Topical Magnesium Cannot Cross Your Skin: The Biophysics Of A Hydrated Ion
By Jacob Gordon, INHC, FMT-CThis article contains affiliate links. As an Amazon Associate, MyBioHack earns from qualifying purchases at no extra cost to you. We only link products we research and stand behind.
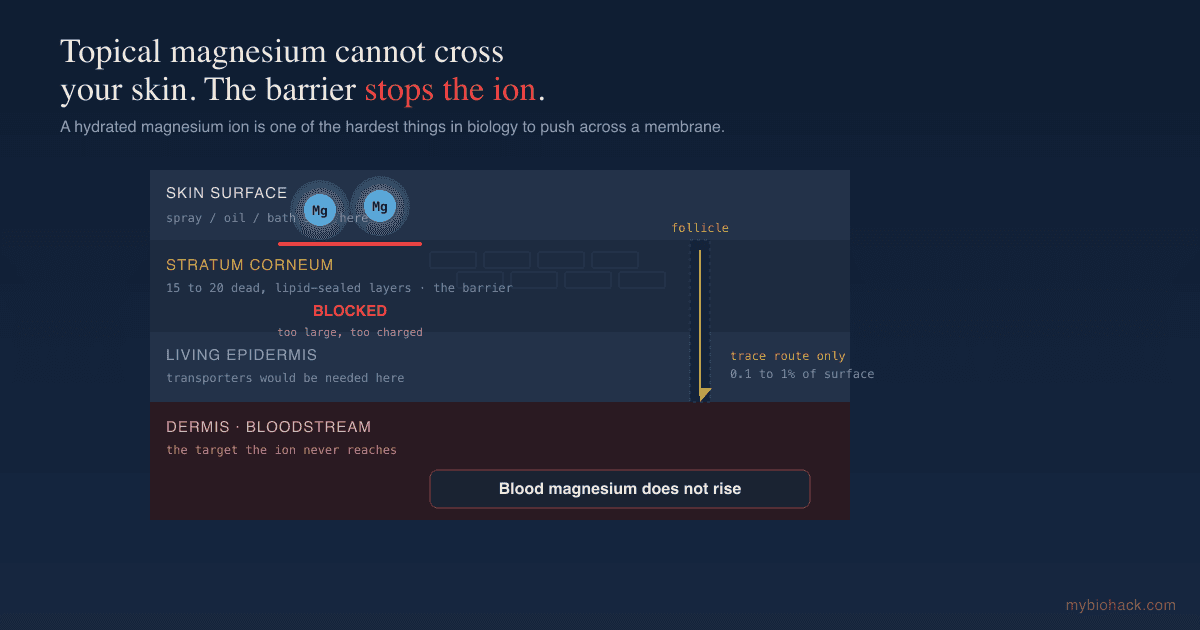
Magnesium sprays, oils, and bath flakes promise to fix a deficiency through your skin, but the biophysics of the magnesium ion and the structure of your skin barrier make that route close to useless.
In this post, we will discuss why magnesium cannot meaningfully cross intact skin, what the human trials actually show, why the deficiency is still worth fixing, and the oral forms that actually raise your magnesium.

Basics: The Transdermal Magnesium Pitch
Walk into any wellness shop and you will find magnesium sprays, oils, and bath flakes promising to fix a deficiency through your skin.
The pitch is appealing, because it claims you can skip the gut entirely, avoid the loose stools that high-dose oral magnesium can cause, and absorb the mineral straight into the body.
The problem is that the claim runs head-on into one of the most basic facts about how this particular ion behaves in water.
Magnesium is not a molecule that quietly slips through a fatty membrane.
It is a small, doubly charged ion that grips water harder than almost anything else moving through your tissues, and your skin is specifically engineered to keep things like it out.
The Magnesium Ion Carries A Shell Of Water
Magnesium in solution does not travel as a bare atom.
It carries a tightly held shell of water molecules, and the hydrated ion is roughly 400 times larger by volume than its dehydrated core. R
That is the largest hydration ratio of any common biological cation, far beyond sodium, potassium, or calcium. R
The reason is charge density.
Magnesium packs a double positive charge onto a very small ionic radius, so it pulls water in close and holds it tightly. R
To cross a fatty membrane, the ion would have to strip that water shell off, which costs a large amount of energy, and that energy barrier is exactly why no cell in the body moves magnesium by simple diffusion.
Every bit of magnesium that enters a cell is shuttled through dedicated protein transporters, such as TRPM6 and TRPM7, built specifically for the job. R
A spray sitting on your skin has none of those transporters working for it.
It has only diffusion, and diffusion is the one route a hydrated divalent ion is worst at.
Your Skin Is Built To Keep Ions Out
Now look at what the spray actually has to get through.
The outermost layer of skin, the stratum corneum, is 15 to 20 layers of dead, flattened cells with no nuclei and no functioning transporters.
Those dead cells are packed into a water-repellent matrix of ceramides, cholesterol, and free fatty acids, with almost none of the phospholipids found in living membranes. R
This layer is engineered to keep the outside world out, and only fat-soluble molecules cross it in meaningful amounts. R
A hydrated, doubly charged ion is the chemical opposite of fat-soluble.
It is large, it is charged, and it is wrapped in water, which is the worst possible profile for crossing a lipid barrier.
The only real openings in this barrier are hair follicles and sweat glands, and those account for somewhere between 0.1 and 1 percent of your skin's surface area. R
A pore here and there is not a delivery system.
What The Human Trials Actually Show
The theory is clear, and the human data line up with it.
A 2017 review in Nutrients evaluated the evidence and concluded that transdermal magnesium is scientifically unsupported. R
A 2017 pilot study put a magnesium cream against a placebo cream for two weeks and measured serum and 24-hour urinary magnesium. R
The cream was null for the group as a whole, reaching statistical significance only in a small subgroup of non-athletes, which is the kind of result that appears when an effect is at the edge of the noise rather than real and robust. R
The follicle route, the one genuine opening, has been imaged directly, and it moves only trace amounts through that tiny fraction of skin. R
None of these studies show the kind of serum rise you would need to correct an actual deficiency.
They show a barrier doing its job.
The Follicle Loophole
The strongest argument the transdermal crowd has is the hair follicle.
Follicles bypass the stratum corneum, and researchers have shown that magnesium ions can travel down them into deeper skin. R
This is real, and it is worth being precise about rather than dismissing it outright.
The problem is arithmetic.
Follicles and sweat glands are 0.1 to 1 percent of your skin's surface, so even if the follicle route worked perfectly, it would be drawing from a sliver of the available area. R
A trace amount through a tiny fraction of skin does not add up to a meaningful dose, which is exactly what the serum measurements keep showing.
The loophole exists.
It is just far too small to drive through.

Magnesium Deficiency Is Real, So The Route Matters
None of this means magnesium is useless, and that is the part the debunking crowd often gets wrong.
Magnesium runs more than 600 enzymatic reactions, including the ones that make ATP, so being low has real consequences. R
Subclinical magnesium deficiency is common in modern populations, driven by depleted soils, refined food, chronic stress, and several common medications, and most of it goes undiagnosed. R
It goes undiagnosed in part because the standard serum magnesium test does not reflect the magnesium stored inside your cells, so you can run a normal blood level and still be functionally low. R
Stress and low magnesium also feed each other in a vicious circle, where stress wastes magnesium and low magnesium amplifies the stress response. R
So the deficiency is worth taking seriously.
The point is not that magnesium does not matter, it is that the route matters, and the skin is the wrong route.
Magnesium, Mast Cells, And The Chronically Ill
This is where magnesium becomes more than a general wellness mineral, because the chronically ill population I work with is both more likely to be depleted and more dependent on what magnesium does.
Magnesium sits in the pore of the NMDA receptor as a natural block, which restrains glutamate excitotoxicity, and losing that block is part of how a stressed nervous system tips toward overexcitation and tinnitus. R
Magnesium also helps stabilize mast cells and supports the calm side of the nervous system, which matters for anyone dealing with histamine intolerance or mast cell activation.
It is a required cofactor for methylation, so being low quietly drags on a pathway that touches detox, neurotransmitters, and gene regulation.
Several of the drugs this population takes actively waste magnesium, and proton pump inhibitors are the clearest example, with long-term use linked to frank hypomagnesemia.
In other words, the people most likely to reach for a magnesium spray because it feels gentle are often the ones who most need a route that actually works.
How To Actually Raise Your Magnesium
Oral magnesium is one of the best-documented mineral interventions there is, and the form matters more than the marketing.
Bioavailability differs between forms, with the organic, chelated forms generally outperforming cheap magnesium oxide, which is poorly soluble and mostly acts as a laxative. R
1. For general repletion and sleep
Magnesium glycinate pairs magnesium with the calming amino acid glycine, is gentle on the gut, and is my default for sleep and general repletion.
Oral magnesium has held up in randomized trials for insomnia, modestly shortening the time it takes to fall asleep. R
2. For constipation or quick repletion
Magnesium citrate is well absorbed and draws water into the bowel, which makes it useful if you are also constipated, and oral citrate has outperformed oxide in absorption studies. R
3. For the brain and NMDA balance
Magnesium L-threonate is the form shown to raise magnesium in the brain, where it increases NMDA receptor signaling, synaptic density, and learning in animal models. R
This is the form I reach for when the goal is cognition, GABA tone, and calming an overexcited nervous system rather than just topping up body stores.
4. For muscle and energy
Magnesium malate ties magnesium to malate, an intermediate in the energy cycle, and is a reasonable choice for muscle aches and ATP production.
5. For the cardiovascular system
Magnesium taurate pairs magnesium with taurine and is often chosen for blood pressure and vascular support.
Take magnesium with food, split larger doses across the day to improve tolerance, and titrate to just below the dose that loosens your stool.
What To Stay Away From
Magnesium sprays and oils marketed for repletion: the serum data do not support them as a way to correct a deficiency, however pleasant they feel on sore muscles.
Epsom salt baths as a magnesium source: the absorption claim rests on the same broken transdermal logic, even if the warm soak itself is relaxing.
Magnesium oxide as your only form: it is cheap and common but poorly absorbed, so most of the dose acts as a laxative rather than repleting you.
Mega-dosing any oral form at once: pushing the dose past your gut tolerance just causes diarrhea, which then wastes minerals, so split it instead.
Trusting a normal serum magnesium to rule out deficiency: serum magnesium misses the intracellular pool, so a "normal" result does not mean you are replete.
Testing
Confirming magnesium status is harder than it looks, because the cheap, common test is the weakest one.
Blood And Functional Markers
Standard serum magnesium is the routine test, but it reflects only a small fraction of total body magnesium and stays normal until you are quite depleted, so a normal value does not rule out a deficiency. R
Red blood cell magnesium and functional intracellular measures track your stores more closely than serum.
Functional Lab Panels
I use the Nutrient Zoomer (Vibrant Wellness) to assess magnesium alongside the other minerals, vitamins, and amino acids it competes and works with, which gives a fuller picture than a single serum value.
For a more functional read on how your cells are actually using magnesium, the Cellular Zoomer (Vibrant Wellness) covers organic acids that shift when magnesium-dependent energy pathways are struggling.
Mechanisms Of Action
Simple:
- Magnesium is a tiny ion wrapped in a thick coat of water, and your skin is built to block exactly that kind of thing, so sprays and baths leave your blood magnesium essentially unchanged while swallowing magnesium works.
Advanced:
- Charge density and hydration: magnesium's double charge on a small radius gives it the highest charge density of the major biological cations, so it binds a large hydration shell and pays a steep desolvation energy cost to cross any lipid membrane. R
- Transporter dependence: because passive diffusion is so unfavorable, cellular magnesium uptake runs through dedicated channels and transporters like TRPM6 and TRPM7, none of which exist in the dead stratum corneum. R
- Stratum corneum barrier: the outer skin is corneocytes embedded in a ceramide, cholesterol, and fatty acid matrix with no phospholipids, a structure optimized to admit lipophilic molecules and exclude hydrated ions. R
- Follicular shunt: the only appreciable transdermal route for magnesium is the follicular and sweat-gland pathway, which covers 0.1 to 1 percent of skin surface and carries only trace amounts. R
- NMDA channel block: inside the brain, magnesium occupies the NMDA receptor pore in a voltage-dependent manner, limiting calcium influx and excitotoxicity, which is part of why brain-penetrant forms matter for the nervous system. R
Genetics
TRPM6
TRPM6 encodes the channel that absorbs magnesium in the intestine and reabsorbs it in the kidney.
Loss-of-function mutations cause hereditary hypomagnesemia, and common variants nudge how well you hold onto magnesium.
rs11144134 and related variants are associated with differences in serum magnesium and reabsorption efficiency. R
CNNM2
CNNM2 encodes a magnesium transporter active in the kidney's handling of the ion.
Variants here are linked to hypomagnesemia and, in severe cases, to neurological features.
This is one of the genes that explains why some people stay low despite a reasonable intake. R
More Research
Genetics aside, the largest driver of low magnesium in modern populations is environmental, between depleted agricultural soils, food refining that strips magnesium out, and medications that waste it. R
Oral magnesium has signals beyond sleep and migraine, including improved insulin sensitivity in insulin-resistant subjects, which fits its central role in energy metabolism. R
Oral magnesium has also held up in randomized prophylaxis trials for migraine, where high-dose oral magnesium reduced attack frequency against placebo. R
For magnesium and mineral status I use the Nutrient Zoomer (Vibrant Wellness) rather than a single serum value, because the serum test is the part of this picture most likely to mislead.
The open question is not whether the skin blocks magnesium, which is settled, but how much of the reported subjective benefit from sprays and baths is the warm water, the massage, and the relaxation rather than the mineral, and that is the part the trials have not cleanly separated.
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Electrolyte Complex
1 scoop/day
CoQ10
200mg/day
Magnesium Glycinate
400mg at bedtime