7 Benefits Of Tesamorelin: The GHRH Peptide For Visceral Fat, Liver Fat, And The IGF-1 Axis
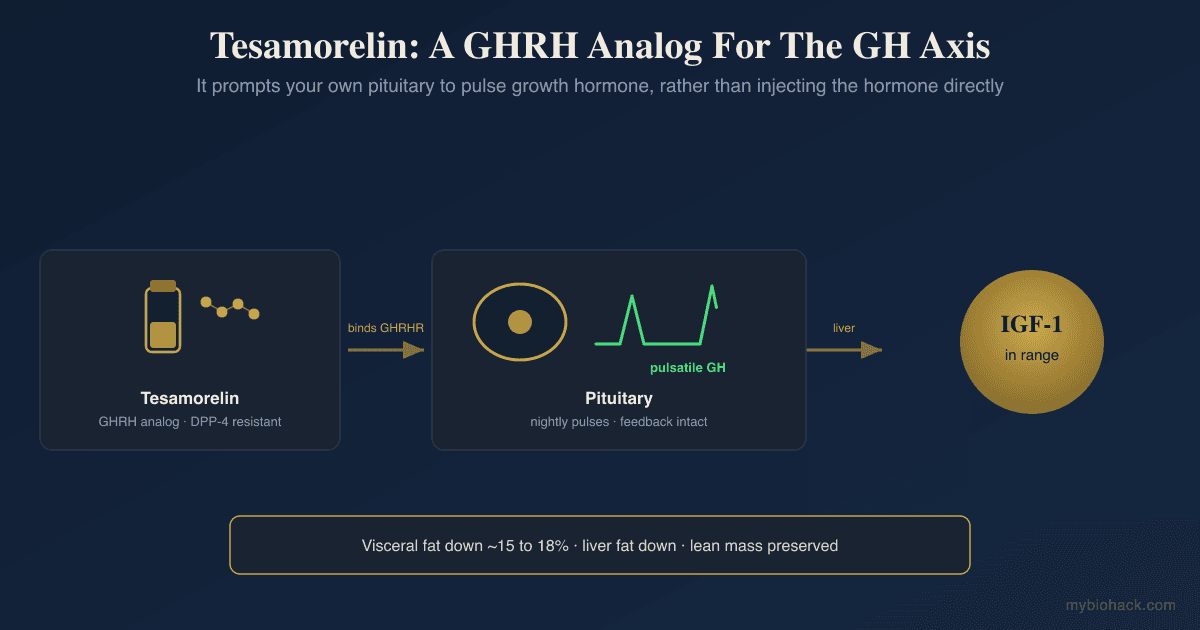
By Jacob Gordon, INHC, FMT-CTesamorelin is a stabilized growth hormone-releasing hormone analog that strips deep abdominal fat by coaxing your own pituitary to release growth hormone in natural pulses, rather than injecting the hormone directly.
In this post, we will discuss what tesamorelin is, its seven best-documented benefits, how it is dosed, its real risks around glucose and IGF-1, the mechanisms behind its effects, the genetics of the growth hormone axis, and the research that is still open.

What Is Tesamorelin
Tesamorelin is a synthetic 44-amino-acid analog of human growth hormone-releasing hormone (GHRH), the hypothalamic peptide that tells the pituitary to release growth hormone.
Native GHRH is destroyed within minutes by the enzyme dipeptidyl peptidase-4, so it is useless as a drug on its own.
Tesamorelin solves this by adding a stabilizing trans-3-hexenoyl group to the N-terminus, which blocks that enzymatic clipping and extends the half-life enough to produce a real physiologic effect. R
It is the only GHRH analog with full FDA approval, sold as Egrifta and Egrifta SV, and it was approved in 2010 to reduce excess visceral adipose tissue (VAT) in people with HIV-associated lipodystrophy. R
The important distinction is that tesamorelin is a secretagogue, not a hormone.
It does not replace growth hormone (GH) the way injected recombinant HGH (somatropin) does.
Instead it stimulates the somatotroph cells of the pituitary to make and release your own GH in the same pulsatile rhythm the body uses naturally, which preserves the feedback loops that keep the axis in a physiologic range. R
Most of the human evidence comes from people with HIV, because that is the population it was developed and approved for.
The mechanisms are not HIV-specific, so the metabolic and cognitive findings are broadly informative, but extrapolating them to healthy biohackers is inference rather than proven fact, and that caveat runs through the entire post.
7 Benefits Of Tesamorelin
1. It Selectively Strips Visceral Fat
This is the effect tesamorelin is built around, and it is the best-documented one.
In the pivotal 26-week randomized, double-blind, placebo-controlled phase 3 trial of 412 patients, tesamorelin reduced visceral adipose tissue by roughly 15 percent while the placebo group gained fat. R
Pooled phase 3 data showed VAT falling by approximately 18 percent in continuing responders, and a 2026 meta-analysis of randomized controlled trials confirmed a significant, selective loss of visceral fat and a gain in lean mass. R R
The key word is selective.
Tesamorelin preferentially targets the metabolically dangerous fat packed around the organs and largely spares subcutaneous fat, which is why body mass index barely moves even as visceral fat drops. R
2. It Reduces Liver Fat And Slows Fibrosis
Visceral fat and a fatty liver travel together, so it follows that tesamorelin also acts on Non-Alcoholic Fatty Liver Disease (NAFLD).
In a 12-month randomized, double-blind trial in people with HIV and NAFLD, tesamorelin cut the hepatic fat fraction (HFF) by 37 percent relative to placebo. R
Thirty-five percent of the tesamorelin group brought their liver fat below the 5 percent steatosis threshold, versus 4 percent on placebo. R
More striking, only 10.5 percent of tesamorelin-treated participants showed fibrosis progression over the year, compared with 37.5 percent on placebo, which suggests the peptide does more than shift fat and may blunt the scarring process itself. R

An earlier 6-month trial had already found modest liver-fat reductions alongside the visceral-fat effect, so the liver signal has now replicated. R
If you are working through fatty liver, the mechanistic background sits in the post on NAFLD, NASH, and chronic liver disease.
3. It Preserves Your Own Pulsatile GH Rhythm
Growth hormone is not meant to sit at a steady high level.
The body releases it in sharp pulses, mostly at night, and that pulsatility is part of the signal.
Injected recombinant HGH flattens this into a sustained, supraphysiologic plateau, which is a large part of why exogenous GH carries more metabolic baggage.
Because tesamorelin works one step upstream at the pituitary, it amplifies the natural pulses instead of overriding them, and a controlled study in healthy men confirmed it preserves pulsatile GH architecture while leaving insulin sensitivity intact. R

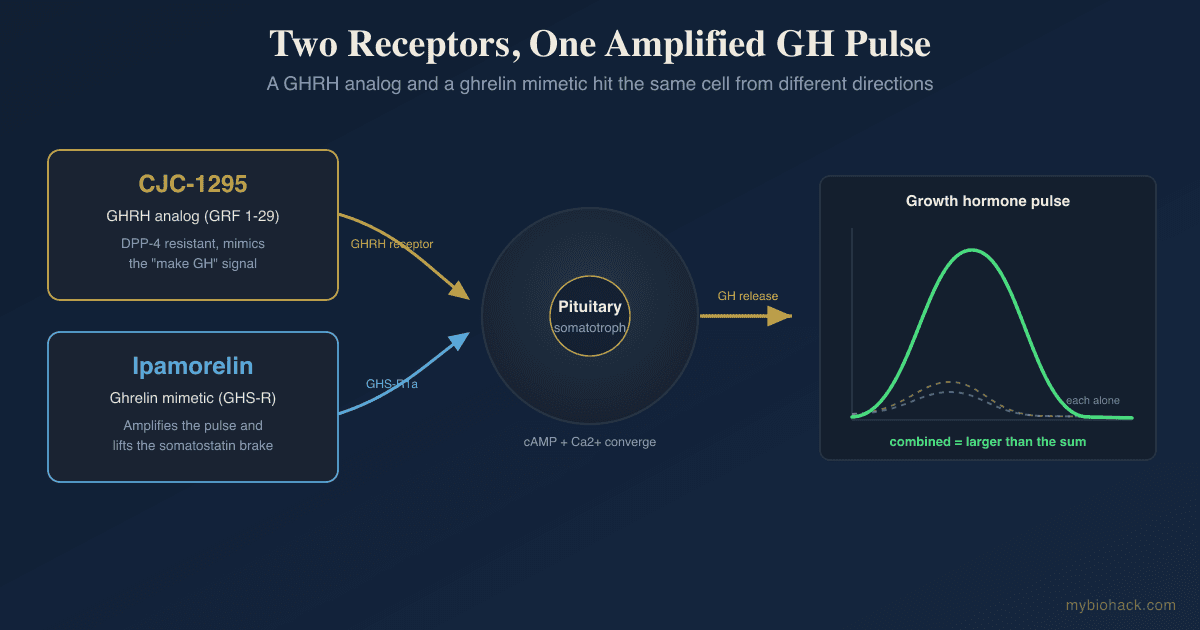
This is the mechanistic argument for choosing a GHRH analog over direct HGH, and it is the same logic behind stacked GH secretagogues like CJC-1295 and ipamorelin.
4. It Raises IGF-1 While Keeping It In The Physiologic Range
Downstream of GH, the liver produces insulin-like growth factor 1 (IGF-1), the anabolic mediator responsible for much of what GH accomplishes in muscle and brain.
Tesamorelin reliably raises IGF-1.
In the cognition trial, IGF-1 rose 117 percent from baseline yet stayed within the normal physiologic range, because the intact feedback loop through somatostatin and IGF-1 itself caps how high the axis can climb. R
That ceiling is the whole point.
Raising IGF-1 is a benefit for body composition and tissue repair, but IGF-1 is also a growth signal, so keeping it inside the physiologic band rather than pushing it into supraphysiologic territory is what separates a GHRH analog from a blunt IGF-1 or HGH protocol.
For the full picture of the IGF-1 axis, its role in longevity, and why context decides whether it helps or harms, see the post on humanin, IGF-1, and mitochondrial signaling.
5. It Improves The Lipid Profile
The metabolic benefits extend to blood lipids.
Across the phase 3 program, tesamorelin lowered triglycerides and improved the ratio of total to HDL cholesterol, tracking the reduction in visceral fat. R
The 2026 meta-analysis confirmed favorable shifts in the lipid panel without a meaningful adverse effect on glucose in the pooled short-term data. R
This is consistent with the idea that much of the harm from visceral fat runs through the lipids and inflammatory signals it exports, so removing the depot improves the downstream markers.
6. It Improves Muscle Quality And Lean Area
Tesamorelin is not a bulking agent, but it does improve the quality of muscle.
In a subgroup of clinically meaningful responders, tesamorelin increased the density of all four measured trunk muscle groups, meaning less fat infiltrating the muscle, and increased lean muscle cross-sectional area. R
Reduced intramuscular fat and higher muscle density matter for insulin sensitivity and function, not just appearance.
This makes tesamorelin conceptually interesting as an adjunct where muscle is under threat, such as the muscle loss that can accompany aggressive GLP-1 use, a problem covered in the post on preserving muscle on GLP-1 drugs.
7. It Supports Executive Function And Memory In Aging Brains
The most surprising benefit is neurological.
In a 20-week randomized, double-blind, placebo-controlled trial of 152 older adults, including 66 with mild cognitive impairment (MCI), 1 mg of tesamorelin per day produced a favorable effect on executive function (P = 0.005) and a trend toward better verbal memory (P = 0.08). R
Healthy adults improved and the expected decline in the MCI group was attenuated. R
A companion analysis found the peptide raised brain gamma-aminobutyric acid levels, and the GABA change correlated with the cognitive gains, offering a plausible neurochemical route. R
This is a single, well-run study rather than a settled body of evidence, so it should be read as a promising signal, not a reason to treat tesamorelin as a nootropic.
How It Is Used And Dosing
Tesamorelin is injection-only.
There is no oral, sublingual, or transdermal form that survives digestion, so anyone claiming otherwise is selling something that does not work.
The FDA-approved dose for visceral fat is 2 mg injected subcutaneously once daily, rotating sites around the abdomen. R
The cognition trial used a lower 1 mg daily dose given about 30 minutes before bedtime, which mirrors the body's nocturnal GH pulse. R
Timing at night is deliberate, because that is when the largest natural GH pulse occurs and when the pituitary is most responsive.
Effects on visceral fat are measurable by around three months and approach their maximum near six months. R
The effect is maintenance-dependent.
When tesamorelin is stopped, visceral fat tends to return, so it behaves like a chronic metabolic therapy rather than a one-time correction. R
Because it moves the GH and IGF-1 axis, it should be run with objective bloodwork rather than by feel.
A prescriber orders a baseline and 26-week IGF-1 level, and the FDA label directs discontinuation if the IGF-1 standard deviation score climbs above 2. R
For the metabolic side, I track fasting glucose, insulin, and metabolic markers with the Cardio Zoomer (Vibrant Wellness) and liver enzymes such as AST, ALT, and GGT with the Foundation Zoomer (Vibrant Wellness) before starting and periodically on treatment.
Tracking those trends over months, rather than reading a single draw, is exactly the kind of longitudinal data the Health Hub is built to hold.
Safety, Risks, And The FDA Compounding Context
Tesamorelin is generally well tolerated, but it is not casual, and the honest risks matter more than the marketing.
Contraindications and cautions (not an exclusive list):
- Active malignancy (the axis it stimulates is a growth axis, and the label bars use in active cancer) R
- Disrupted hypothalamic-pituitary axis (pituitary tumor, hypophysectomy, or head irradiation)
- Fluid retention, joint pain, and injection-site reactions (the most common on-treatment complaints) R
- Pregnancy (not appropriate)
The two risks worth sitting with are glucose and IGF-1.
On glucose, tesamorelin was broadly neutral in the pooled short-term trials, but the FDA label still carries a warning, because in phase 3 the proportion of patients crossing into an HbA1c of 6.5 percent or higher was 4.5 percent on tesamorelin versus 1.3 percent on placebo. R
The mechanism is real: growth hormone is counter-regulatory to insulin, so a minority of users can drift toward glucose intolerance, and anyone with existing insulin resistance should watch this closely.
On IGF-1, the same growth signal that repairs tissue also feeds tumors.
Large prospective epidemiology links higher circulating IGF-1 to a modestly increased risk of prostate, breast, and colorectal cancer, with men in the highest fifth of IGF-1 carrying about a 29 percent higher prostate cancer risk than the lowest fifth. R
There is a big MAYBE here.
Tesamorelin trials did not show an increase in cancer, and the peptide keeps IGF-1 within the physiologic range rather than driving it supraphysiologic, which is reassuring.
But those trials were not long enough or large enough to rule out a small long-term signal, so the epidemiology is a reason for genuine caution, not a settled all-clear.
The regulatory picture is also in flux.
The branded product (Egrifta) remains FDA-approved and unaffected, but in April 2026 the FDA removed 12 peptide bulk drug substances, tesamorelin among them, from Category 2 of its interim Section 503A bulk-substances list after the nominations were withdrawn, moving them into limbo pending review by the Pharmacy Compounding Advisory Committee.
Removal from Category 2 is not an approval for compounding pharmacies, and people relying on compounded tesamorelin may see supply and legality shift as that review plays out, so source and regulatory status are worth confirming before starting.
If you are weighing a GH-axis peptide against your own labs and history, this is a reasonable topic for a consult rather than a self-guided experiment, and you can book one at /contact.
Mechanisms Of Action
Simple:
- Tesamorelin tells your pituitary to release your own growth hormone in natural nightly pulses, and that growth hormone, together with the IGF-1 it triggers in the liver, signals deep belly fat and liver fat to break down while sparing muscle.
Advanced:
- GHRH receptor agonism. Tesamorelin binds the GHRH receptor on pituitary somatotrophs, a G-protein-coupled receptor that raises intracellular cyclic AMP and activates protein kinase A, driving synthesis and pulsatile release of GH while leaving somatostatin and IGF-1 negative feedback intact, which is why the pulse pattern and physiologic ceiling are preserved. R
- Preferential visceral lipolysis. GH acts on visceral adipocytes to activate hormone-sensitive lipase and suppress lipoprotein lipase, favoring lipid mobilization from the visceral depot specifically, which explains the selective loss of VAT with relative sparing of subcutaneous fat. R
- Hepatic gene reprogramming. In paired liver biopsies, tesamorelin raised expression of oxidative-phosphorylation gene sets and lowered gene sets governing inflammation, tissue repair, and cell division, and those shifts tracked with an improved fibrosis-gene score, while de novo lipogenesis (DNL) genes were not clearly changed in the fasting-state biopsies. R
- Central IGF-1 and GABA signaling. GH and IGF-1 cross the blood-brain barrier, and IGF-1 is neurotrophic, but the cognition study specifically linked tesamorelin to higher brain GABA levels that correlated with executive-function gains, pointing to a neurochemical mechanism beyond simple IGF-1 elevation. R
- Enzymatic stabilization. The trans-3-hexenoyl modification on the N-terminal tyrosine blocks dipeptidyl peptidase-4 cleavage, extending the functional half-life of the GHRH(1-44) sequence enough to produce sustained daily pituitary stimulation. R
Genetics
The genes that decide how strongly anyone responds to a GHRH analog sit along the GH and IGF-1 axis.
GHRHR
The growth hormone-releasing hormone receptor (GHRHR) gene encodes the pituitary receptor that tesamorelin actually binds.
Inactivating mutations in GHRHR cause isolated growth hormone deficiency and short stature, and even heterozygous carriers of a null GHRHR mutation end up shorter than normal in later life, when the GH and IGF-1 axis is already running sub-maximally. R
These are rare loss-of-function mutations rather than a single common SNP, but they make the point cleanly: a person with reduced GHRHR signaling has fewer functional receptors for tesamorelin to work through, which is a plausible source of the responder versus non-responder split seen in the trials.
IGF1
The IGF1 gene encodes insulin-like growth factor 1, the mediator that carries out most of tesamorelin's downstream effects.
A cytosine-adenine microsatellite repeat in the IGF1 promoter influences circulating IGF-1, with the common 192-base-pair (19-repeat) allele associated with differences in IGF-1 level and body height, though the literature is genuinely mixed on the direction. R
The same promoter variation has been tied to IGF-1-related cancer risk in some cohorts, which is the genetic echo of the epidemiologic caution above and a reason people with a strong family history of hormone-sensitive cancers should be especially deliberate about raising IGF-1. R
More Research
Cognition mechanism is still preliminary, resting on one 20-week trial and a linked GABA analysis, so the executive-function benefit is a promising signal rather than an established indication. R R
General-population data are thin, because nearly all controlled evidence comes from people with HIV-associated fat accumulation, and applying it to otherwise healthy adults is a reasonable inference that has not been directly tested at scale. R
Muscle-quality gains were seen in a responder subgroup rather than every participant, so the effect on muscle density and area is real but conditional on a meaningful visceral-fat response. R
NASH histology was not the endpoint of the liver trial, which was powered for fat fraction and fibrosis-progression signals, so tesamorelin reducing liver fat and slowing fibrosis is well supported while formal reversal of established NASH is not yet proven. R
Weight regain after discontinuation means the visceral-fat benefit is maintenance-dependent, and the durability of any metabolic or cognitive gain once the peptide is stopped has not been characterized. R
For biomarker tracking on any GH-axis protocol, I track IGF-1, fasting insulin, and liver enzymes over time in the Health Hub, and it is those trends, not a single blood draw, that tell you whether the risk-benefit is actually landing in your favor.
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Ashwagandha (KSM-66)
600mg/day
Vitamin D3 + K2
5000 IU + 200mcg/day
Zinc
30mg/day with food