Coregulation And Attachment Style: How Your Early Nervous System Wiring Shapes Your Biology
By Jacob Gordon, INHC, FMT-CThis article contains affiliate links. As an Amazon Associate, MyBioHack earns from qualifying purchases at no extra cost to you. We only link products we research and stand behind.
Attachment style is the pattern of relating to others that forms in early childhood based on how reliably caregivers responded to distress, and it is not simply a psychological preference but a physiological set-point that determines how efficiently your autonomic nervous system coregulates with other people's.
In this post, we will discuss what the four attachment styles are, how each one maps onto a measurable physiological signature (HRV, cortisol, electrodermal activity), why coregulation succeeds or fails differently across attachment patterns, what the epigenetic and genetic mechanisms are, what you can do to shift your regulatory capacity, and what the current evidence says about changing attachment style in adulthood.

Basics Of Attachment Theory
Attachment theory, developed by John Bowlby and empirically mapped by Mary Ainsworth, proposes that infants are biologically prepared to form a strong bond to a primary caregiver because that bond is their survival system. R
The attachment system activates whenever the infant experiences threat, pain, or uncertainty.
The caregiving response (or its absence) shapes whether social proximity becomes associated with safety or with further threat. R
From this early patterning, three organized attachment strategies and one disorganized pattern emerge:
Secure attachment (low anxiety, low avoidance)
The caregiver responds consistently and appropriately to the infant's distress signals.
Social proximity reliably produces calm.
The infant learns: distress is temporary, others are trustworthy, I am worth helping.
In adulthood: comfortable with intimacy, able to ask for support, recovers from conflict, physiologically flexible under stress. R
Anxious (preoccupied) attachment (high anxiety, low avoidance)
The caregiver responds inconsistently, sometimes available and warm, sometimes distracted, dismissive, or overwhelming.
The infant cannot predict when social proximity will produce calm.
The adaptive strategy: maximize attachment signals, never de-escalate, stay hypervigilant for caregiver availability.
In adulthood: preoccupied with relationships, high rumination, persistent distress signaling, hypersensitive to perceived rejection or abandonment. R
Avoidant (dismissing) attachment (low anxiety, high avoidance)
The caregiver consistently rejects or dismisses emotional bids, particularly distress.
The infant learns that expressing need produces rejection, not comfort.
The adaptive strategy: suppress emotional expression, deactivate the attachment system, appear independent.
In adulthood: minimizes reliance on others, uncomfortable with closeness, reports low distress but shows physiological stress markers that contradict self-report. R
Disorganized (fearful) attachment (high anxiety, high avoidance)
The caregiver is simultaneously the source of safety and the source of threat.
The attachment system activates (because there is fear) but proximity-seeking is blocked (because the proximity source is the threat).
There is no coherent strategy: the system collapses into approach-avoidance oscillation.
In adulthood: volatile relationship dynamics, dissociation under stress, contradictory impulses of wanting closeness and fleeing it. R
A note on measurement:
Attachment has been measured as categorical (Strange Situation procedure in infants, Adult Attachment Interview) and as continuous dimensions (self-report scales measuring anxiety and avoidance).
Both approaches have validity.
The dimensional approach (anxiety and avoidance as two independent axes) is increasingly dominant in adult research because it allows finer-grained physiological correlations. R
How Each Attachment Style Maps To Physiology
This is where attachment theory stops being psychology and starts being biology.
The core finding:
Attachment style functions as a strategy for regulating physiological stress responses.
The hyperactivating strategy of anxious attachment and the deactivating strategy of avoidant attachment each produce distinct, measurable autonomic, endocrine, and neuroimaging signatures. R
Secure Attachment: Physiological Flexibility
Securely attached individuals show the most adaptive autonomic profile.
They respond to stressors with appropriate physiological reactivity, then return to baseline efficiently.
In the Vagal Tank Theory framework, organized (including secure) attachment was associated with a decrease in HRV (measured by RMSSD) from baseline to stress and a return to baseline during recovery, the expected adaptive pattern.
In contrast, unresolved/disorganized attachment showed a paradoxical HRV increase from baseline to stress that remained elevated during recovery, an anomalous and maladaptive pattern. R
Thinking of an attachment figure increases HRV in securely attached or low-avoidance individuals.
The same priming has no effect or opposite effects in high-avoidance individuals. R
Anxious Attachment: Hyperactivated HPA Axis And Elevated Cortisol
Anxious attachment is associated with greater cortisol reactivity to psychosocial stress.
In a study of 78 healthy young women exposed to the Trier Social Stress Test (TSST-G), insecure anxious attachment (high insecurity and proximity-seeking) predicted significantly greater cortisol reactivity than secure attachment, independent of age, smoking, menstrual phase, and BMI. R
In a study of dating couples, anxiously attached women receiving positive partner support during stress showed cortisol levels that remained elevated longer compared to less anxious women receiving equivalent support.
The support itself was not the problem.
The anxious nervous system could not use it. R
Anxious attachment is associated with:
- Elevated self-reported stress and more frequent negative affect R
- Accelerated heart rate during conflict discussions with partners R
- Higher HF-HRV suppression during stress (more physiological reactivity) in children R
- Greater electrodermal reactivity to conflict discussions R
- Increased neuroimaging activity in social threat processing areas (amygdala, right insula) R
The pattern is consistent: the anxious nervous system is chronically primed for threat, amplifies distress signals, and struggles to use social proximity to downregulate once activated.
Avoidant Attachment: Suppressed Subjective Stress, Elevated Autonomic Activity
Avoidant attachment produces the most clinically misleading pattern: low self-reported stress combined with elevated physiological stress markers. R
Attachment avoidance is inversely associated with HF-HRV, a marker of vagal influence on cardiac activity, independent of age and respiratory variability.
Importantly, avoidance predicts reduced HF-HRV but is not associated with subjective stress. R
This is the physiological cost of the deactivating strategy: you suppress the subjective experience of distress, but the body continues to mount a stress response.
Highly avoidant individuals show greater electrodermal reactivity across stressful tasks despite reporting lower distress.
Adults with a deactivating pattern toward their childhood caregiver showed greater electrodermal activity during a conflict discussion with a romantic partner, while concurrently presenting affectively neutral behavior. R
The dismissing attachment style (insecure-avoidant representation) is associated with an emotionally deactivating strategy, while at the physiological, biochemical, and nonverbal levels, emotional stress is still measurably present. R
Avoidant individuals do not relax when they think of an attachment figure.
In low-avoidance individuals, mentally activating an attachment figure produces increased HRV.
In high-avoidance individuals, this effect is absent or reversed. R
In children with chronic medical conditions, heart rate differed significantly across attachment groups (F2,42 = 44.48, P < 0.001).
Anxious children had higher resting heart rates than avoidant children, but avoidant children showed cognitive patterns consistent with sustained sympathetic load. R
Disorganized Attachment: No Coherent Regulatory Strategy
Disorganized attachment lacks a coherent physiological regulatory pattern.
It is associated with heightened stress reactivity, dissociation following trauma, prolonged recovery from stress, rapid emotional fluctuations, and the anomalous HRV patterns described above (increases where decreases are expected, failure to recover). R
At the neural level, disorganized attachment is associated with alterations in oxytocin and cortisol physiology, neurophysiological correlates (EEG, fMRI activation differences), and morphological brain changes in regions involved in emotional regulation. R
How Coregulation Works Differently Across Attachment Styles
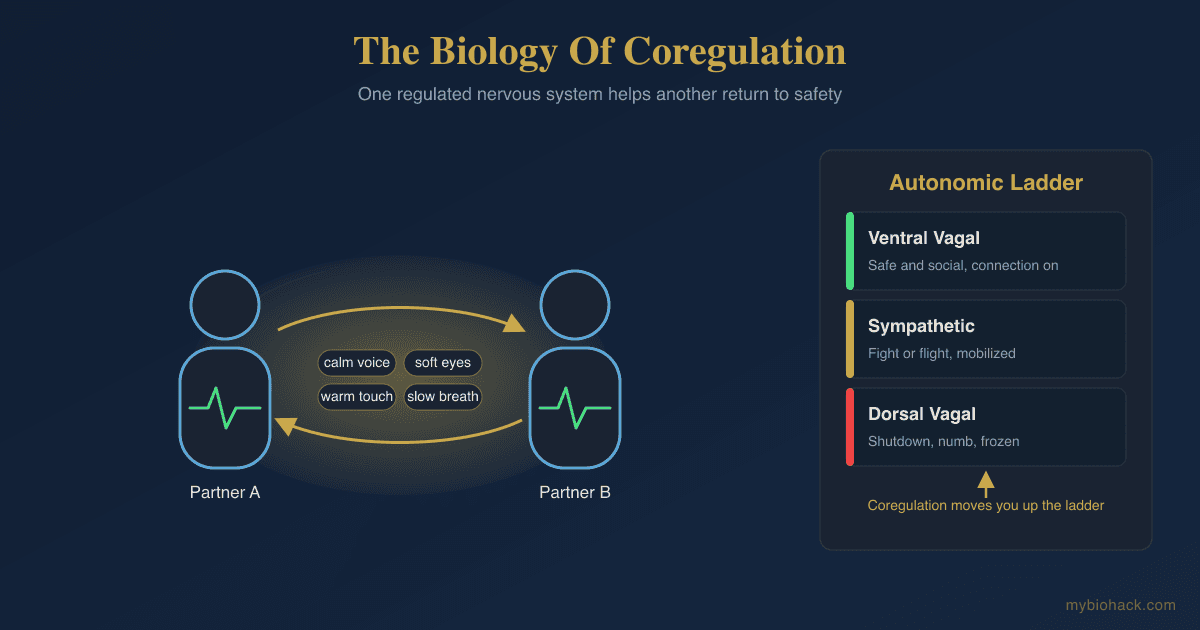
Coregulation is the process by which one nervous system stabilizes another through interpersonal cues of safety: vocal prosody, facial expression, paced breathing, rhythmic touch, and consistent availability. R
Attachment style determines whether coregulation can occur and how.
Secure: coregulation is bidirectional and efficient
Securely attached individuals can both receive and offer coregulation.
They detect cues of safety accurately, use them to downregulate defensive autonomic states, and return to baseline quickly. R
Their partners' physiology reliably influences their own because the social engagement system is accessible.
They can also support others effectively because their own regulatory capacity is not depleted by chronic defensive activation. R
Anxious: coregulation-seeking without coregulation-receiving
The central paradox of anxious attachment is that the person desperately seeks coregulation but cannot actually receive it. R
This is not willfulness.
The anxiously attached nervous system has been calibrated to treat the absence of reassurance as the norm and reassurance itself as potentially temporary or unreliable.
Even when a regulated, warm partner provides clear cues of availability, the anxious nervous system cannot fully process them as resolving threat. R
Physiological coregulation in couples involves the coordination of autonomic state between partners.
Anxiously attached individuals show dependent coregulation: their physiology tracks and amplifies their partner's, rather than moving toward homeostasis.
When the partner is dysregulated, the anxiously attached person becomes more dysregulated.
When the partner is calm, they move toward calm, but more slowly and incompletely than secure individuals. R
Poor physiological coregulation in couples predicts larger increases in negative affect after conflict discussions in both healthy couples and those with personality pathology. R
Avoidant: coregulation blocked at input
The avoidantly attached nervous system has learned to shut down the attachment system rather than activate coregulation through it. R
When an avoidant individual shows heightened autonomic nervous system activity (elevated electrodermal response, reduced HRV), they simultaneously suppress behavioral and subjective expression of that activation.
They appear regulated while being physiologically stressed. R
Avoidantly attached individuals show contrarian coregulation: when their partner is approaching them emotionally or physiologically, they move away.
During conflict discussions, their physiology diverges from their partner's rather than aligning. R
This prevents coregulation from occurring.
The consequence is that avoidant individuals carry their physiological stress load without access to the social buffering that would reduce it.
Over time, this produces the health consequences associated with chronic sympathetic loading without parasympathetic recovery. R
Disorganized: coregulation collapsed
Disorganized attachment produces the most severe coregulation impairment.
Social proximity activates threat (because the attachment figure was also a threat source), so the social engagement system itself becomes conditioned to danger.
Attempts at coregulation by others may trigger either freezing, dissociation, or unpredictable behavioral oscillation between approach and avoidance. R
Causes And Early Developmental Drivers
Attachment style is not fixed at birth.
It is shaped by the early caregiving environment through biological mechanisms that alter gene expression, autonomic set-points, and neural architecture. R
Caregiver sensitivity and consistency
Secure attachment develops when caregivers respond promptly, accurately, and warmly to infant distress signals across the majority of interactions.
Perfect consistency is not required.
"Good enough" caregiving, meaning sufficient reliability that the infant can predict that distress will resolve through social proximity, produces secure attachment. R
Anxious attachment develops with inconsistent caregiving, where the caregiver is sometimes available and sometimes not, producing hyperactivation of attachment signaling as the infant's attempt to maximize the probability of response. R
Avoidant attachment develops with consistently dismissing caregiving, where the caregiver reliably does not respond or responds negatively to emotional bids.
The infant learns to suppress rather than signal. R
Disorganized attachment develops when the caregiver is simultaneously frightening and/or frightened.
Abuse, neglect combined with terror, a caregiver with unresolved trauma who becomes dissociated during caregiving, or a severely depressed parent who becomes unpredictably unavailable: all activate the attachment system (threat) while simultaneously blocking its resolution (caregiver is the threat source). R
NR3C1 epigenetic programming
Maternal sensitivity in infancy significantly predicts lower NR3C1 (glucocorticoid receptor gene) methylation at two CpG loci in children at age 6.
Higher methylation of NR3C1 suppresses glucocorticoid receptor expression, impairing the cortisol negative feedback loop and producing higher HPA axis reactivity. R
Children who experienced less maternal support during stress and who had high NR3C1 methylation developed greater anxious attachment 18 months later than children with low NR3C1 methylation in the same caregiving conditions.
NR3C1 methylation acts as a biological moderator that amplifies the effect of caregiving quality on attachment development. R
Childhood maltreatment correlates significantly with NR3C1 hypermethylation (P = 6.16 × 10-8), with sexual abuse severity and number of abuse types both predicting higher methylation. R
Hippocampal samples from suicide victims with a history of childhood abuse showed increased NR3C1 promoter methylation, decreased glucocorticoid receptor mRNA, and impaired transcription factor binding, compared to suicide victims with no childhood abuse history and controls.
The abuse history, not the suicide per se, drove the epigenetic difference. R
Caregiver transmission
Maternal PTSD and childhood IPV exposure are associated with specific NR3C1 methylation signatures in both mothers and their children, with mother-child methylation levels significantly correlated.
The caregiver's own unresolved trauma transmits to the child not only through behavior but through epigenetic mechanisms that shape the child's stress response system. R
This is intergenerational biology, not just intergenerational psychology.
Overlapping Conditions
Depression And Anxiety Disorders
Insecure attachment (both anxious and avoidant) is a risk factor for depression in adults.
The HRV reductions associated with insecure attachment overlap substantially with the HRV reductions characteristic of anxiety disorders (Hedges' g approximately 0.39 to 0.63 depending on anxiety subtype) and depression. R
Anxious attachment specifically predicts HPA axis hyperreactivity patterns (elevated cortisol reactivity to social stress) that are mechanistically associated with anxiety disorder development. R
Chronic Illness And Immune Dysregulation
Attachment insecurity is associated with dysregulated physiological responses to stress, risky health behaviors, susceptibility to physical illness, and poorer disease outcomes across multiple conditions. R
The vagal tone reduction associated with avoidant attachment withdrawal of the cholinergic anti-inflammatory pathway from peripheral tissues.
Chronically reduced vagal tone removes the braking effect on macrophage cytokine production, contributing to systemic inflammatory load. R
Personality Disorders
Disorganized attachment is specifically and robustly associated with personality, eating, affective, dissociative, and addictive disorders.
The cortisol dysregulation, neurophysiological alterations, and morphological brain changes associated with disorganized attachment overlap with the neurobiological profiles of borderline personality disorder and other cluster B conditions. R
Gut And Somatic Symptom Disorders
The chronically reduced vagal tone of insecure attachment impairs the gut-brain axis, reducing parasympathetic drive to gut motility, mucosa integrity, and the anti-inflammatory vagal reflex to the enteric nervous system.
People with insecure attachment styles show higher rates of functional somatic symptoms and irritable bowel syndrome, partially mediated by these autonomic mechanisms. R
PTSD
Insecure attachment style (adjusted OR = 4.29, P < 0.001) is a significant predictor of probable lifetime PTSD in a nationally representative sample of 2,163 U.S. military veterans.
The interaction of OXTR rs53576 genotype and insecure attachment style further increased PTSD risk: among A allele carriers with insecure attachment, the prevalence of probable PTSD was 23.9% versus 2.0% in A allele carriers with secure attachment (adjusted OR = 10.7). R
Disorganized attachment is the specific subtype most strongly associated with PTSD development after trauma exposure, because the attachment system was already conditioned to threat and the social coregulation pathway that normally provides post-trauma recovery was never reliably available. R
How To Improve Regulatory Capacity And Shift Attachment Patterns
Attachment style is not immutable.
Adult romantic relationships, therapy, and deliberate regulatory practices can all shift it, though this requires sustained experience rather than single interventions. R
The process is fundamentally biological: the nervous system needs repeated experiences of threat-then-resolution through social proximity before its threat-to-proximity association updates.
1. Secure-Base Relationships
The most powerful intervention is a consistently reliable relationship with a regulated person, whether a romantic partner, a therapist, or a close friend who maintains availability without collapsing under the anxious person's distress or withdrawing from the avoidant person's distance. R
This functions as repeated coregulation practice: over hundreds of interactions, the nervous system updates its working model because the expected outcome (non-response, abandonment, threat) does not occur. R
The partner's attachment style matters physiologically.
A partner's dispositional anxiety moderates how the other partner responds to their own baseline anxiety: if partners are high in dispositional anxiety, probands exhibited contrarian coregulation, and if partners are low in anxiety, they exhibited dependent coregulation. R
In practice: the attachment system cannot be updated in isolation.
It was built through relationships and it changes through relationships.
2. Attachment-Informed Psychotherapy
Attachment-informed therapies (including Emotionally Focused Therapy, AEDP, schema therapy, and long-term psychodynamic work) work by establishing the therapeutic relationship itself as a coregulatory secure base through which new working models are developed.
The therapist's consistent availability, regulated state, and accurate attunement to the client's affective states provides the repeated corrective experience that the nervous system requires to update its predictions about social proximity. R
For disorganized attachment specifically, the sequence matters: autonomic stabilization (often via body-based methods) typically needs to precede narrative processing of attachment experiences because the nervous system must first learn that the social engagement system can be safe before it can process why it learned to collapse. R
3. HRV Biofeedback For Physiological Flexibility
HRV biofeedback directly exercises the vagal pathways that are structurally underactive in insecure attachment, particularly in the avoidant pattern where HF-HRV is chronically reduced. R
Slow paced breathing (approximately 5 to 6 breaths per minute) maximally engages the baroreflex and RSA pathway, building vagal tone through repeated activation.
This does not directly change attachment representations, but it increases the physiological substrate available for coregulation.
A more flexible vagal brake means social proximity is more capable of producing calm, which creates more opportunities for the nervous system to associate relationship with relief rather than threat. R
For anxious attachment specifically:
The goal is to increase baseline HRV and reduce the magnitude of cortisol reactivity to social stress, decreasing the nervous system's hair-trigger threat response so that the coregulatory signal from others can actually land. R
For avoidant attachment specifically:
The goal is to increase HF-HRV, which is the most consistently reduced physiological marker in avoidant individuals.
Greater vagal tone makes it physiologically possible to allow proximity to be regulatory rather than activating the defensive deactivation reflex. R
Typical protocol: 20 minutes daily at approximately 5 to 6 breaths per minute, sustained over 6 to 8 weeks. R
4. Somatic Experiencing And Body-Based Work
Somatic Experiencing (SE) addresses the incomplete defensive responses stored in the nervous system from early attachment disruptions.
For individuals with disorganized or anxious attachment, early threat responses are held as unresolved physiological states.
SE works to complete those cycles through tracked sensation rather than narrative, allowing the autonomic state to shift without requiring verbal processing of experiences that may not have been stored verbally. R
5. Targeted Mindfulness And Interoception Training
Mindfulness practices that specifically train interoceptive awareness (attending to internal bodily sensations) increase the capacity to notice and name autonomic states in real time.
For avoidant individuals who have suppressed interoceptive access as part of the deactivating strategy, recovering the ability to sense internal state is prerequisite to being able to use social input to regulate it. R
For anxious individuals, mindfulness practices that cultivate equanimity toward internal states (observing activation without amplifying it through rumination) reduce the hyperactivating response to distress that prevents effective use of coregulatory support. R
6. Phosphatidylserine For HPA Normalization
Phosphatidylserine normalizes the hyper-responsivity of the HPA axis to acute stressors in chronically stressed individuals, working at the pituitary level to reduce excessive ACTH and cortisol release during stress. R
For anxiously attached individuals whose cortisol reactivity to social stress is chronically elevated, PS supplementation reduces the physiological cost of the hyperactivating strategy and may create more room for coregulatory inputs to produce calm. R
Typical dosing: 400 to 800 mg daily.
7. Magnesium For Sympathetic Tone
Magnesium glycinate reduces noradrenergic transmission and acts as a natural NMDA receptor modulator.
Chronic stress and the sustained sympathetic activation of insecure attachment strategies deplete magnesium, which further amplifies sympathetic hyperreactivity in a feedback loop.
Replenishment reduces the baseline sympathetic load that competes with parasympathetic engagement. R
Typical dosing: 300 to 400 mg elemental magnesium at night.
What To Stay Away From
- Relationships with highly dysregulated partners, which deplete regulatory capacity and prevent the stable, predictable availability that allows attachment updating (particularly problematic for anxiously attached individuals who amplify their partner's dysregulation) R
- Chronic isolation, which removes coregulatory input entirely and allows the nervous system's defensive set-points to consolidate without corrective experience R
- Reassurance-seeking loops without behavioral change for anxiously attached people, which temporarily reduce distress but reinforce the hyperactivating strategy rather than building genuine security (the relief is real, but the underlying prediction that proximity is unreliable is not updated) R
- Deactivating self-sufficiency framing for avoidantly attached people, which reinforces the suppression of the attachment system and prevents the gradual re-association of closeness with safety rather than threat R
- Trauma-processing without autonomic stabilization first for disorganized attachment, which can reactivate the collapsed regulatory system without the safety structures to hold the experience R
- Chronic sleep deprivation, which degrades the HRV recovery that occurs during sleep, reduces available regulatory capacity the next day, and makes all attachment strategies more extreme under daily stress R
- Alcohol and cannabis used to manage attachment-related distress, which produce acute autonomic dampening without updating the underlying threat-proximity association and chronically reduce HRV baseline R
Mechanisms Of Action
Simple:
- Attachment style is a learned physiological strategy for managing stress, shaped by whether proximity to the caregiver reliably produced autonomic calm in early development R
- Secure attachment: the social engagement system is open, social proximity reliably produces calm, and HRV is appropriately flexible across stress and recovery R
- Anxious attachment: the HPA axis is chronically primed, cortisol reactivity to social stress is elevated, and coregulation from others cannot be fully received because the threat detection system treats even genuine availability as potentially temporary R
- Avoidant attachment: the attachment system is deactivated, subjective distress is suppressed, but physiological stress markers (low HF-HRV, elevated electrodermal activity) persist, meaning the body pays the cost of the stress load without the relief of social buffering R
- Disorganized attachment: both the hyperactivating and deactivating systems fire simultaneously without resolution, producing the paradoxical HRV patterns, dissociative responses, and approach-avoidance oscillation characteristic of this style R
- The mechanism through which caregiving quality produces these physiological differences is partly epigenetic: responsive caregiving predicts lower NR3C1 methylation, and NR3C1 methylation determines glucocorticoid receptor density, which determines how efficiently the HPA axis self-regulates after stress R
Advanced:
The hyperactivating strategy: anxious attachment at the ANS level
The hyperactivating strategy involves persistent activation of the threat appraisal system, maintained vigilance for cues of abandonment or non-availability, and amplification of distress signals.
At the neuroendocrine level, this corresponds to elevated amygdala reactivity to negative social cues, heightened corticotropin-releasing hormone output, and a cortisol response that both overshoots baseline activation and shows delayed recovery. R
The anxious nervous system has been calibrated by early experience to weight the probability of non-response heavily.
Even when support is present and genuine, the amygdala continues to signal threat probability, which maintains HPA activation.
This is why partner support does not efficiently reduce cortisol in anxiously attached women during stress: the evaluation of "this is safe, I can relax" requires trust in the permanence and reliability of the support, which the anxious system cannot generate. R
The deactivating strategy: avoidant attachment at the ANS level
The deactivating strategy involves suppression of the subjective experience of distress, devaluation of the importance of close relationships, avoidance of dependency, and self-reliance. R
At the physiological level, this strategy successfully suppresses the reporting of distress but fails to suppress the autonomic and endocrine responses to it.
Avoidant individuals may report low stress while showing elevated electrodermal response and reduced HF-HRV.
This dissociation between subjective and physiological stress markers is a defining feature of the avoidant profile. R
The reduced HF-HRV in avoidant individuals reflects withdrawal of vagal brake function.
The vagal brake suppresses sympathetic influence on the heart and facilitates the social engagement system.
When the attachment system is chronically deactivated, so is the vagal input that would make coregulation possible.
The avoidant person is therefore physiologically unable to receive social soothing through the same mechanisms that they are behaviorally preventing from being offered. R
Physiological coregulation dynamics in couples
Physiological coregulation has been measured as the bidirectional linkage between partners' autonomic states over time, using time-series analysis of heart rate, HRV, and electrodermal activity during conversations.
Poor physiological coregulation (divergent autonomic states between partners) predicts larger increases in negative affect after conflict discussions. R
Dependent coregulation (anxious pattern): the person's physiology closely tracks their partner's, amplifying both increases and decreases.
Contrarian coregulation (avoidant pattern): the person's physiology diverges from the partner's, moving in the opposite direction to their partner's escalation or de-escalation.
Both patterns disrupt efficient physiological coregulation and increase negative affect outcomes after conflict. R
NR3C1 methylation as the biological bridge between caregiving and attachment
Maternal sensitivity shapes the epigenetic state of the NR3C1 promoter region in the child.
Higher maternal sensitivity predicts lower NR3C1 methylation.
Lower methylation means more glucocorticoid receptors are expressed.
More glucocorticoid receptors means cortisol negative feedback is more efficient.
More efficient feedback means the HPA axis turns off faster after stress.
A faster-recovering HPA axis makes it easier for social proximity to produce calm, because the cortisol alarm is not already running when the coregulatory input arrives. R R
Conversely, early adversity and low maternal sensitivity predict NR3C1 hypermethylation, reduced GR expression, impaired cortisol feedback, and a chronic HPA reactivity profile that makes the anxious hyperactivating strategy more physiologically costly and the coregulatory resolution of distress harder to achieve. R
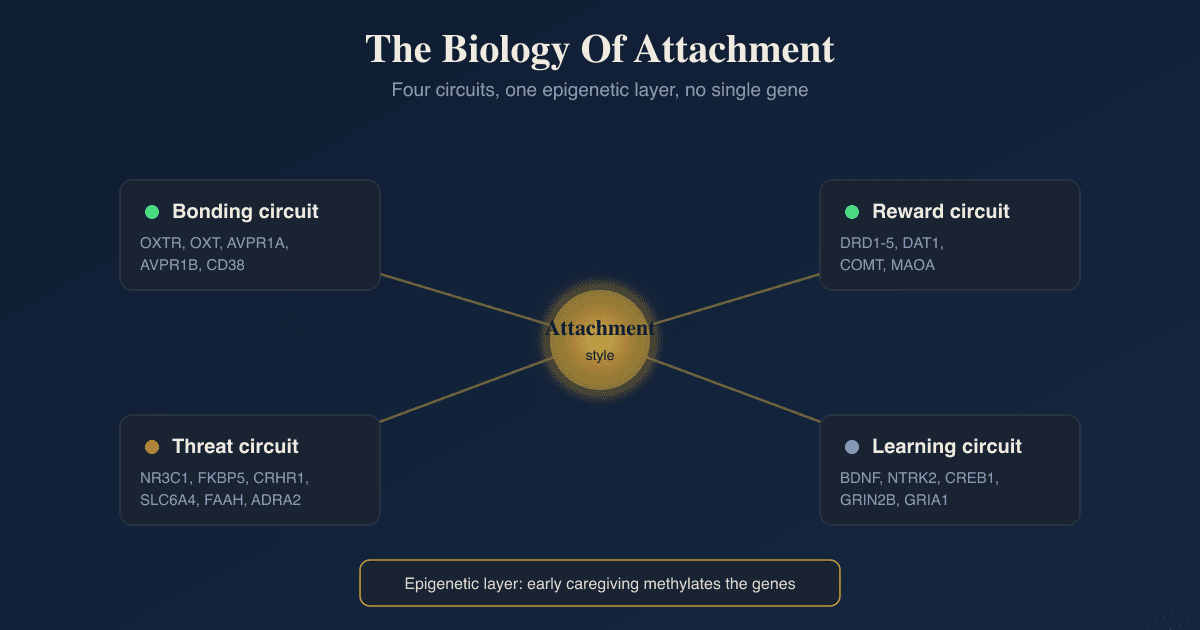
Genetics And Epigenetics
OXTR rs53576 (oxytocin receptor gene)
The OXTR gene encodes the oxytocin receptor, which mediates the calming and trust-promoting effects of oxytocin in limbic circuitry.
The A allele of rs53576 is associated with reduced oxytocin receptor expression and function.
Among veterans with insecure attachment, A allele carriers showed a prevalence of probable PTSD of 23.9% versus 2.0% in GG carriers with secure attachment (adjusted OR = 10.7).
The gene-by-attachment interaction was statistically significant (OR = 2.58, P = 0.02), meaning OXTR genotype moderates how much insecure attachment increases PTSD risk. R
Less secure attachment combined with OXTR rs53576 A allele carriage predicts greater social anxiety, consistent with a gene-environment interaction in which reduced oxytocin receptor efficiency amplifies the social threat reactivity of insecure attachment. R
The A allele of rs2254298 (a separate OXTR SNP) was associated with attachment security in non-Caucasian infants in the Strange Situation (P < 0.005), suggesting that oxytocin receptor variation contributes to the initial formation of attachment security through modulation of social stress regulation and trust development. R
OXTR G/G genotype and stability of attachment across development
The continuity of attachment security from infancy into young adulthood was consistently moderated by OXTR genetic variation in a prospective longitudinal study.
Infant attachment security predicted adult attachment security (measured by Adult Attachment Interview at ages 19 and 26 and Current Relationship Interview at ages 26 to 28) only for individuals with the OXTR G/G genotype.
This moderation was significant across multiple measurement points.
DRD4 and 5-HTTLPR genetic variation did not consistently moderate this longitudinal association. R
OXTR G/G carriers whose early secure attachment was disrupted by adverse experiences showed more attachment security recovery in adulthood.
A allele carriers showed less recovery, suggesting that the oxytocin system moderates both the stability of secure attachment and the resilience of the attachment system after disruption. R
5-HTTLPR (serotonin transporter, SLC6A4)
The short (s) allele of 5-HTTLPR is associated with reduced serotonin transporter expression and elevated amygdala reactivity to emotional stimuli.
Parents with the s/s genotype of 5-HTTLPR showed lower levels of sensitive responsiveness to their toddlers, independent of maternal education, depression, and marital quality. R
Given that caregiver sensitivity is the primary environmental driver of attachment security, 5-HTTLPR effects on parenting represent one pathway through which serotonin system genetics influence the attachment security of the next generation. R
NR3C1 methylation (epigenetic, not genetic)
NR3C1 methylation at exon 1F is the most replicated epigenetic mechanism linking early adversity to HPA dysregulation and attachment insecurity.
Several types of early life stress are associated with NR3C1 hypermethylation, while PTSD is associated with hypomethylation.
The direction of methylation change differs by the type of stress and its developmental timing. R
NR3C1 methylation moderates the effect of maternal support on anxious attachment development.
Highly methylated children who received less maternal support during stress showed significantly greater anxious attachment 18 months later. R
Mother-child NR3C1 methylation signatures are correlated, providing evidence for intergenerational epigenetic transmission of stress reactivity that operates in parallel with behavioral transmission of attachment patterns. R
COMT Val158Met
Children with the Val/Met genotype of COMT Val158Met showed higher disorganized attachment scores across two independent birth cohort studies (combined effect size d = 0.22, CI 0.10 to 0.34, P < 0.001), the most consistent genetic finding for disorganized attachment in large-scale studies. R
COMT Val158Met affects dopamine metabolism in prefrontal cortex.
The Val allele produces faster dopamine catabolism, reducing PFC dopamine availability and impairing prefrontal regulation of the amygdala and the threat appraisal system.
The connection to disorganized attachment likely operates through reduced top-down regulation of limbic threat circuitry under conditions of unpredictable caregiver threat. R
More Research
- Physiological coregulation measurement as a clinical tool. The field has validated psychophysiological paradigms (RSA synchrony, HRV coupling during interaction, electrodermal concordance) that can objectively characterize how efficiently two nervous systems coregulate in real time. R These measures could be used clinically to identify patterns (contrarian vs. dependent coregulation) and track therapy progress. Current therapy assessment almost exclusively uses self-report. Adding even basic HRV measurement before and after therapy would connect the subjective experience of change to its physiological substrate.
- The epigenetic reversibility question. NR3C1 methylation established in early life influences attachment and HPA reactivity across the lifespan. R Whether sustained positive relationship experiences, effective psychotherapy, or biological interventions can reverse NR3C1 methylation in adulthood is an active research question with real implications: if the answer is yes, the biological embedding of insecure attachment is not permanently fixed. Animal research suggests maternal licking and grooming can reverse adversity-induced methylation in offspring. Human translation of this finding is underway.
- Sex differences in attachment physiology. Males and females show systematically different physiological responses to attachment-related stress, with females showing more robust cortisol reactivity to social stress and males showing greater electrodermal reactivity. R The CRH receptor internalization sex difference (females show heightened CRH sensitivity under stress; males show receptor downregulation) adds a mechanistic layer to why anxious attachment produces different physiological phenotypes in men and women. This has direct clinical implications for treatment targeting and outcome expectations.
- For biomarker assessment of attachment-related dysregulation, resting HRV measured over 24 hours (not just during rest) captures both baseline vagal tone and the diurnal HRV pattern that reflects autonomic flexibility across the full day-night cycle. The cortisol awakening response (CAR) measured via 4-point salivary cortisol on waking provides the most functionally relevant HPA axis assessment because it reflects the morning HPA drive that shapes the day's regulatory capacity. Both are accessible through consumer monitoring and home testing services.
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Lion's Mane
1000mg/day
Omega-3 (DHA)
2g/day
Phosphatidylserine
100mg 3x/day