SIBO (Small Intestinal Bacterial Overgrowth): Root Causes, Testing, And Evidence-Based Treatment
By Jacob Gordon, INHC, FMT-CThis article contains affiliate links. As an Amazon Associate, MyBioHack earns from qualifying purchases at no extra cost to you. We only link products we research and stand behind.
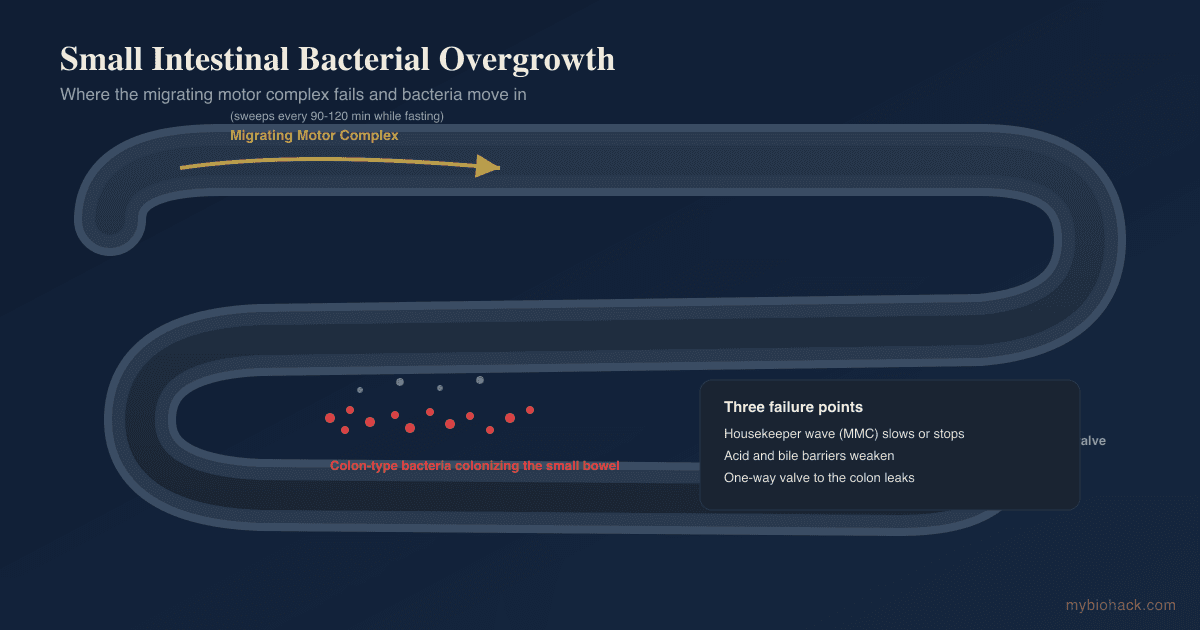
Small Intestinal Bacterial Overgrowth (SIBO) is a condition where bacteria that belong in the colon colonize the small intestine, where they ferment food too early and drive bloating, pain, and altered bowel habits.
In this post, we will discuss what SIBO actually is at a mechanistic level, why it keeps coming back, the three gas subtypes, why standard breath testing is imperfect, the root causes beyond antibiotics, and an evidence-based approach to treatment.

Basics Of SIBO
SIBO is defined as an excessive number of bacteria in the small intestine that produces gastrointestinal symptoms. R
The small intestine is not sterile, but it normally carries far fewer bacteria than the colon, and those bacteria are mostly different species. R
When colon-type bacteria migrate upstream and set up residence in the small bowel, they meet your food before you have finished digesting and absorbing it.
They ferment carbohydrates in the wrong place, producing gas, drawing water into the lumen, and generating byproducts that damage the brush border and the intestinal lining.
The classic symptoms are bloating within an hour or two of eating, abdominal distension, gas, cramping, and either diarrhea or constipation depending on the dominant organisms.
Because the overgrowth interferes with absorption, longstanding SIBO can also cause deficiencies in fat-soluble vitamins, iron, and B12, along with unintended weight changes. R
The single most important thing to understand is that SIBO is almost always a downstream problem, not a primary infection.
It is a signpost pointing at a failure of one of the mechanisms that is supposed to keep the small intestine clean, which is why antibiotics alone so often produce only temporary relief.
The Three Subtypes: Hydrogen, Methane, And Hydrogen Sulfide
Not all SIBO is the same, and the dominant gas produced by the overgrowth predicts both the symptom pattern and the response to treatment.
Hydrogen-dominant SIBO is driven by fermenting bacteria that release hydrogen gas, and it tends to present with diarrhea, urgency, and bloating.
Methane-dominant overgrowth is now formally called Intestinal Methanogen Overgrowth (IMO), because the organisms responsible are not bacteria at all. R
They are archaea, most often Methanobrevibacter smithii, and they consume hydrogen produced by other microbes and convert it to methane. R
Methane slows intestinal transit, which is why IMO is tightly associated with constipation, and the degree of methane elevation correlates with the severity of constipation. R
Because methanogens can colonize the entire gut and not just the small bowel, IMO is technically a broader term than SIBO.
Hydrogen sulfide SIBO is the most recently characterized subtype, driven by sulfate-reducing organisms such as Desulfovibrio that consume hydrogen and produce hydrogen sulfide gas.
Elevated breath hydrogen sulfide correlates with diarrhea-predominant symptoms and with a higher relative abundance of sulfide-producing bacteria. R
This subtype was invisible to older two-gas breath tests, so a subset of patients who "tested normal" for years actually had a sulfide-driven overgrowth the whole time.

Knowing your subtype matters because methane responds to different antimicrobials than hydrogen, and sulfide overgrowth responds to reducing sulfur load in the diet.
What Causes SIBO
SIBO is a consequence of a broken defense mechanism, and identifying which one is broken is the entire game.
The most common and most overlooked driver is impaired motility of the small intestine, specifically loss of the cleansing wave called the Migrating Motor Complex (MMC), which is covered in detail in the next section.
Root causes of SIBO (not an exclusive list):
- Adhesions and structural obstruction from prior abdominal surgery, endometriosis, or Crohn's strictures that create pockets of stasis
- Bile insufficiency from gallbladder removal or cholestasis, since bile acids are directly antimicrobial in the small bowel
- Hypochlorhydria (low stomach acid), often from chronic acid-suppressing medication, which removes the acid barrier that sterilizes incoming food R
- Ileocecal valve dysfunction, where the one-way gate between the small intestine and colon fails and allows colonic bacteria to reflux upstream
- Impaired migrating motor complex from post-infectious autoimmunity, diabetes, hypothyroidism, or opioid use
- Pancreatic enzyme insufficiency, which leaves undigested substrate in the lumen for bacteria to ferment R
The post-infectious pathway deserves special attention because it explains a large fraction of cases that seem to come out of nowhere.
After a bout of food poisoning, the immune system produces antibodies against a bacterial toxin called cytolethal distending toxin B (CdtB).
Through molecular mimicry, those antibodies cross-react with vinculin, a protein your own gut nerve cells use, and the resulting autoimmune damage impairs the migrating motor complex. R
This is why so many people trace their SIBO back to a single memorable case of traveler's diarrhea or food poisoning.
Underlying dysbiosis in the colon also raises the baseline pressure of bacteria trying to migrate upstream, which is why gut health upstream and downstream of the small intestine both matter.
How The Small Intestine Keeps Itself Clean
The small intestine has a layered defense system, and SIBO is what happens when enough of those layers fail at once.
The migrating motor complex is the master defense.
It is a wave of coordinated muscular contractions that sweeps through the stomach and small intestine roughly every 90 to 120 minutes during fasting, physically clearing residual food, debris, and bacteria toward the colon. R
It has been called the intestinal housekeeper, and Phase III of the complex is the powerful sweeping contraction that does most of the cleaning.
The critical evidence linking the MMC to SIBO is old but definitive.
Patients with bacterial overgrowth were shown decades ago to have an absent or disordered migrating motor complex, and disrupting the MMC experimentally is enough to produce overgrowth on its own. R
The MMC only runs when you are fasting, and it is suppressed every time you eat, which is why constant snacking is quietly one of the worst habits for someone prone to SIBO. R
Stomach acid is the second layer, sterilizing most of what you swallow before it reaches the small intestine, which is why suppressing acid raises overgrowth risk. R
Bile and pancreatic secretions are the third layer, since bile acids are antimicrobial and enzymes prevent undigested food from feeding bacteria. R
The ileocecal valve is the fourth layer, acting as a one-way gate that keeps the dense colonic population from washing back into the small bowel.
The gut immune system, including secretory IgA and the intestinal lining itself, is the final layer, and once bacterial products like lipopolysaccharide accumulate they can inflame and loosen the barrier further.
When the housekeeper stops sweeping, the acid barrier is down, and the valve leaks, bacteria have every advantage, and SIBO becomes self-sustaining.

SIBO And Overlapping Conditions
SIBO rarely travels alone, and its comorbidities are a clue to shared underlying mechanisms.
Conditions that overlap with SIBO (not an exclusive list):
- Diabetes and hypothyroidism, both of which slow gut motility and impair the migrating motor complex
- Ehlers-Danlos syndrome and hypermobility, where connective tissue laxity contributes to dysmotility, and SIBO prevalence runs high in this group R
- Gastroparesis and chronic constipation, which share the motility deficit at the root of SIBO
- Histamine intolerance and mast cell issues, since overgrowth feeds histamine production and barrier disruption, discussed in histamine intolerance versus MCAS
- Irritable bowel syndrome, where a large fraction of cases show abnormal breath tests and post-infectious autoimmunity R
- Rosacea and skin conditions tied to intestinal permeability and zonulin
- Scleroderma and connective tissue disease, the textbook example of severe dysmotility-driven overgrowth
The thread running through most of these is motility.
Anything that damages the nerves or muscle of the gut, whether autoimmune, metabolic, or structural, tends to allow overgrowth downstream.
This is also why chasing the bacteria without addressing the comorbid driver produces relapse after relapse.
Why Standard Breath Testing Is Imperfect
Breath testing is the most widely used SIBO test, and it is genuinely useful, but you should understand its real limitations before you put too much weight on a single result.
The test works by having you drink a sugar substrate, usually lactulose or glucose, and then measuring hydrogen and methane in your breath at intervals, since those gases come only from bacterial fermentation. R
The problem is accuracy.
A meta-analysis of breath testing found the lactulose breath test had a pooled sensitivity of only 42 percent and specificity of 71 percent, while the glucose breath test reached 55 percent sensitivity and 83 percent specificity. R
In plain terms, a normal breath test does not rule SIBO out, and the two substrates disagree with each other often enough to matter.
Glucose is absorbed quickly in the upper small intestine, so it can miss overgrowth further downstream, producing false negatives.
Lactulose travels the whole length of the small bowel, but because it eventually reaches the colon, a fast transit time can produce a false positive when the gas rise is really just the substrate hitting the colon early.
There is a big MAYBE built into every breath test, and this is why interpretation should always be anchored to symptoms and pretest probability, not the number alone.
The older tests also measured only hydrogen and methane, missing the hydrogen sulfide subtype entirely, though newer three-gas devices have closed that gap. R
The gold standard, a direct culture of small bowel fluid, has its own problems, since only a minority of gut bacteria grow in culture and the sample is easily contaminated on the way out.
The honest position is that no SIBO test is definitive, so treat the test as one input alongside history, subtype, and response to treatment.
How To Improve SIBO
The evidence-based approach to SIBO has three parts that must all happen or the overgrowth returns: reduce the bacterial load, remove the fuel temporarily, and restore the defense that failed.
Skipping the third step is the single most common reason SIBO relapses within months.
1. Reduce The Bacterial Load
Rifaximin is the best-studied antibiotic for hydrogen-dominant SIBO, and it is a reasonable first-line choice because it stays almost entirely in the gut with minimal systemic absorption.
A meta-analysis found an overall eradication rate around 70 percent by breath test, with a low adverse event rate, though the underlying studies are of modest quality. R
Methane-dominant overgrowth responds better to rifaximin combined with a second agent that targets archaea, since methanogens resist rifaximin alone. R R
Rifaximin is a prescription, so this is a conversation to have with a physician, and you can reach out through the consultation page if you want help building a plan.
Herbal antimicrobials are a legitimate alternative for people who cannot or prefer not to use antibiotics.
A study at Johns Hopkins found herbal antimicrobial protocols achieved breath test normalization at rates statistically equivalent to rifaximin. R
The herbal agents with the most support are combined into standard protocols, alphabetically:
Allicin: Stabilized garlic extract, valued particularly for methane-dominant overgrowth.
Berberine: A plant alkaloid with broad antimicrobial activity that is one of the two best-supported botanicals for SIBO, available as a berberine supplement.
Neem: A traditional antimicrobial with preclinical support, often rotated with other botanicals.
Oregano oil: A potent antimicrobial, the other most-studied botanical alongside berberine.
Biofilms can shelter bacteria from both antibiotics and herbs, which is one reason overgrowth is stubborn, and disrupting them is covered in the post on inhibiting biofilms.
2. Remove The Fuel
Fermentable carbohydrates are what the overgrowth eats, so restricting them starves the bacteria and calms symptoms while you treat.
A low FODMAP diet ranks first among dietary strategies for improving global IBS symptoms, abdominal pain, and bloating in network meta-analysis, and it overlaps heavily with SIBO management. R
Low FODMAP is a temporary therapeutic tool, not a permanent diet, because long-term restriction starves your beneficial Bifidobacteria and reduces microbial diversity.
For the hydrogen sulfide subtype, additionally lowering high-sulfur foods often produces faster relief than FODMAP restriction alone.
The most aggressive option is an elemental diet, a predigested formula absorbed high in the small intestine that leaves almost nothing for bacteria downstream.
A 14-day elemental diet normalized the lactulose breath test in roughly 80 percent of subjects, with a further 5 percent normalizing by day 21. R
Elemental formulas are demanding to tolerate, so most people use them as a two-week reset rather than a lifestyle, and a ready-made elemental diet formula makes it more practical.
3. Restore The Defense That Failed
This is the step that determines whether you stay well.
If motility is the driver, a prokinetic taken at night supports the migrating motor complex during the fasting window and is the mainstay of relapse prevention.
Prescription prokinetics like low-dose prucalopride or erythromycin are the strongest options, and natural agents include ginger and melatonin, which supports gut motility beyond its role in sleep. R
Space your meals four to five hours apart and stop snacking, because every bite shuts the housekeeper off and constant grazing is a self-inflicted cause of relapse.
If low stomach acid is the driver, betaine HCl with meals can restore the acid barrier, though it should be avoided if you have active gastritis or ulcers.
If bile or enzyme insufficiency is the driver, digestive enzymes and bile support such as TUDCA address the missing antimicrobial secretions.
Once the overgrowth is cleared and the defense is restored, the rebuilding phase reintroduces fermentable fiber and beneficial organisms to restore diversity.
This is where resistant starch, short chain fatty acids like butyrate, and targeted Lactobacillus and Bifidobacteria strains come back in, slowly.
For severe, refractory dysbiosis underneath the overgrowth, fecal microbiota transplantation is an emerging option, though it is not a first-line SIBO treatment. R
What To Stay Away From
Some common habits and interventions actively feed SIBO or blunt the defenses you are trying to rebuild.
Things to avoid or minimize with SIBO (not an exclusive list):
- Constant snacking and grazing, which suppresses the migrating motor complex all day
- High-dose probiotics during active overgrowth, which can worsen bloating in some people until the load is reduced (reintroduce them in the rebuilding phase)
- Long-term acid-suppressing drugs where not strictly necessary, given the link between acid suppression and overgrowth, discussed in proton pump inhibitors and the gut R R
- Opioids and unnecessary anticholinergics, which slow gut motility directly
- Permanent ultra-restrictive dieting, which starves beneficial bacteria and reduces diversity
- Sugar alcohols and excess fermentable fiber during the active phase, which are direct fuel for the overgrowth
The overarching principle is to avoid anything that either feeds the bacteria or turns off the housekeeper.
Testing
Testing for SIBO has two goals: confirm the overgrowth and its subtype, and find the root cause driving it.
Breath Testing And Subtyping
The three-gas breath test is the most complete option because it captures the hydrogen sulfide subtype that older tests miss.
I use the trio-smart SIBO Breath Test (Gemelli Biotech) to measure hydrogen, methane, and hydrogen sulfide together, which is the only way to identify all three subtypes in one test. R
For a classic two-gas lactulose approach, the SIBO Test (3-Hour) or the shorter SIBO Test (2-Hour) (Genova Diagnostics) measure hydrogen and methane across the small bowel transit.
Interpret every breath test against symptoms and pretest probability, because sensitivity is modest and a normal result does not rule SIBO out. R
Root Cause And Post-Infectious Markers
To identify the post-infectious autoimmune driver, I use the ibs-smart (Gemelli Biotech) blood test, which measures anti-CdtB and anti-vinculin antibodies. R
Positive antibodies point to migrating motor complex damage from a prior gut infection, which changes the plan toward long-term prokinetic support.
Comprehensive Gut And Barrier Panels
To assess the colonic dysbiosis, pathogens, and barrier integrity underneath the overgrowth, I use the Gut Zoomer (Vibrant Wellness), which profiles the microbiome, permeability markers like zonulin, and digestion.
For a PCR-based stool alternative, the GI-MAP (Diagnostic Solutions) quantifies pathogens, commensals, and methanogens including Methanobrevibacter smithii.
To directly measure the leaky barrier that often accompanies SIBO, the Intestinal Permeability Assessment (Genova Diagnostics) uses the lactulose to mannitol ratio.
Mechanisms Of Action
Simple:
- SIBO happens when the wave that sweeps your small intestine clean between meals slows down and lets colon bacteria move in and stay.
- Those bacteria ferment your food too early, producing gas that causes bloating, and byproducts that inflame the gut lining.
- Methane gas from archaea slows the gut and causes constipation, while hydrogen and hydrogen sulfide gases speed it up and cause diarrhea.
Advanced:
- Migrating motor complex failure. The MMC is a cyclical interdigestive motor pattern regulated by motilin and the enteric nervous system, and its Phase III sweeping contractions clear luminal contents toward the colon roughly every 90 to 120 minutes during fasting. R Loss of the MMC, whether from autoimmune neuropathy, diabetic vagal damage, or opioid receptor activation, removes the primary mechanical clearance of the small bowel and permits colonization. R
- Molecular mimicry and anti-vinculin autoimmunity. After enteric infection with organisms expressing cytolethal distending toxin, anti-CdtB antibodies cross-react with vinculin, a cytoskeletal adhesion protein expressed by interstitial cells of Cajal, the pacemaker cells that generate the MMC. R The resulting loss of interstitial cell of Cajal function degrades motility and sustains overgrowth.
- Interspecies hydrogen transfer. Fermenting bacteria produce hydrogen, and methanogenic archaea such as Methanobrevibacter smithii and sulfate-reducing bacteria such as Desulfovibrio consume that hydrogen, producing methane and hydrogen sulfide respectively. R Methane acts as a neuromuscular slowing signal that prolongs transit and drives constipation, while hydrogen sulfide is cytotoxic to colonocytes and associates with diarrhea. R R
- Loss of chemical barriers. Gastric acid, bile acids, and pancreatic enzymes together sterilize and clear incoming contents, so hypochlorhydria from acid suppression measurably raises overgrowth risk by removing the proximal chemical barrier. R
Genetics
SIBO is not a monogenic disease, but host genetics shape susceptibility through motility, connective tissue, and immune targets.
VCL
VCL encodes vinculin, a cytoskeletal protein that anchors cell-to-cell and cell-to-matrix junctions, including in the interstitial cells of Cajal that pace the migrating motor complex.
In post-infectious SIBO, autoantibodies raised against bacterial CdtB cross-react with vinculin, and higher anti-vinculin levels track with more severe symptoms. R
This is an acquired autoimmune hit on a structural gene product rather than an inherited VCL mutation, but it explains the durable motility damage after food poisoning.
COL genes (connective tissue)
Collagen genes underlie the heritable connective tissue disorders, and defects in them produce joint hypermobility and Ehlers-Danlos syndrome.
Connective tissue laxity contributes to gastrointestinal dysmotility, and SIBO prevalence is elevated in hypermobile and Ehlers-Danlos populations. R
This is why unexplained recurrent SIBO in a flexible, easily bruised patient should prompt a look at the connective tissue picture.
More Research
Antibiotic resistance and rifaximin deserves ongoing attention, because although rifaximin has a favorable resistance profile compared with systemic antibiotics, repeated courses without addressing the root cause are still not a durable strategy. R
Breath test standardization remains unsettled, since substrate choice, cutoffs, and transit time all shift results, and clinicians still disagree on the best protocol, which is why interpretation matters as much as the raw number. R
Elemental diet as a non-antibiotic reset is a striking finding that remains underused, given how effective a two-week formula was at normalizing the breath test, and it is worth considering for antibiotic-intolerant patients. R
Herbal versus antibiotic equivalence rests largely on a single retrospective study, so while promising, it should not yet be read as settled science, and better randomized trials are underway. R
Hydrogen sulfide as a distinct subtype is a genuinely new axis of understanding, and three-gas testing is reclassifying patients who were told for years that their tests were normal. R
For biomarker and subtype testing I use the trio-smart SIBO Breath Test and the ibs-smart to separate the mechanical from the autoimmune drivers, and you can track your labs, symptoms, and treatment response over time in the Health Hub with a Pro membership.
If you want a deeper look at how the gut barrier and bacterial byproducts drive systemic symptoms, the post on MCT oil types and the piece on Akkermansia muciniphila cover the rebuilding side, and dysbiosis covers the colonic foundation underneath it all.
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Spore-Based Probiotics
1 cap with food
L-Glutamine
5g 2x/day on empty stomach
Butyrate
300mg 2x/day with meals