release growth hormone.
It is built on the first 29 amino acids of GHRH, called GRF 1-29, which is the shortest fragment that keeps full biological activity.
Four amino acid substitutions protect the molecule from dipeptidyl peptidase-4 (DPP-4), the enzyme that degrades native GHRH within a few minutes.
In healthy adults, single subcutaneous doses of CJC-1295 produced a 2 to 10-fold rise in growth hormone lasting six days or more, and a 1.5 to 3-fold rise in insulin-like growth factor 1 (IGF-1) that stayed elevated for 9 to 11 days. R
Ipamorelin is a pentapeptide (Aib-His-D-2-Nal-D-Phe-Lys-NH2) that mimics ghrelin, the gut hormone discovered in 1999 as the natural ligand for the growth hormone secretagogue receptor. R
It is a Growth Hormone Secretagogue Receptor (GHS-R) agonist, which is a separate receptor from the one GHRH uses.
Ipamorelin was the first compound in its class to release growth hormone without meaningfully raising adrenocorticotropic hormone, cortisol, or prolactin, unlike the older secretagogues GHRP-6 and GHRP-2. R
That selectivity is the entire reason it is preferred over GHRP-2 and GHRP-6, since a peptide that spikes cortisol and prolactin every time you dose it is a poor long-term tool.

Both peptides work upstream of the pituitary, so they raise your own pulsatile growth hormone rather than replacing it with injected recombinant hormone.
How They Work Together
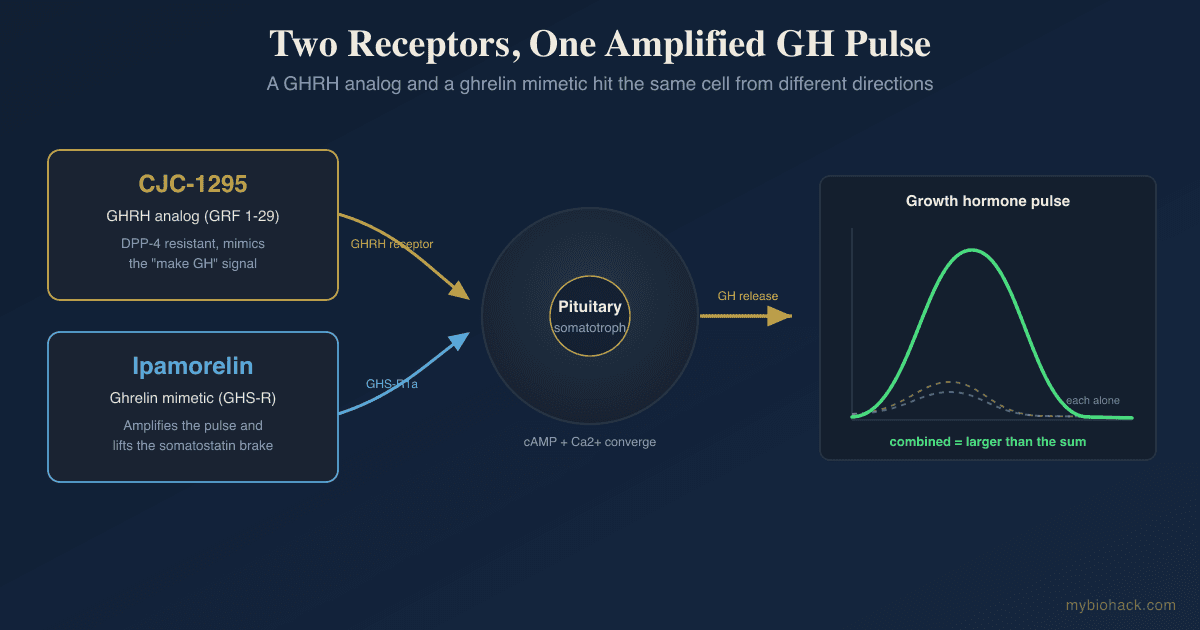
The stack works because GHRH and ghrelin act on two different receptors through two different intracellular pathways.
GHRH binds the GHRH receptor and drives growth hormone synthesis and release.
Ghrelin, and therefore ipamorelin, binds GHS-R1a and amplifies the pulse while blunting somatostatin, the brake on growth hormone. R
Because the two signals converge on the same somatotroph cell from different directions, giving them together produces more growth hormone than the sum of either one alone.
In healthy men, combining a GHRP with GHRH released growth hormone synergistically, and the combination was a more potent and reproducible releaser than either peptide by itself. R
CJC-1295 supplies the GHRH side of that equation and ipamorelin supplies the ghrelin side, which is the pharmacological logic behind the stack.
Here is the honest caveat.
The synergy is well documented for native GHRH plus a growth hormone releasing peptide in acute human dosing studies, but those studies did not use CJC-1295 and ipamorelin specifically, so the exact stack most people buy is an extrapolation from the receptor biology, not a validated combination from a large trial.
Benefits
The claims below range from well supported at the hormone level to almost entirely theoretical at the outcome level, and the difference matters.
1. Higher endogenous growth hormone and IGF-1
This is the one claim with direct human data behind it.
CJC-1295 reliably raises growth hormone and IGF-1 in healthy adults, and ipamorelin raises growth hormone acutely, so the stack does what it says at the level of the blood test. R
Whether a higher IGF-1 number translates into the outcomes people actually want is a separate question.
2. Body composition
The body composition claim is extrapolated from growth hormone physiology, not from trials of these peptides.
The best long-term data on any growth hormone secretagogue comes from MK-677, an oral ghrelin mimetic, which raised IGF-1 into the young-adult range and increased fat-free mass (FFM) by about 1.1 kg over a year in older adults. R
The same trial found no improvement in strength or physical function despite the fat-free mass gain, which is the single most sobering data point for this entire class of compounds. R
Some of the added fat-free mass is intracellular water rather than contractile muscle, which is worth remembering before assuming the scale weight means new tissue.
3. Recovery and connective tissue
Growth hormone and IGF-1 support collagen synthesis and tissue repair, so recovery is a plausible benefit, but there is no controlled trial showing CJC-1295 plus ipamorelin accelerates healing in humans.
If injury recovery is the actual goal, the direct evidence is stronger for BPC-157 and for topical GHK-Cu than for a growth hormone secretagogue.
4. Sleep
Most growth hormone is released during slow-wave sleep (SWS), and GHRH itself promotes slow-wave sleep, so a subjective improvement in deep sleep is one of the more mechanistically reasonable reports.
This too is inference from physiology rather than a sleep endpoint measured in a trial of the stack.
5. Preserved pulsatility versus injected growth hormone
The strongest conceptual argument for this stack over injecting recombinant growth hormone is that it works through your own pituitary and stays under negative feedback control.
That means fewer of the sustained supraphysiologic peaks you get from injecting the hormone directly, at least with the no-DAC version dosed as a pulse.
It is a mechanistic advantage, not an outcome that has been proven to reduce side effects in a head-to-head study.
DAC vs No-DAC
CJC-1295 comes in two forms, and the choice between them changes the whole character of the compound.
The DAC version carries a Drug Affinity Complex (DAC), a chemical group that binds covalently to albumin in the blood and drags the half-life out to roughly 5.8 to 8.1 days. R
That long half-life is convenient, since it can be dosed once or twice a week, but it produces a continuous low-grade elevation of growth hormone often called a "GH bleed."
A continuous elevation flattens the natural pulsatile pattern, and growth hormone is normally released in sharp bursts followed by troughs, so the DAC version trades physiological rhythm for convenience.

The no-DAC version, sold as Mod GRF 1-29 or tetrasubstituted GRF 1-29, has a half-life of only about 30 minutes because it lacks the albumin anchor.
The four substitutions that resist DPP-4 are what let even this short peptide survive long enough to trigger a clean pulse.
No-DAC is therefore dosed alongside ipamorelin at each administration, so the pair fires a discrete growth hormone pulse that rises and falls the way an endogenous pulse would.
The practical trade-off is simple.
DAC means fewer injections and a flatter, more drug-like exposure, while no-DAC means more frequent injections and a more physiological pulse.
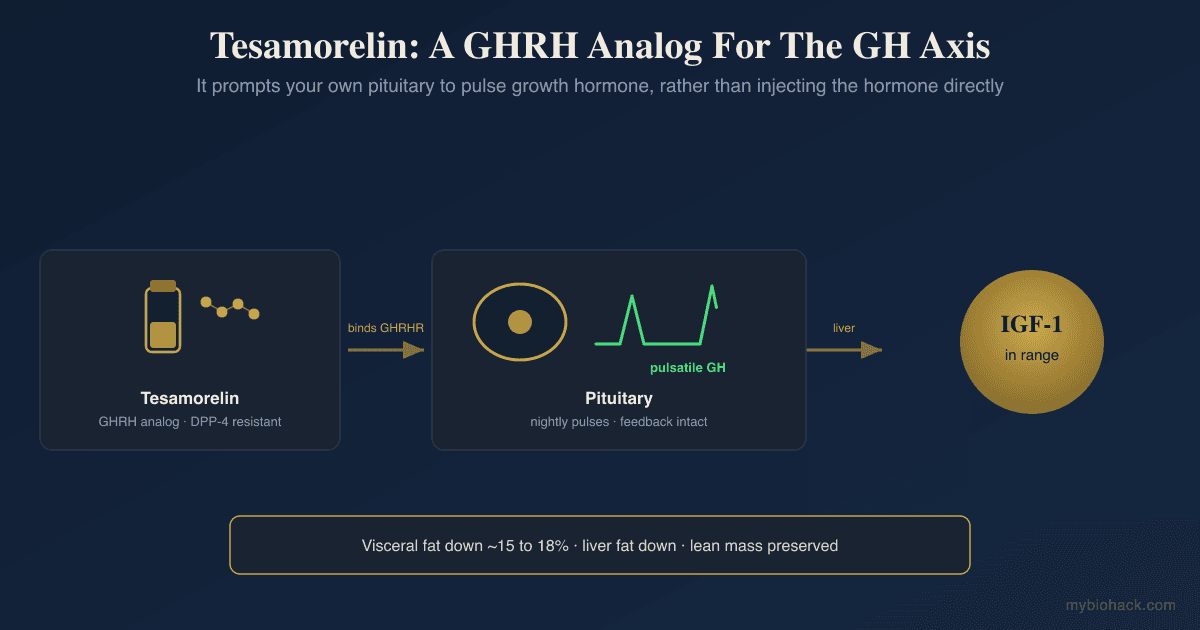
For readers who want an approved GHRH analog with real regulatory review rather than a research chemical, tesamorelin is the FDA-approved member of this family, studied specifically for visceral fat.
Dosing And Safety
This section is descriptive, not a protocol, because CJC-1295 and ipamorelin are not FDA-approved drugs.
They are sold as research chemicals in a legal gray zone, which means purity, sterility, and actual peptide content vary by source and are frequently not what the label claims.
There are no large human randomized controlled trials of the stack, and the human safety record rests on a small number of short studies.
The most rigorous human trial of ipamorelin tested it for postoperative ileus after bowel surgery, missed its primary endpoint, and was discontinued for insufficient efficacy, though it was well tolerated over the short term. R
Community protocols for the no-DAC combination typically report dosing ipamorelin and Mod GRF 1-29 together before bed or after training, timed to an empty stomach so that food-driven insulin and somatostatin do not blunt the pulse.
The predictable side effects are the same ones seen whenever growth hormone and IGF-1 are pushed up.
- Fluid retention, including puffiness, joint stiffness, and carpal tunnel type paresthesias, which track with the degree of growth hormone elevation and are more common in older, heavier, and female users. R
- Insulin resistance and a small rise in fasting glucose and HbA1c, documented directly for the secretagogue MK-677, which reduced insulin sensitivity over 12 months. R
- Sustained IGF-1 elevation, which is the safety signal that deserves the most respect for reasons covered below.
Higher circulating IGF-1 is associated with higher risk of several cancers in large prospective cohorts, with a clear signal for prostate cancer and smaller but consistent associations for breast and colorectal cancer. R R
That is an association from population data, not proof that a peptide protocol causes cancer, but deliberately driving IGF-1 upward for cosmetic or performance reasons is not a decision to make casually, and an active or recent cancer is a hard contraindication.
If someone does use these peptides, the markers that matter are IGF-1 and the metabolic panel, not how they feel.
I use the Insulin Resistance Panel (Quest) to catch the rise in fasting insulin and HOMA-IR before it shows up as elevated glucose, and the Foundation Zoomer (Vibrant Wellness) to track fasting glucose, HbA1c, and liver markers across a cycle.
For readers who want the longevity side of this trade-off, raising IGF-1 is one of the clearest examples of the growth versus lifespan tension covered in the post on IGF-1, Humanin, and longevity.
Mechanisms Of Action
Simple:
- CJC-1295 acts like the body's own signal to make growth hormone, and ipamorelin acts like the body's hunger hormone that tells the pituitary to release it, so together they push a bigger, cleaner burst of your own growth hormone.
- Because they hit two different switches on the same cell, the effect is larger than either one alone, and because your pituitary is still in charge, the release stays closer to a natural pulse than injecting growth hormone directly.
Advanced:
- GHRH receptor signaling. CJC-1295 binds the GHRH receptor, a Gs-coupled G-protein-coupled receptor on pituitary somatotrophs, raising cAMP and activating protein kinase A, which drives both growth hormone gene transcription through CREB and the release of stored growth hormone. The four amino acid substitutions on GRF 1-29 block cleavage by DPP-4, extending the signal from minutes to a usable window. R
- GHS-R1a signaling and somatostatin withdrawal. Ipamorelin activates GHS-R1a, a Gq/11-coupled receptor, triggering phospholipase C, IP3, and a rise in intracellular calcium that amplifies growth hormone release, while ghrelin-pathway activation also opposes somatostatin, the tonic inhibitor of the somatotroph. This dual action, amplifying the releasing signal while lifting the brake, is why ghrelin-pathway agonists amplify pulsatile growth hormone secretion so strongly. R
- Receptor independence and synergy. Because the GHRH receptor and GHS-R1a use distinct G proteins and second messengers, their combined stimulation is supra-additive rather than redundant, which is the receptor-level basis for the clinically observed synergy of GHRH plus a growth hormone releasing peptide. R
- The DAC albumin anchor. The Drug Affinity Complex on the DAC version is a maleimido group that forms a covalent bond with a cysteine on circulating albumin, converting a short peptide into a long-lived depot with a multi-day half-life and a sustained, non-pulsatile pattern of growth hormone exposure. R
Genetics
GHRHR
GHRHR encodes the receptor that CJC-1295 targets on the pituitary.
Biallelic loss-of-function mutations in GHRHR cause isolated growth hormone deficiency type IB, with low but detectable growth hormone and short stature, and more than twenty such mutations have been described. R
The practical point is that a GHRH analog can only work as well as the receptor it binds, so impaired GHRHR signaling blunts the response to CJC-1295.
GHSR
GHSR encodes GHS-R1a, the ghrelin receptor that ipamorelin targets.
A missense mutation that selectively removes the receptor's constitutive activity, while sparing its response to ghrelin, causes familial short stature, which shows how much baseline growth hormone tone depends on this receptor even between meals. R
Other inactivating GHSR variants have been found in children with constitutional delay of growth and puberty, another sign that reduced ghrelin-receptor signaling lowers the growth hormone axis set point. R
Someone carrying a low-activity GHSR variant may get a smaller pulse from a ghrelin mimetic than the population average.
IGF1
IGF1 encodes the downstream effector that carries out most of growth hormone's actions and provides the negative feedback that limits the axis.
A cytosine-adenine repeat polymorphism in the IGF1 promoter sets your baseline IGF-1, and the common 192 base-pair allele, with 19 repeats, is associated with higher circulating IGF-1 and greater adult height. R
The same functional polymorphism has been linked to metabolic and cardiovascular risk, a reminder that your genetically set IGF-1 tone already shapes both the benefit and the risk before any peptide is added. R
More Research
CJC-1295 human data comes down to a single pharmacokinetic and pharmacodynamic study showing it raises growth hormone and IGF-1, with no body-composition or performance endpoints ever measured in a controlled trial. R
For biomarker tracking on a cycle I use the Insulin Resistance Panel (Quest) and the Foundation Zoomer (Vibrant Wellness), and readers who want IGF-1 and these markers charted over time can track them in the Health Hub with a Pro membership.
Ipamorelin's human record is essentially one phase 2 trial for postoperative ileus that missed its endpoint, so almost every efficacy claim for the stack is extrapolated from general growth hormone physiology rather than measured in people using these peptides. R
MK-677 remains the honesty check for the whole class, because it is the one secretagogue studied for a full year, and it raised IGF-1 and fat-free mass but produced no gain in strength or function and worsened insulin sensitivity. R
Regulatory status matters here, since CJC-1295 and ipamorelin are not approved drugs and the approved GHRH analog in this family is tesamorelin, which was actually run through trials for visceral fat.
Sourcing is a real safety variable that no study can control for, because research-chemical peptides vary in purity and content, and a bad vial is its own risk independent of the pharmacology.
Stacking questions come up constantly, and readers exploring peptides for recovery or immune support should see the posts on BPC-157, GHK-Cu, the thymosin peptides, and Thymosin Alpha-1, which target different mechanisms than the growth hormone axis.
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Ashwagandha (KSM-66)
600mg/day
Vitamin D3 + K2
5000 IU + 200mcg/day
Zinc
30mg/day with food