The Autoimmune Protocol (AIP) Diet: How Elimination Eating Reduces Inflammation
By Jacob Gordon, INHC, FMT-CThe Autoimmune Protocol (AIP) diet is a structured elimination-and-reintroduction framework designed to reduce intestinal permeability, quiet immune activation, and identify the specific foods driving inflammation in each person.
In this post, we will discuss what the AIP diet is, which foods it eliminates and why, how the elimination and reintroduction phases work, the mechanistic rationale behind the diet, how it overlaps with related conditions, and what testing looks like before starting.

Basics Of AIP
The Autoimmune Protocol (AIP) is a therapeutic elimination diet originally developed from the Paleo diet framework by researchers including Dr. Sarah Ballantyne, who synthesized the immunology behind food-driven autoimmune flares. R
The diet has three phases: an elimination phase (typically 30 to 90 days) where potentially inflammatory foods are removed, a reintroduction phase where foods are tested one at a time to identify individual triggers, and a long-term maintenance phase built around a personalized diet that excludes only the foods that cause reactions for that person. R
The goal is not permanent restriction.
The goal is to learn which foods your body tolerates and which ones drive inflammation, then build a sustainable diet around that knowledge.
Unlike general anti-inflammatory diets, AIP is a temporary investigative tool.
It removes foods that are otherwise considered healthy (eggs, nuts, nightshade vegetables, seeds) because these foods have the potential to trigger immune responses in susceptible individuals.
AIP emerged from clinical research showing that diet can meaningfully alter the course of autoimmune disease.
The most cited trial is the 2017 Konijeti study at Scripps, where 15 patients with active Crohn's disease or ulcerative colitis followed AIP for six weeks of elimination plus five weeks of maintenance. R
At week six, 73 percent achieved clinical remission, with improvements confirmed on endoscopy and in inflammatory markers.
A 2019 pilot study by Abbott and colleagues found that 17 women with Hashimoto's thyroiditis reported significant improvements in quality of life and symptom burden after 10 weeks on AIP, though the study was small and uncontrolled. R
A 2023 study on AIP in Hashimoto's disease showed improvements in thyroid parameters and quality of life after 12 weeks. R
A 2026 pilot study in rheumatoid arthritis found that nine participants showed clinically meaningful reductions in disease activity scores after eight weeks on AIP. R
The evidence base remains modest.
All published trials are small, open-label, and lack control arms.
But the effect sizes are large enough that the diet warrants serious consideration for anyone with an autoimmune condition.
What AIP Eliminates And Why
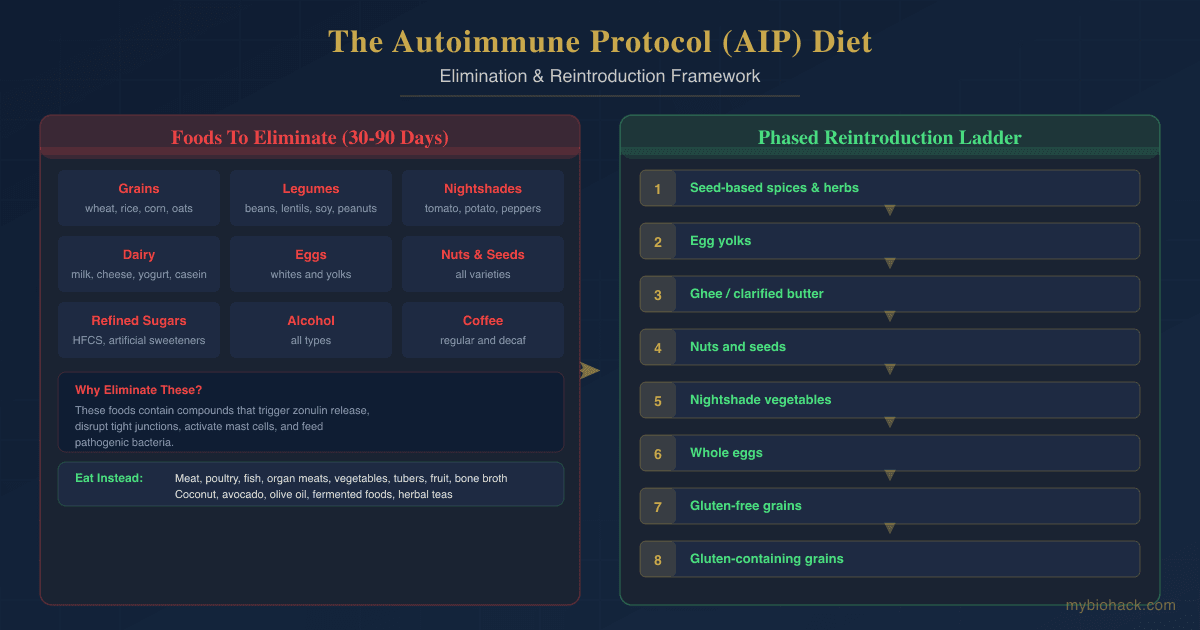
The elimination phase removes the following food categories because they contain compounds that can increase intestinal permeability, activate immune cells, or cross-react with human tissues.

- Grains (wheat, barley, rye, oats, rice, corn, millet, sorghum): Grains contain gluten, prolamines, and lectins that can trigger zonulin release and open intestinal tight junctions. R Gliadin, the gluten protein in wheat, binds to the CXCR3 receptor on intestinal epithelial cells and stimulates zonulin secretion, leading to increased paracellular permeability. R See the post on prolamine intolerance for more detail.
- Legumes (beans, lentils, peanuts, soy, chickpeas, peas): Legumes contain lectins (particularly phytohemagglutinin in raw beans) and saponins that can bind to intestinal microvilli and disrupt gut barrier integrity. R They also contain protease inhibitors that interfere with protein digestion.
- Nightshades (tomatoes, potatoes, eggplant, peppers, goji berries, ashwagandha, spices derived from peppers): Nightshades contain glycoalkaloids (solanine, chaconine, tomatine) that can embed in cholesterol-containing membranes and increase intestinal permeability. R Potato glycoalkaloids have been shown to worsen colonic injury in animal models of inflammatory bowel disease. R Capsaicin in peppers can activate TRPV1 receptors on mast cells and trigger degranulation in susceptible individuals. R
- Dairy (milk, cheese, yogurt, butter, cream, casein, whey): Dairy proteins, particularly A1 beta-casein and whey, are common allergens that can drive IgG and IgE-mediated responses. Lactose malabsorption is also common in autoimmune populations due to intestinal brush border damage. R
- Eggs (whites and yolks): Egg whites contain lysozyme and ovalbumin that can cross the gut barrier and carry other proteins with them. Eggs are among the most commonly identified triggers during AIP reintroduction. R
- Nuts and seeds (all varieties, including tree nuts, peanuts, sesame, sunflower, flax, chia, and seed-based spices): Nuts and seeds contain phytic acid, lectins, and enzyme inhibitors. Many are also common IgE and IgG allergens.
- Refined and processed sugars (white sugar, high-fructose corn syrup, artificial sweeteners, agave): Refined sugars promote dysbiosis by feeding pathogenic bacteria, increase intestinal permeability through multiple pathways, and drive systemic inflammation. R
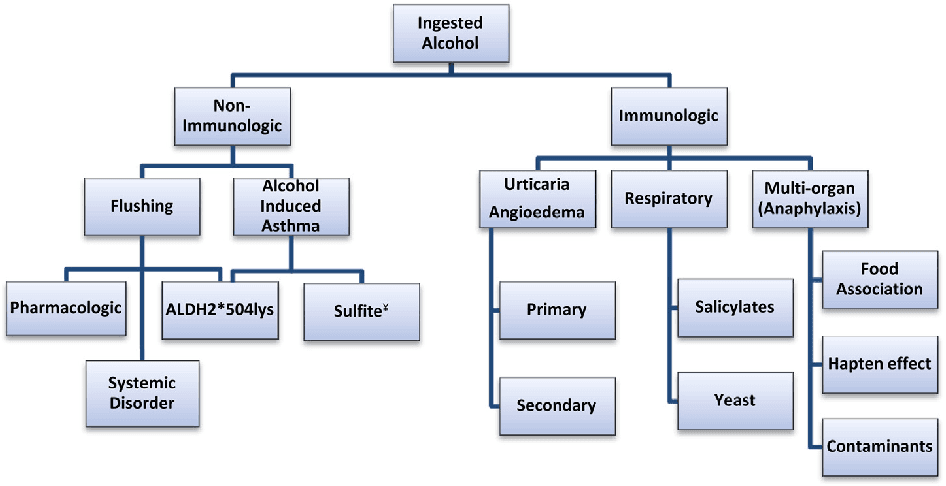
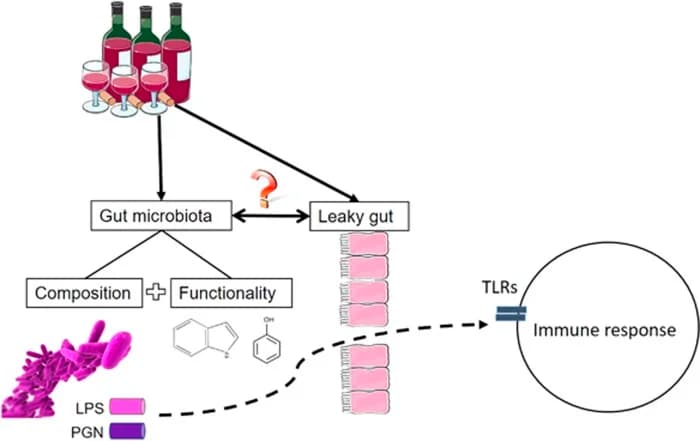
- Alcohol: Alcohol directly damages tight junction integrity, increases endotoxin translocation across the gut barrier, and impairs liver detoxification capacity. R
- Coffee (including regular and decaf): Coffee can increase intestinal permeability in sensitive individuals through its effect on gastric acid secretion and direct irritation of compromised gut mucosa. Many people tolerate coffee well and can reintroduce it.
- Food additives (emulsifiers, thickeners, gums, artificial colors, preservatives, non-nutritive sweeteners): Food additives disrupt the gut microbiome and increase intestinal permeability. Emulsifiers like carboxymethylcellulose and polysorbate-80 have been shown to alter mucus thickness and promote bacterial translocation. R
- NSAIDs (non-steroidal anti-inflammatory drugs): NSAIDs are not a food but are eliminated during AIP because they directly increase intestinal permeability and can trigger flares in IBD and other autoimmune conditions. R
The Elimination Phase
The elimination phase lasts between 30 and 90 days.
The length depends on symptom severity, how quickly the person responds, and how long it takes for baseline symptoms to stabilize.
During this phase, the person eats only AIP-approved foods: high-quality meat, poultry, fish, shellfish, organ meats, bone broth, vegetables (excluding nightshades), sweet potatoes and other tubers, fruits, fermented foods (if tolerated), coconut products, avocados, olive oil, and herbal teas.
The goal is to maximize nutrient density while removing all potential immune triggers.
Organ meats, fatty fish, and bone broth are emphasized because they provide vitamins A, D, K2, zinc, iron, copper, B vitamins, collagen, glycine, and glutamine that support gut barrier repair. R
Fermented vegetables (sauerkraut, kimchi, coconut yogurt, kombucha) are encouraged to support microbiome diversity and short-chain fatty acid production, provided the person tolerates them (some with histamine intolerance or MCAS may need to defer fermentation).
See the post on short-chain fatty acids for more.
It is common for symptoms to worsen transiently in the first one to two weeks as the gut microbiome shifts and dietary histamine or oxalate stores are mobilized.
This is not a sign the diet is wrong.
This is a known adaptation period.
Most people begin noticing improvements in digestive symptoms, joint pain, skin clarity, energy, and brain fog between weeks two and six. R
If there is no improvement after eight weeks of strict elimination, the diet may not be addressing the right triggers, or there may be non-dietary factors (mold exposure, stealth infections, mast cell issues, hormonal dysregulation) that need investigation.
The Reintroduction Phase
Reintroduction is the most important and most overlooked phase of AIP.
Without it, the diet is just a restrictive eating plan that provides no information about which specific foods are problematic for you.
Reintroduction begins once symptoms have stabilized or improved significantly, typically after 30 to 90 days of strict elimination.
Each food is tested individually using a structured protocol.
Day one: Eat a small amount of the test food (about half a teaspoon) and wait 15 minutes.
If no immediate reaction, eat a normal serving.
Then do not eat that food again for five days.
Days two through five: Monitor for delayed reactions including digestive changes, joint pain, skin flares, headaches, fatigue, mood changes, sleep disturbance, brain fog, and changes in preexisting symptoms.
If no reaction occurs by day five, the food can be considered safe and added back into the regular rotation.
If a reaction occurs, wait until symptoms fully resolve (which may take several days), then move on to the next food.
The order of reintroduction matters.
Foods that are less likely to cause reactions should be tested first.
A typical reintroduction sequence is:
Nutrient-dense seed-based spices and herbs first, then egg yolks (separated from whites), then seed-based spices, then ghee or clarified butter, then nuts, then nightshade vegetables starting with peeled and cooked potatoes, then whole eggs, then gluten-free grains starting with white rice, then legumes starting with lentils, then dairy starting with fermented forms like yogurt, then gluten-containing grains last. R
Keep a detailed symptom journal throughout.
Reactions can be subtle and delayed.
If you miss them, you will conclude a food is safe when it is not.
If a food triggers symptoms, eliminate it again and retest it three to six months later after more gut healing has occurred.
Some foods may remain permanently out of reach.
Many people find they can never tolerate gluten or dairy again once autoimmunity is established.
Others tolerate nearly everything except their few personal triggers.
How AIP Works Mechanistically
AIP targets three interconnected systems: intestinal barrier integrity, microbiome composition, and immune tolerance.
Intestinal barrier: The intestinal epithelium is a single-cell layer that separates the gut lumen from the underlying immune tissue.
Tight junction complexes between epithelial cells regulate what passes through.
Gliadin from wheat binds CXCR3 receptors, triggering zonulin release and opening tight junctions. R
Glycoalkaloids from nightshades embed in cell membranes and disrupt barrier function directly. R
Alcohol and NSAIDs cause similar disruption.
By removing all foods that drive barrier opening, AIP allows tight junctions to reseal.
Microbiome: The Western diet promotes dysbiosis by depriving beneficial bacteria of fermentable fibers and feeding pathogenic species with refined sugars and emulsifiers. R
AIP removes the substrates that feed pathogenic bacteria (refined sugar, processed starches, food additives) while increasing fermentable fibers from vegetables and resistant starches from sweet potatoes and tubers.
Fermented foods provide beneficial microbes directly.
Immune tolerance: When dietary antigens cross the gut barrier and enter the submucosa, they encounter dendritic cells, macrophages, and mast cells in the gut-associated lymphoid tissue (GALT).
If the immune system is already primed toward inflammation, these antigens can trigger adaptive immune responses that cross-react with human tissues through molecular mimicry. R
Removing the antigenic load for long enough allows regulatory T cell populations to expand and oral tolerance to be reestablished.
See the post on haptens and food intolerance for more.
Mast cell stabilization: Many foods eliminated in AIP are direct mast cell triggers.
Capsaicin in peppers activates TRPV1 on mast cells, alcohol triggers degranulation, and histamine-rich aged foods add to the total mediator burden.
For patients with mast cell activation syndrome or histamine intolerance, AIP functions similarly to a low-histamine diet by removing the most common degranulation triggers.
See the posts on histamine intolerance vs MCAS and mast cells and neurogenic inflammation for deeper coverage.

AIP And Overlapping Conditions
AIP is relevant to any condition where intestinal permeability, immune dysregulation, or mast cell activation plays a role.
Inflammatory bowel disease: AIP has the strongest evidence base in Crohn's disease and ulcerative colitis, with the Konijeti trial showing 73 percent clinical remission at six weeks. R
Hashimoto's thyroiditis: The Abbott trial and subsequent studies show quality-of-life improvements and some inflammatory marker reductions, though thyroid antibody reductions have been inconsistent. R
Rheumatoid arthritis: A 2026 pilot study found clinically meaningful reductions in RAPID3 and RAID scores over eight weeks on AIP. R
Mast cell activation syndrome and histamine intolerance: AIP eliminates many high-histamine and histamine-liberating foods.
For MCAS patients who react broadly, AIP can serve as a baseline elimination diet before more targeted testing.
See the post on histamine intolerance vs MCAS.
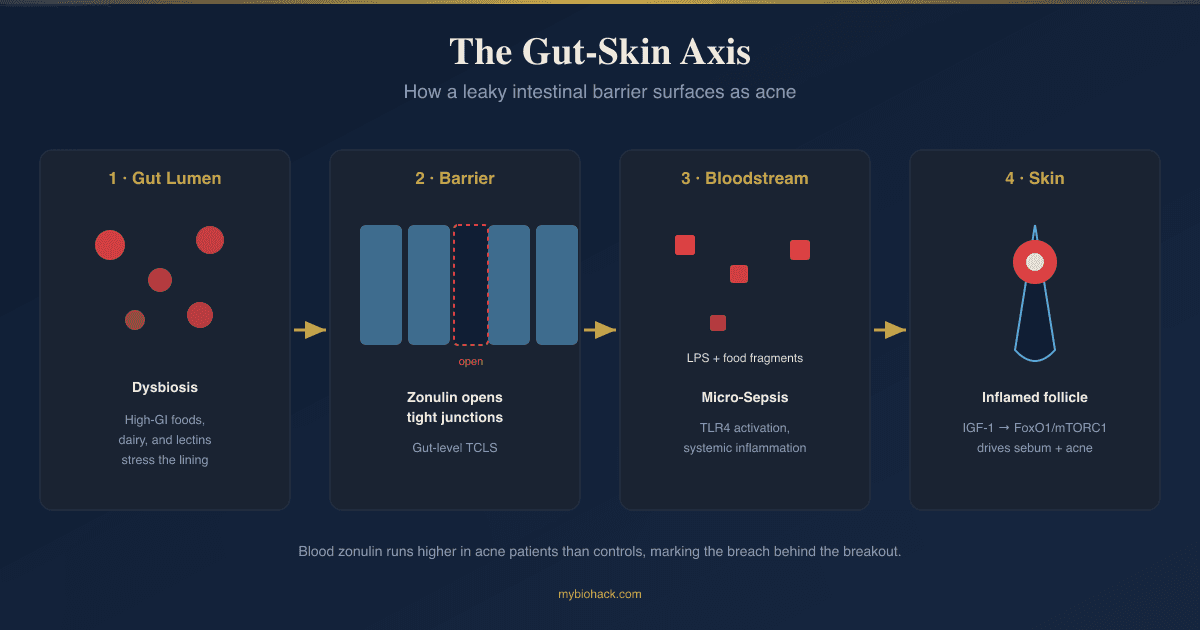
Eczema and atopic dermatitis: The gut-skin axis connects intestinal permeability with skin inflammation.
Removing trigger foods can reduce skin flaring in patients with food-sensitive eczema.
See the posts on eczema and the neuroimmune connection and the gut-skin axis.
Dysbiosis and SIBO: AIP removes the fermentable substrates that feed small intestinal bacterial overgrowth and pathogenic bacteria.
The emphasis on bone broth, collagen, and gut-healing nutrients supports barrier repair.
See the posts on dysbiosis and SIBO.
Psoriasis and psoriatic arthritis: A national survey found that 52 percent of psoriasis patients who tried removing nightshades reported skin improvement or clearance. R
Type 1 diabetes and other autoimmune conditions: The zonulin-mediated mechanism is not disease-specific.
Any condition driven by intestinal permeability and molecular mimicry could theoretically respond to AIP, though condition-specific trials are largely lacking. R
Contrast With The Low-Lectin Diet
The low-lectin diet and AIP share the goal of removing dietary antigens that trigger immune activation.
AIP is broader, removing entire food categories (grains, legumes, nightshades, dairy, eggs, nuts, seeds) for a defined period, then testing each individually.
The low-lectin diet specifically targets lectin-containing foods but allows many foods that AIP restricts (eggs, nuts, seeds, coffee, chocolate).
For most autoimmune patients, AIP offers a more rigorous starting point because it casts a wider net and provides a clearer signal during reintroduction.
See the full post on the low-lectin diet for comparison.
Testing Before Starting
Before starting AIP, baseline testing helps identify contributing factors that may need parallel intervention.
Blood And Urine Markers
High-sensitivity C-Reactive Protein (hs-CRP): measures systemic inflammation and provides a baseline to track diet response.
I use the Cardio Zoomer to assess this alongside lipid and metabolic markers.
Comprehensive Metabolic Panel (CMP): evaluates liver and kidney function, electrolyte balance, and fasting glucose.
This is included in the Foundation Zoomer.
Complete Blood Count (CBC) with differential: screens for anemia, infection, and immune cell distribution.
Included in the Foundation Zoomer.
Thyroid Panel (TSH, Free T3, Free T4, TPO antibodies, thyroglobulin antibodies): essential baseline for anyone with autoimmune thyroid disease.
I use the Foundation Zoomer for the core thyroid markers.
Fasting Insulin and HOMA-IR: assesses metabolic health and insulin resistance, which frequently coexists with autoimmune inflammation.
I use the Cardio Zoomer to evaluate these markers.
Functional Lab Panels
I use the Gut Zoomer to assess microbiome composition, pathogenic bacteria, parasites, yeast, digestive function, and intestinal permeability markers (zonulin) before starting an elimination diet.
I use the Food Zoomer to identify existing IgG and IgA food sensitivities across 200 foods.
This panel can guide which foods to prioritize during reintroduction.
I use the Immune Zoomer to assess systemic autoantibodies, mast cell markers (tryptase, histamine), and organ-specific immune reactivity.
I use the Toxin Zoomer when mold or heavy metal exposure is suspected, as biotoxin illness can prevent response to dietary intervention.
Genetics
I use the Methylation Genetics panel to evaluate variants in MTHFR, COMT, and related genes that affect detoxification and immune regulation.
Elimination Testing
The AIP diet itself is the primary elimination test.
If the diet produces clear improvement, the reintroduction phase is where the diagnostic information lives.
If the diet produces no improvement after eight to twelve weeks of strict adherence, consider stool testing for pathogens and digestive function, organic acids testing for mitochondrial and metabolic function, and assessment for mold illness or stealth infections.
Mechanisms Of Action
Simple:
AIP removes foods that damage the gut lining, feed pathogenic bacteria, or directly activate immune cells, then floods the body with nutrient-dense foods that support tissue repair.
This gives the intestinal barrier a chance to heal and the immune system a chance to reset its tolerance settings.
Advanced:
- Zonulin inhibition: Gliadin and other food antigens bind CXCR3 on enterocytes, triggering zonulin secretion and tight junction disassembly. Eliminating these antigens removes the signal that drives paracellular permeability. R
- Glycoalkaloid-induced membrane permeabilization: Solanine and chaconine from nightshades embed in cholesterol-containing membranes, creating pores that increase permeability independent of tight junction regulation. AIP removes these membrane-active compounds. R
- Microbiome substrate removal: Refined sugars and processed starches feed pathogenic bacteria like Clostridium difficile, Klebsiella, and Proteus species that produce pro-inflammatory metabolites and lipopolysaccharides. AIP removes these substrates and replaces them with fermentable fibers that promote Bifidobacterium, Lactobacillus, and Faecalibacterium prausnitzii populations that produce short-chain fatty acids. R
- Mast cell mediator reduction: Dietary histamine, histamine liberators (egg white, shellfish, alcohol, nightshade alkaloids), and TRPV1 agonists (capsaicin) directly trigger mast cell degranulation. Removing these inputs reduces total mast cell mediator burden and stabilizes degranulation threshold. R
- Molecular mimicry interruption: Food proteins, including gliadin, casein, and ovalbumin, share peptide sequences with human tissues (thyroid peroxidase, synovial tissue, cerebellar tissue). Removing these antigens eliminates the cross-reactive stimulus that sustains autoimmune attack. R
- Regulatory T cell expansion: Prolonged antigen removal in the presence of high-nutrient-density foods (vitamin A, vitamin D, zinc, short-chain fatty acids) supports the expansion of FoxP3+ regulatory T cells in gut-associated lymphoid tissue, restoring oral tolerance mechanisms. R
- Butyrate-mediated barrier repair: Resistant starches from AIP-approved tubers and vegetables are fermented by beneficial bacteria into butyrate, the primary fuel for colonocytes. Butyrate upregulates tight junction protein expression (occludin, claudin-1, ZO-1) and reduces paracellular permeability. R
Genetics
The success of AIP depends partly on genetic variants that affect immune regulation, detoxification, and food antigen sensitivity.
HLA-DQ2 AND HLA-DQ8
The HLA-DQ genes encode MHC class II molecules that present dietary antigens to T cells.
HLA-DQ2 (encoded by DQA1*05 and DQB1*02) is present in approximately 90 percent of celiac disease patients. R
HLA-DQ8 is present in most of the remaining 5 to 10 percent.
These same HLA haplotypes increase risk for non-celiac gluten sensitivity and other autoimmune conditions.
Carrying HLA-DQ2 or HLA-DQ8 means your immune system is genetically programmed to mount a response against gluten-derived peptides, making strict gluten elimination essential.
AIP eliminates gluten regardless of HLA status, but individuals with these variants are far more likely to need permanent gluten avoidance.
Nearly all autoimmune patients have at least one HLA-DQ risk variant, though testing is not widely done outside of celiac diagnosis.
PTPN22
The PTPN22 gene encodes a tyrosine phosphatase that regulates T cell receptor signaling.
The R620W variant (rs2476601) is one of the strongest non-HLA genetic risk factors for autoimmune disease, associated with rheumatoid arthritis, type 1 diabetes, Hashimoto's thyroiditis, Graves' disease, and systemic lupus erythematosus. R
This variant reduces the threshold for T cell activation, meaning dietary antigens are more likely to trigger adaptive immune responses.
Carriers may benefit more aggressively from dietary antigen removal.
MTHFR
MTHFR encodes methylenetetrahydrofolate reductase, a rate-limiting enzyme in the folate cycle that provides methyl groups for methylation, detoxification, and neurotransmitter synthesis.
The C677T variant (rs1801133) reduces enzyme activity by 40 percent in heterozygotes and 70 percent in homozygotes. R
Reduced methylation capacity impairs liver phase I and phase II detoxification, which can increase the body's sensitivity to dietary antigens and environmental toxins.
MTHFR variants are also linked to elevated homocysteine, which drives systemic inflammation.
FUT2
The FUT2 gene encodes fucosyltransferase 2, which determines secretor status and influences the gut microbiome composition.
Non-secretor status (rs601338) is associated with altered gut microbiome composition, increased intestinal permeability, and higher risk for Crohn's disease and type 1 diabetes. R
Non-secretors may have a harder time maintaining a healthy microbiome during AIP elimination and may benefit more from targeted probiotic and prebiotic support.
NOD2
NOD2 encodes an intracellular pattern recognition receptor that detects bacterial peptidoglycan fragments and activates immune responses.
Loss-of-function variants (rs2066844, rs2066845, rs5743293) are strongly associated with Crohn's disease and impair the ability to clear intracellular bacteria. R
Carriers may have chronically upregulated gut inflammation that requires more aggressive dietary intervention and longer elimination phases to see improvement.
More Research
AIP in multiple sclerosis: The Wahls Protocol, which shares significant overlap with AIP and adds extreme vegetable intake for mitochondrial support, has shown benefit in small MS trials.
No AIP-specific trial in MS has been published, though Dr. Terry Wahls' work in this area uses a modified AIP template. R
AIP in systemic lupus erythematosus: No controlled trials exist for AIP in lupus, though case reports and clinical observations suggest benefit.
The anti-inflammatory and gut-healing framework is theoretically applicable, but the lack of data means any recommendation is extrapolation.
AIP in psoriasis: Survey data suggests nightshade elimination benefits roughly half of psoriasis patients who try it, but no controlled dietary intervention trial has been published. R
AIP and long COVID: The AIP framework may benefit post-viral patients with gastrointestinal symptoms and systemic inflammation, but no studies exist.
Given the overlap between long COVID and MCAS, the mast cell stabilizing effects of AIP may be particularly relevant.
AIP in food allergy: A 2026 review explored AIP as a potential framework for food allergy management given its elimination of the most common allergens, but this remains theoretical pending clinical trials. R
AIP and the oral microbiome: Most AIP research focuses on the gut microbiome, but dietary changes also alter oral microbial composition, which influences nitric oxide production and systemic immune tone through the oral-gut axis.
This is an area needing more research.
Nutrient risks of prolonged elimination: AIP eliminates entire food groups that provide important nutrients.
Calcium, vitamin D, B vitamins, and fiber intake can drop significantly if the diet is not carefully planned.
Prolonged time in the elimination phase (beyond 90 days without medical supervision) increases the risk of nutrient deficiencies.
Working with a practitioner is recommended for anyone with a history of eating disorders or nutrient malabsorption.
For biomarker testing I use the Gut Zoomer to assess intestinal permeability (zonulin) and microbiome composition, the Food Zoomer to identify existing food sensitivities, and the Immune Zoomer to evaluate mast cell and autoimmune markers before starting dietary intervention.
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Quercetin
500mg 2x/day
Vitamin D3 + K2
5000 IU + 200mcg/day
DAO Enzyme
1 cap before meals