Restless Leg Syndrome: The Brain Iron Deficiency And Dopamine Connection
By Jacob Gordon, INHC, FMT-CThis article contains affiliate links. As an Amazon Associate, MyBioHack earns from qualifying purchases at no extra cost to you. We only link products we research and stand behind.
Restless leg syndrome is a sensorimotor disorder where the core problem is not in the legs at all but in a brain that cannot get enough iron into the right cells, even when blood tests look normal.
In this post, we will discuss what restless leg syndrome actually is, why serum ferritin can read normal while brain iron runs low, how the dopamine system gets pulled into it, why the standard drugs often make it worse over time, the genetic risk variants behind it, and an evidence-based approach to iron repletion built around targets specific to this condition.

Basics Of Restless Leg Syndrome
Restless Leg Syndrome (RLS), also called Willis-Ekbom disease, is defined by an urge to move the legs that is usually paired with an uncomfortable sensation deep in the limbs.
The International Restless Legs Syndrome Study Group (IRLSSG) diagnostic criteria require five features to all be present. R
The urge to move begins or worsens during rest.
It is partially or fully relieved by movement for as long as the movement continues.
It is worse in the evening or night than during the day.
And it is not better explained by another condition such as leg cramps or positional discomfort. R
That last circadian feature is a clue to the mechanism, because both brain iron and dopamine signaling follow a daily rhythm that bottoms out at night.
RLS is common, with a pooled global prevalence of roughly 7% among adults, which works out to hundreds of millions of people. R
Most cases are primary (genetic, familial, and lifelong), while secondary cases stack on top of iron deficiency, pregnancy, kidney disease, or certain medications.
What Causes Restless Leg Syndrome
The single most reproducible finding in RLS is not low blood iron but low brain iron.
This is the part that confuses patients and clinicians alike, so it is worth stating plainly.
You can have a completely normal serum ferritin and still have an iron-starved brain.
When researchers measured iron transport proteins in spinal fluid, people with RLS had significantly lower cerebrospinal fluid ferritin and higher cerebrospinal fluid transferrin than controls, despite identical serum ferritin values. R
Elevated transferrin with low ferritin in the fluid bathing the brain is the biochemical signature of a tissue that is trying to pull in more iron and failing.
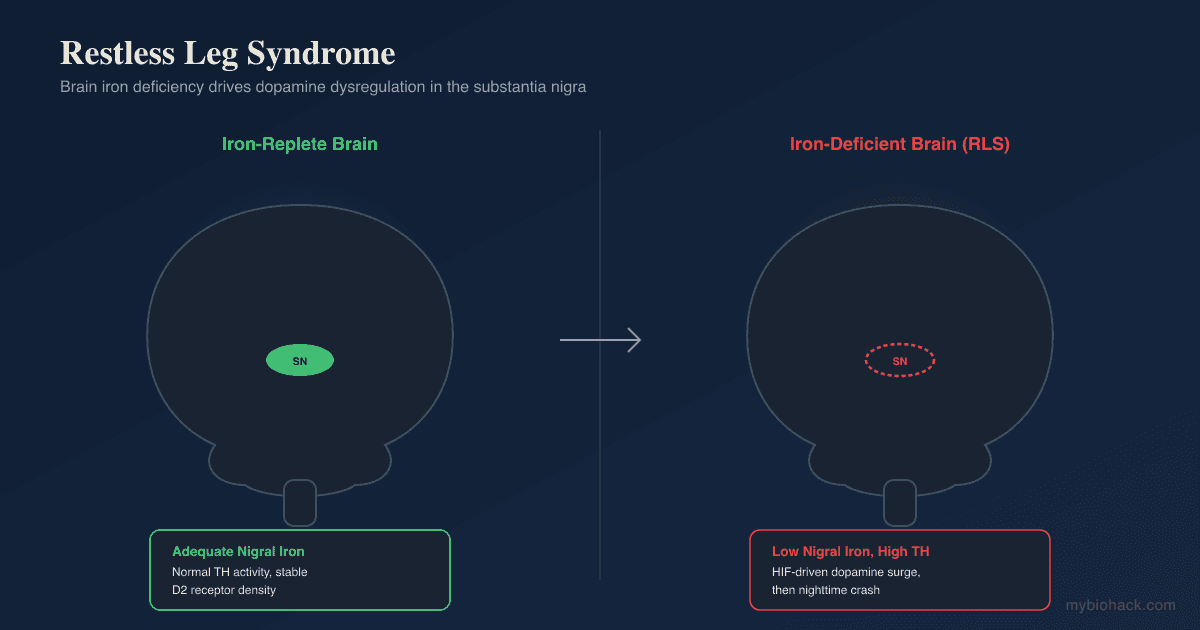
Brain imaging tells the same story from a different angle, because MRI relaxometry finds reduced iron in the substantia nigra of people with RLS in proportion to symptom severity, even when peripheral iron reads normal. R R
Root causes and contributors (not an exclusive list):
- Genetic risk variants in MEIS1, BTBD9, and MAP2K5/SKOR1 that shape iron handling and dopamine circuits R
- Impaired iron transport across the blood-brain barrier, where neuromelanin cells fail to acquire iron even when peripheral stores are adequate R R
- Kidney disease and dialysis, which drive some of the highest RLS rates of any population R
- Peripheral iron deficiency, which lowers the ceiling on what the brain can import
- Pregnancy, especially the third trimester, when iron demand peaks R
- Pro-dopaminergic and antidopaminergic drugs, which either provoke the circuit or unmask it
The genetic and the iron stories are the same story, because the risk genes themselves govern how iron and dopamine are managed in the brain.
How Brain Iron And Dopamine Create The Problem
Iron is a required cofactor for tyrosine hydroxylase (TH), the rate-limiting enzyme that converts tyrosine into L-DOPA on the way to dopamine.
The intuitive assumption is that low brain iron would lower dopamine, but the data show the opposite, and this inversion is the key to understanding the whole condition.
Autopsy tissue from people with primary RLS showed increased tyrosine hydroxylase in the substantia nigra, roughly 40% higher total TH and 86% higher phosphorylated (active) TH, alongside a decrease in D2 dopamine receptors in the putamen that tracked with symptom severity. R
In other words, the RLS brain is not dopamine-deficient at the source.
It is running an overactive, dysregulated dopamine system with downregulated receptors, which is exactly what you would expect from a system that is flooded during the day and crashing at night.

The mechanistic bridge is the hypoxia-inducible factor (HIF) pathway.
Brain iron deficiency activates HIF, which upregulates tyrosine hydroxylase and dopamine synthesis, while simultaneously reducing dopamine transporter function at the cell membrane so that extracellular dopamine accumulates. R
The result is high dopamine tone during the day and a steep withdrawal at night when dopamine naturally falls, which lines up with why symptoms hit in the evening.
There is a second, less discussed arm to this.
Brain iron deficiency also downregulates adenosine A1 receptors and shifts the balance toward A2A receptors, which removes a brake on glutamate release and produces a hyperglutamatergic, hyperarousable state. R
This adenosine-glutamate axis is why some people get the sensory and arousal components of RLS that pure dopamine models never fully explained.
Neuropathology confirms the upstream problem is iron acquisition itself.
The neuromelanin cells of the substantia nigra in RLS show a protein profile consistent with cells that cannot properly regulate their transferrin receptors, meaning they are locked out of the iron they need rather than degenerating. R R
This is why RLS is best understood as a functional iron-acquisition disorder of the brain, not a neurodegenerative disease.
Restless Leg Syndrome And Overlapping Conditions
RLS rarely travels alone, and the overlaps point back to iron, dopamine, and sleep architecture.
Conditions that cluster with RLS (not an exclusive list):
- Attention and dopamine-related conditions, given the shared dopaminergic circuitry
- Chronic kidney disease and dialysis, one of the strongest secondary drivers
- Insomnia and fragmented sleep, both as a consequence of nighttime symptoms and as an independent overlap driven by the same arousal systems (see gut microbiome and insomnia)
- Iron deficiency anemia, which lowers the brain's iron ceiling
- Periodic limb movements of sleep, which share the BTBD9 genetic risk variant R
- Peripheral neuropathy and small-fiber neuropathy, which can mimic or coexist with RLS
- Pregnancy, where symptoms often appear or worsen and then remit after delivery
The sleep overlap is bidirectional, because the same adenosine-glutamate imbalance that drives the leg symptoms also drives hyperarousal, so treating one without the other tends to disappoint.
How To Improve Restless Leg Syndrome
The evidence-based core is iron repletion aimed at brain-specific targets, not the anemia targets most doctors default to.
Standard practice treats iron as normal once you are out of the anemia range, but RLS needs a much higher floor because the problem is getting iron across the blood-brain barrier.
1. Repair Brain Iron With Oral Iron (Correctly Dosed)
The consensus target for RLS is a serum ferritin above 75 ng/mL, which is far higher than the roughly 15 to 30 ng/mL that ends a diagnosis of anemia. R
Take iron with vitamin C on an empty stomach, and take it every other day rather than daily.
Alternate-day dosing raises total absorption by lowering hepcidin, the hormone that a fresh iron dose spikes for the next 24 hours. R
A chelated, gentle form that is easier on the gut than ferrous sulfate at an equivalent elemental dose.
The best-studied form, with about 65 mg of elemental iron per 325 mg tablet, effective but more likely to cause constipation.
Taken alongside iron, it reduces ferric to ferrous iron and meaningfully improves absorption. R
2. Consider IV Iron When Oral Fails Or Stores Are Very Low
Some people cannot absorb enough oral iron, do not tolerate it, or need faster repletion, and for them intravenous iron is the better tool.
A single 1000 mg dose of ferric carboxymaltose produced significant and clinically meaningful improvement in RLS severity by week 12 in patients with nonanemic iron deficiency. R
This is a prescription procedure that requires a physician, and it is worth discussing if oral iron stalls or your ferritin will not climb.
3. Correct The Cofactors
Iron does not work in isolation, and several cofactor deficiencies both worsen RLS and blunt iron's benefit.
Supports the glutamate-GABA balance that the adenosine shift disrupts, and the glycinate form is calming rather than laxative.
Low folate is a recognized secondary cause, especially in pregnancy, and it is a cofactor in dopamine synthesis.
Deficiency contributes to the neuropathy that overlaps with and mimics RLS.
Low vitamin D correlates with RLS severity and is worth correcting given how common the deficiency is. R
4. Support Dopamine Without Overdriving It
Because the RLS brain is already running an overactive dopamine system, the goal is to support healthy dopamine metabolism, not to flood the receptors the way the drugs do.
Gentle nutritional support of the pathway is safer than pharmacologic overdrive, and you can go deeper in the posts on how to increase tyrosine hydroxylase and increase dopamine naturally.
5. Fix Sleep And The Arousal System
Because the same adenosine-glutamate imbalance drives both the legs and the arousal, addressing sleep directly matters.
Keep a consistent sleep window, get morning light, and treat any coexisting insomnia driver, including the gut microbiome contribution to insomnia.
What To Stay Away From
Several everyday substances and drug classes provoke RLS by antagonizing dopamine, depleting iron, or raising arousal.
Things that commonly worsen RLS (not an exclusive list):
- Alcohol, which fragments sleep and worsens evening symptoms
- Antihistamines, especially sedating first-generation ones like diphenhydramine, which block central histamine and can trigger flares
- Caffeine, particularly in the afternoon and evening
- Dopamine-blocking antiemetics such as metoclopramide and prochlorperazine
- Dopamine agonists over the long term, because of augmentation (covered below)
- Iron overloading without testing, because blindly loading iron is dangerous in anyone carrying an HFE variant (see iron overload, ferritin, and hemochromatosis)
- Nicotine, a stimulant that worsens nighttime symptoms
- Sedating antidepressants and most SSRIs and SNRIs, which frequently intensify RLS (mirtazapine is the worst offender) R
The augmentation problem deserves its own warning.
Dopamine agonists like pramipexole and ropinirole work at first, but over months to years they paradoxically worsen RLS, a phenomenon called augmentation, where symptoms start earlier in the day, spread to the arms, and become more intense than before treatment. R
In a head-to-head trial, the alpha-2-delta ligand pregabalin produced far less augmentation than pramipexole over a year (2.1% versus 7.7% at the 0.5 mg dose). R
The mechanistic reason augmentation happens is that pushing more dopamine onto already-downregulated, overdriven receptors accelerates the exact receptor changes that cause the disease, which is why fixing brain iron is the more durable strategy.
Testing
The most important point is that a normal ferritin does not rule out RLS-relevant iron deficiency, because the RLS target is much higher than the anemia cutoff.
Blood And Urine Markers
Draw iron studies in the morning while fasting, because serum iron and transferrin saturation swing widely across the day. R
Ferritin is the storage marker, and for RLS the treatment threshold is a level at or below 75 ng/mL, not the far lower anemia cutoff. R
Transferrin saturation (TSAT) below 20% supports iron repletion, while a TSAT above 45% is a signal to stop and rule out overload before giving any iron. R
I use the Ferritin test (Quest Diagnostics) to check storage iron, and the Iron + Total Iron Binding Capacity panel (Quest Diagnostics) to calculate transferrin saturation.
For serum iron alone, the Iron, Total test (Quest Diagnostics) is the simplest option.
Functional Lab Panels
I use the Foundation Zoomer (Vibrant Wellness) to get the CBC, metabolic, and thyroid context around iron status, since anemia, kidney function, and thyroid all shape the picture.
For the broader nutrient cofactors that overlap with RLS, I use the Nutrient Zoomer (Vibrant Wellness) to assess B12, folate, vitamin D, copper, and zinc together.
Genetics And Overload Screening
Before aggressive iron loading, anyone with a high ferritin, a high transferrin saturation, or a family history of iron overload should be screened for hereditary hemochromatosis with the Hereditary Hemochromatosis DNA Analysis (Quest Diagnostics), which tests the HFE gene.
Loading iron into an undiagnosed HFE homozygote is how you turn a treatable sleep problem into organ damage, so this screen matters when the numbers are ambiguous.
If your case is complex or the iron numbers are not adding up, this is a good point to work with someone directly, and you can reach out through the consultation page.
Mechanisms Of Action
Simple:
- The brain cannot pull in enough iron, so it overreacts by cranking up dopamine production during the day, which then crashes at night and leaves the legs restless.
- Iron is the raw material and the traffic controller for dopamine, and when the brain runs short, both the production and the disposal of dopamine go haywire.
- The same iron shortage lifts a brake on the brain's arousal chemistry, which is why RLS also wrecks sleep and not just the legs.
Advanced:
- HIF-driven dopamine dysregulation: Brain iron deficiency activates the hypoxia-inducible factor pathway, which upregulates tyrosine hydroxylase (the iron-dependent rate-limiting step in catecholamine synthesis) while simultaneously reducing dopamine transporter density and function at the membrane. R The net effect is elevated extracellular dopamine and compensatory downregulation of postsynaptic D2 receptors, matching the autopsy finding of raised TH in the substantia nigra and reduced D2 receptors in the putamen. R
- Adenosine A1 to A2A shift: Iron deficiency downregulates adenosine A1 receptors and relatively favors A2A receptors in corticostriatal terminals, and because A1 receptors normally suppress glutamate release through A1-A2A heteromers, their loss produces a hyperglutamatergic, hyperarousable state that accounts for the sensory and sleep-arousal features not explained by dopamine alone. R
- Impaired neuromelanin iron acquisition: The neuromelanin cells of the substantia nigra in RLS show altered iron-management protein profiles consistent with dysregulated transferrin receptor control, so the cells are functionally locked out of iron despite adequate peripheral stores, framing RLS as an acquisition defect rather than a degenerative loss of cells. R
- Central versus peripheral iron dissociation: Cerebrospinal fluid ferritin is low and cerebrospinal fluid transferrin is high in RLS despite normal serum ferritin, demonstrating that the brain iron compartment is regulated separately from blood stores and explaining why serum ferritin is an insensitive marker of the deficit that actually drives symptoms. R
Genetics

MEIS1: Highest Population Risk
MEIS1 is a homeobox transcription factor gene involved in the development of the striatal circuits and cholinergic interneurons that regulate movement.
Common intronic variants in MEIS1 are the strongest known genetic risk factor for RLS, and mouse models with reduced Meis1 show RLS-like motor restlessness and altered striatal dopamine turnover. R
rs2300478 and rs12469063: intronic MEIS1 variants repeatedly associated with RLS across multiple populations. R R
BTBD9
BTBD9 encodes a BTB/POZ domain protein linked to both iron regulation and periodic limb movements.
Variants in BTBD9 associate with RLS, with lower serum ferritin, and with periodic limb movements of sleep, and knockout of the mouse homolog produces motor restlessness, disrupted sleep, and elevated serum iron. R
rs9296249 and rs9357271: BTBD9 variants associated with RLS and reduced iron stores. R R
MAP2K5/SKOR1
MAP2K5 is the kinase gene at this locus, and SKOR1 is the transcriptional co-repressor it sits alongside, the latter directly regulated by MEIS1.
Variants here influence the development of sensory and motor neurons relevant to the RLS circuit.
rs12593813: a MAP2K5/SKOR1 variant confirmed as an RLS risk allele in genome-wide and replication studies. R R
More Research
Augmentation is the strongest argument against reaching for dopamine agonists first, because the drugs that give the fastest relief are the ones most likely to make the disease permanently worse, and alpha-2-delta ligands like gabapentin and pregabalin carry a much lower augmentation risk. R R
Brain iron deficiency with normal blood iron is the central paradox of RLS, and it is the reason a patient can be told their labs are fine while their brain is measurably iron-starved on spinal fluid analysis and imaging. R R
For iron testing I use the Ferritin and Iron + Total Iron Binding Capacity tests (Quest Diagnostics) to track both storage iron and transferrin saturation against the RLS-specific target of ferritin above 75 ng/mL rather than the anemia cutoff. R
Intravenous ferric carboxymaltose is a legitimate option when oral iron fails, and its benefit in nonanemic iron deficiency is direct evidence that the deficit driving RLS is functional and brain-specific rather than a matter of red-cell iron. R
The adenosine-glutamate arm of the model is the most important recent addition, because it explains the arousal and sensory features that dopamine-only models missed and points toward adenosine and glutamate modulation as future targets. R
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Lion's Mane
1000mg/day
Omega-3 (DHA)
2g/day
Phosphatidylserine
100mg 3x/day





