Hyperbaric Oxygen Therapy (HBOT): Mechanisms, Benefits, And Protocols For Chronic Illness
By Jacob Gordon, INHC, FMT-CHyperbaric oxygen therapy is a treatment modality in which 100% oxygen is administered at an atmospheric pressure greater than 1 ATA, resulting in a five- to twenty-fold increase in dissolved plasma oxygen that reaches tissues bypassing hemoglobin-dependent delivery.
In this post, we will discuss how HBOT works mechanistically, what distinguishes hard from soft chambers, which conditions have the strongest clinical evidence, Jacob's preferred protocols for the chronic illness population, safety considerations including the oxidative stress risk, and the relevant genetics.

Basics Of HBOT
Hyperbaric oxygen therapy (HBOT) involves breathing near-100% oxygen inside a sealed chamber that is pressurized above one atmosphere absolute (ATA).
HBOT is relevant to anyone working with mitochondrial psychobiology, because the therapy directly targets the oxygen-sensing and energy-production pathways that go awry in chronic illness.
At sea level, the oxygen dissolved in plasma accounts for roughly 0.3 mL of oxygen per 100 mL of blood, while hemoglobin carries the bulk. R
Under HBOT at 2.0 ATA, dissolved plasma oxygen rises to approximately 4.4 mL per 100 mL, and at 2.5 ATA it reaches about 5.6 mL per 100 mL. R
This is governed by Henry's Law, which states that the amount of gas dissolved in a liquid is proportional to its partial pressure above that liquid.
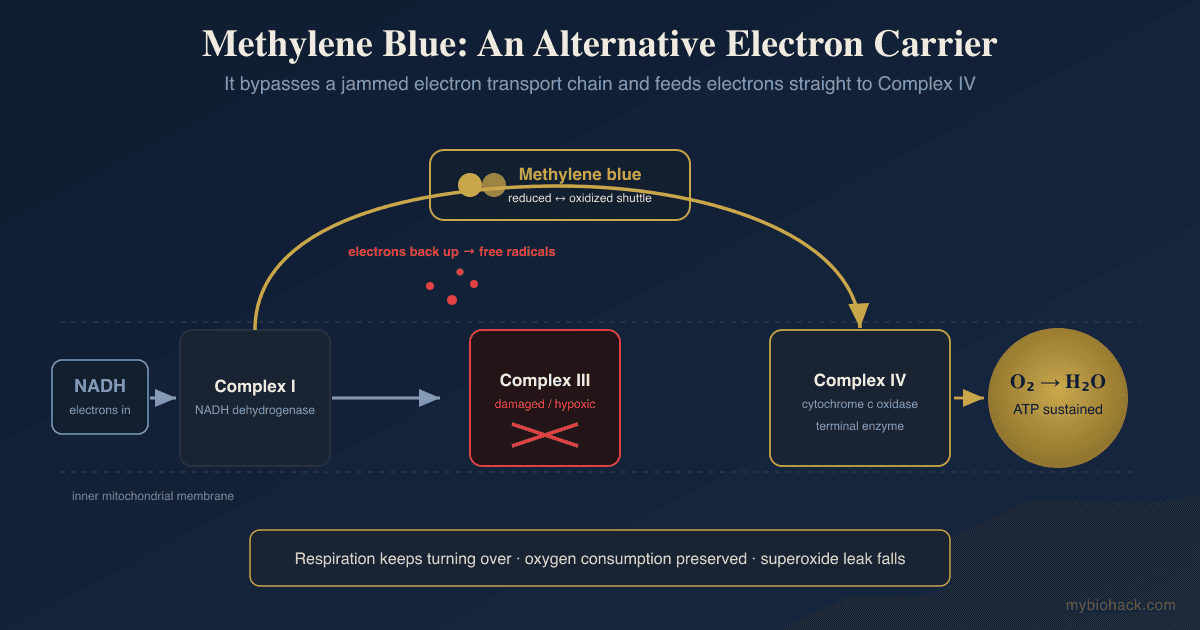
HBOT's mechanism parallels what happens with methylene blue at the mitochondrial level, where oxygen utilization is improved rather than oxygen delivery alone.
The physiological importance is that oxygen can now reach hypoxic tissues even when hemoglobin is fully saturated or when microvascular flow is compromised.
This is fundamentally different from normobaric oxygen therapy (oxygen at 1 ATA), which cannot achieve the same tissue penetration because the pressure component is absent. R
The hormetic nature of HBOT overlaps with what I cover in red light therapy, where the dose ceiling and the individual's redox capacity determine whether a therapy is beneficial or harmful.
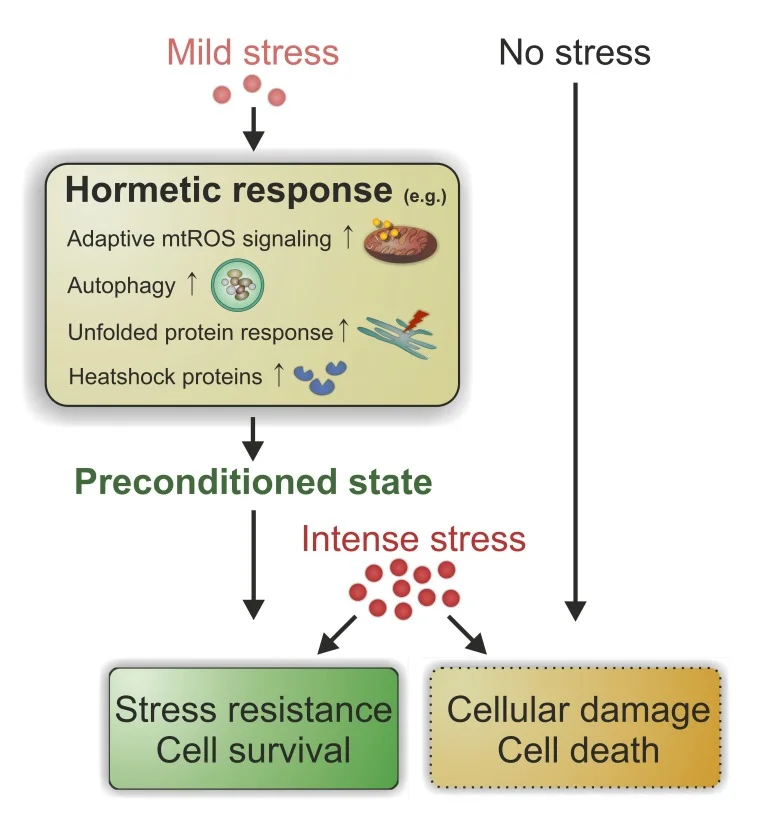
HBOT also provides an intermittent hyperoxic stimulus that triggers adaptive cellular signaling cascades, a phenomenon sometimes called the hyperoxic-hypoxic paradox. R
What HBOT Does Mechanistically
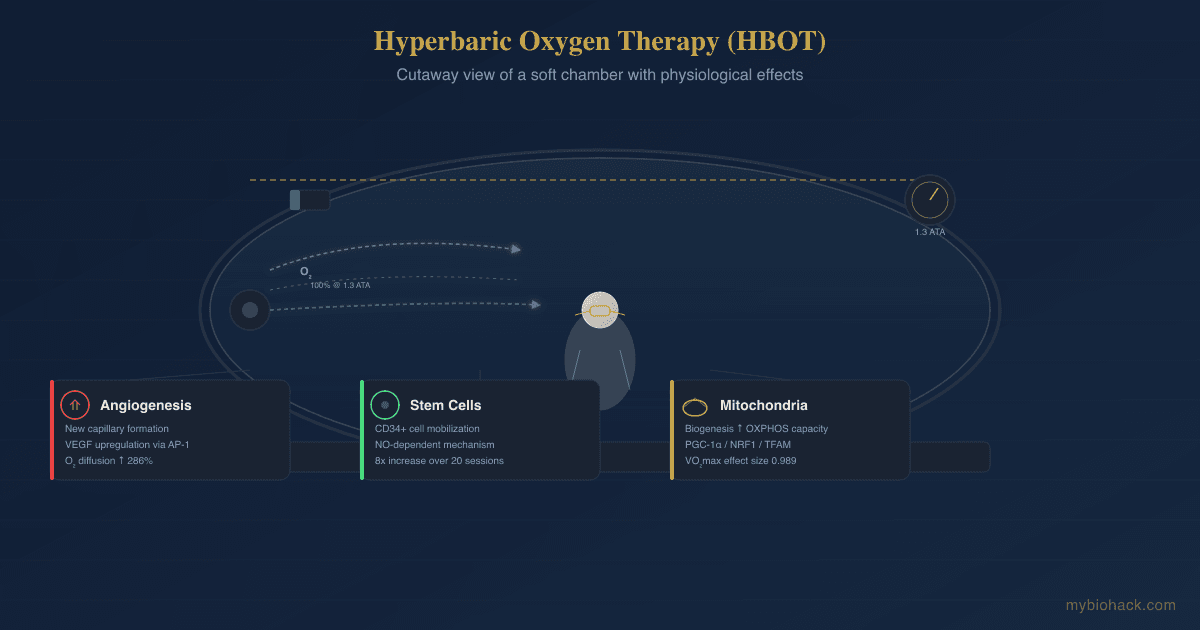
HBOT increases the oxygen diffusion gradient between healthy capillary blood and hypoxic tissue, widening the effective diffusion distance by up to 286%. R
This allows oxygen to reach cells that have become metabolically dormant due to inadequate perfusion.
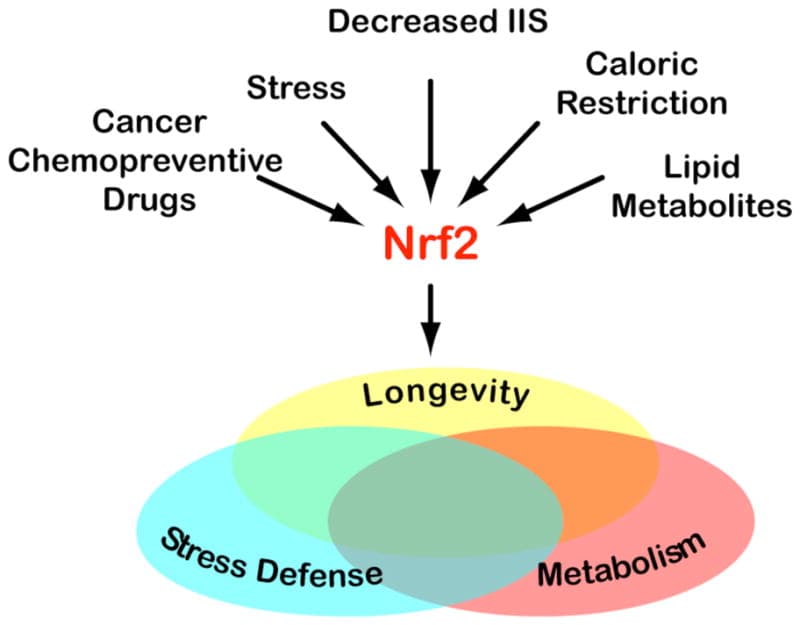
The transient hyperoxia generates a controlled burst of reactive oxygen species (ROS) that, in a competent redox system, upregulates antioxidant response enzymes (AREs) and transcription factors such as Nuclear Factor Erythroid 2-Related Factor 2 (NRF2). R
This is hormesis applied to oxygen metabolism, and it depends entirely on the individual's ability to handle the oxidative load.
HBOT stimulates Hypoxia-Inducible Factor (HIF) stabilization via the cycling between hyperoxic and post-treatment normoxic states. R
Repeated intermittent hyperoxia followed by normoxia creates a microenvironment that paradoxically stabilizes HIF-1alpha, driving the expression of Vascular Endothelial Growth Factor (VEGF), Erythropoietin (EPO), and Stromal Cell-Derived Factor 1 (SDF-1). R
This is the same adaptive cascade that Jacob discusses in the context of HIF as an appropriate response to hypoxia, not a pathology to suppress.
HBOT also mobilizes bone marrow-derived stem and progenitor cells through a nitric oxide-dependent mechanism. R
This is analogous to the stem cell mobilizing effects of sunlight exposure and exercise, both of which also trigger NO-mediated signaling.
A single HBOT session at 2.0 ATA for two hours doubles circulating CD34+ cells, and a course of twenty sessions produces an eight-fold increase. R
These stem cells home to sites of injury and contribute to angiogenesis, neurogenesis, and tissue repair.
Benefits
1. Angiogenesis And Neovascularization
HBOT upregulates VEGF at both the mRNA and protein level via AP-1 transcription factor binding to the VEGF promoter through the SAPK/JNK and ERK pathways. R
This drives the formation of new capillaries from existing vasculature, improving blood supply to ischemic tissues.
In diabetic foot ulcers, HBOT reduces the risk of major amputation (OR 0.242) and improves the chance of complete wound healing (OR 9.992). R
2. Stem Cell Mobilization
HBOT increases circulating stem cell factor by 50% in animal models and doubles colony-forming cells in human subjects. R
A high proportion of the mobilized progeny cells express receptors for VEGF-2 and SDF-1, directing them toward damaged tissue. R
3. Mitochondrial Biogenesis And Function
HBOT at 2.0 ATA over 40 sessions significantly increases maximal oxidative phosphorylation capacity (effect size 1.085), maximal uncoupled capacity (effect size 0.956), and mitochondrial mass (MTG marker) in muscle biopsies. R
This translates to measurable improvements in VO2max (effect size 0.989) and oxygen consumption at the anaerobic threshold. R
HBOT also decreases mitochondrial-mediated apoptosis signaling and reduces mitochondrial membrane potential in dysfunctional cells. R
4. Neuroinflammation Reduction
HBOT modulates microglial activation and reduces pro-inflammatory cytokines including IL-1beta, IL-6, and TNF-alpha while increasing the anti-inflammatory cytokine IL-10. R
The anti-inflammatory effect is mediated in part by hyperoxia interfering with NF-kappaB (NF-kB) and its inhibitor I-kappaB-alpha (IkBa). R
In spinal cord injury models, HBOT reduces astrocyte and microglial markers more effectively than normobaric oxygen alone. R
5. Neuroplasticity And Cognitive Function
HBOT induces neuroplasticity through increased cerebral blood flow, improved brain microstructure integrity, and activation of regions involved in cognitive and emotional processing. R
In long COVID, 40 sessions of HBOT produced significant improvements in global cognitive scores, sleep, psychological symptoms, and pain interference that persisted at one-year follow-up. R
6. Wound Healing
HBOT enhances collagen matrix formation, which is essential for angiogenesis and is inhibited by hypoxia. R
For compromised skin grafts and flaps, HBOT improves graft and flap survival compared to standard surgical care alone. R
In the chronic wound population, HBOT is the single most evidence-supported wound indication with consistent reductions in amputation rates and improved healing outcomes. R
Conditions HBOT May Help
Long COVID / Post-COVID Condition
A sham-controlled randomized trial of 40 daily HBOT sessions showed significant improvements in global cognitive function, energy, sleep, psychological symptoms (somatization, depression, anxiety), and pain interference. R
Long-term follow-up confirmed that improvements persisted at one year post-treatment. R
A 2026 systematic review of 21 studies found HBOT improved quality of life, fatigue, cognition, neuropsychiatric symptoms, and cardiopulmonary function in long COVID patients. R
HBOT addresses several mechanistic drivers of long COVID that align with the JD framework: endothelial dysfunction (glycocalyx loss and TCLS), mitochondrial dysfunction, chronic inflammation, and tissue hypoxia. R
I discuss the full long COVID treatment framework in my long COVID natural treatment protocol, where HBOT can be integrated as an adjunctive modality.
Traumatic Brain Injury (TBI) And Post-Concussion Syndrome
A 2026 systematic review of HBOT for TBI demonstrated clinical efficacy in improving memory, executive function, and neuroprotection, particularly for post-concussive symptoms. R
Mechanistic studies highlight HBOT's role in modulating TLR4/NF-kB and VEGF/ERK pathways, facilitating neuroprotection, angiogenesis, and synaptogenesis. R
I cover alternative TBI approaches in my post on ceftriaxone and beta-lactams for TBI, which targets glutamate regulation through a different mechanism than HBOT.
A randomized trial in severe TBI found that HBOT increased Glasgow Coma Scale scores and decreased NIH Stroke Scale scores compared to controls. R
A retrospective cohort study in adults with childhood TBI showed significant cognitive improvements after HBOT even decades after the original injury. R
Stroke Recovery
HBOT combined with exercise and mental imagery rehabilitation in chronic stroke patients (3-48 months post-stroke) was safe and feasible, with trends for improved upper limb motor function. R
Brain imaging studies show HBOT can increase metabolic activity in brain regions that appear dormant but not destroyed. R
The evidence for acute ischemic stroke is mixed, with meta-analyses showing no clear benefit for HBOT in the hyperacute phase. R
Diabetic Foot Ulcers And Chronic Wounds
A meta-analysis of 11 studies showed HBOT significantly reduced major amputations in diabetic foot ulcer patients (10.7% vs 26.0%, NNT 7). R
Fibromyalgia Secondary To TBI
A randomized controlled trial found HBOT (60 sessions at 2.0 ATA) significantly reduced pain intensity (effect size d=-0.95) compared to pharmacological treatment (pregabalin or duloxetine) in fibromyalgia patients with TBI history. R
SPECT imaging showed increased brain activity in frontal and parietal regions correlating with clinical improvement. R
Hard Vs Soft Chambers
There are two physical classes of hyperbaric chambers, and the distinction matters greatly for the chronic illness population.
Hard chambers (monoplace or multiplace) are steel or acrylic vessels that are pressurized to 2.0-3.0 ATA and deliver 100% medical-grade oxygen.
These are FDA-cleared for 14 medical indications and are the standard in hospital-based hyperbaric medicine units.
The higher pressure and pure oxygen delivery produce blood oxygen tensions above 1,800 mmHg at 2.0 ATA. R
Hard chambers carry a higher risk of oxygen toxicity, barotrauma, and require medical supervision throughout each session. R
Soft chambers (mild HBOT or portable chambers) are fabric or PVC enclosures that pressurize to 1.3-1.5 ATA using an oxygen concentrator that delivers approximately 24-40% oxygen.
Blood oxygen tension in a soft chamber typically reaches 200-250 mmHg, roughly 15% of what a hard chamber achieves. R
Soft chambers are not FDA-cleared for any medical condition and are classified as wellness devices rather than medical devices.
Jacob's position: For the chronic illness population with compromised redox capacity, soft chambers at 1.2-1.5 ATA provide a gentler on-ramp that still triggers the hormetic response (HIF stabilization, stem cell mobilization, angiogenesis) without the oxidative risk of higher pressures.
The lower pressure reduces the risk of oxygen toxicity and barotrauma, allowing longer or more frequent sessions.
Soft chambers are also more affordable and accessible for home use, which matters for conditions requiring 20-40+ sessions.
The trade-off is that the therapeutic signal is weaker, so a higher total number of sessions may be needed compared to hard chamber protocols.
For severe acute conditions (carbon monoxide poisoning, necrotizing infections, acute TBI), a hard chamber is non-negotiable and soft chambers are insufficient.
HBOT should be distinguished from normobaric oxygen therapy (oxygen at 1 ATA through a mask or nasal cannula), which does not involve pressure and does not achieve the same tissue oxygen tensions or biological effects.

Protocols And Safety
Typical HBOT protocols range from 1.3 to 2.5 ATA with session durations of 60 to 90 minutes.
Standard protocols for chronic conditions:
| Condition | Pressure | Sessions | Frequency |
|---|---|---|---|
| Long COVID | 2.0 ATA | 40 | Daily |
| TBI/Concussion | 1.5-2.0 ATA | 20-40 | Daily |
| Chronic wound | 2.0-2.4 ATA | 20-40 | Daily |
| Soft chamber wellness | 1.3-1.5 ATA | 20-40 | Daily or 5x/week |
Jacob's recommended protocol for the chronic illness population:
Start with a soft chamber at 1.3 ATA for 60 minutes, 5 days per week, for a minimum of 20 sessions before evaluating response.
If tolerated well, consider increasing to 1.5 ATA.
If a hard chamber is used, start at 1.5 ATA rather than 2.0 ATA and monitor closely for oxidative stress symptoms (fatigue flare, headache, joint pain).
Always ensure adequate antioxidant support during a course of HBOT, especially if using higher pressures.
Common side effects include ear barotrauma (difficulty equalizing pressure), sinus pain, and temporary myopia (reversible). R
Serious adverse events are rare but include oxygen toxicity seizures (0.06% incidence, primarily above 2.0 ATA), pneumothorax, and fire risk from improper equipment use. R
The risk of oxygen toxicity seizures increases significantly above 2.0 ATA.
Fire risk is the most serious safety concern at a facility level, which is why FDA-cleared chambers require strict protocols around static-generating clothing and electrical devices. R
Contraindications
Untreated pneumothorax is the only absolute contraindication to HBOT, because pressure changes can convert it into a life-threatening tension pneumothorax. R
Relative contraindications include:
- Upper respiratory infections and sinus congestion (can prevent pressure equalization)
- Severe COPD with blebs (risk of pneumothorax)
- Congestive heart failure (volume and oxidative load concerns)
- Uncontrolled seizures (hyperoxia can lower seizure threshold)
- Recent thoracic or eye surgery (air trapping risk)
- Current chemotherapy with doxorubicin, bleomycin, or cisplatin (increased toxicity risk)
- Pregnancy (insufficient safety data)
- Claustrophobia (can be mitigated with open-circuit hoods or anxiolysis)
Jacob adds a clinical caution: anyone with known poor redox capacity (SOD2 mutations, glutathione depletion, chronic oxidative stress) may experience a paradoxical worsening of symptoms from HBOT because the therapy generates a controlled oxidative challenge.
Test first, then treat.
Testing
Before beginning HBOT, pre-existing oxidative stress status and antioxidant capacity should be assessed to ensure the therapy will be hormetic rather than harmful.
Blood And Urine Markers
Oxidative stress markers: evaluate red blood cell glutathione status, superoxide dismutase activity, and lipid peroxidation markers to determine baseline redox capacity.
Glutathione: reduced glutathione (GSH) and the ratio of GSH to oxidized glutathione (GSSG) indicate the body's ability to handle the oxidative load from HBOT.
Superoxide Dismutase Activity: measures the efficiency of the SOD enzyme system, particularly relevant for individuals carrying SOD2 variants.
Iron panel (ferritin, TIBC, serum iron): excess iron amplifies oxidative stress under hyperoxia and should be ruled out before starting HBOT. R
TNF-alpha, hsCRP, IL-6: baseline inflammatory markers to track response to HBOT, since the therapy has anti-inflammatory effects that should correlate with clinical improvement. R
Functional Lab Panels
I use the Cellular Zoomer to assess mitochondrial function, oxidative stress, and methylation status before and after an HBOT protocol.
I use the Cardio Zoomer to evaluate endothelial function, since HBOT improves vascular health and angiogenesis and these changes should be measurable.
I use the Immune Zoomer to track inflammatory cytokine changes across a course of HBOT.
I use the Long COVID Bundle (Cardio + Toxin + Gut + Cellular + Viral) for post-viral patients considering HBOT, since it captures the multisystem dysfunction that HBOT aims to address.
For follow-up, repeat the Cellular Zoomer after 20 sessions to assess whether mitochondrial function has measurably improved.
Genetics
I use the Methylation Genetics panel and Toxin Genetics panel to identify SOD2, NOS3, and glutathione synthesis variants that influence HBOT safety and dosing.
Transcutaneous Oximetry
TcPO2: transcutaneous oxygen pressure measurement is the gold standard for determining whether a wound or tissue bed will respond to HBOT. R
Values below 40 mmHg on room air that increase to above 100 mmHg during HBOT predict a favorable response.
Mechanisms Of Action
Simple:
- HBOT forces oxygen into the plasma at concentrations high enough to reach hypoxic tissues that hemoglobin cannot access, triggering the body's natural repair and regeneration pathways.
- The intermittent hyperoxia creates a controlled hormetic stress that upregulates antioxidant defenses, stem cell activity, and new blood vessel growth.
- The post-treatment return to normoxia stabilizes HIF, which activates VEGF and other growth factors that drive angiogenesis and neuroplasticity.
- Breathing oxygen under pressure also reduces inflammation by suppressing NF-kB signaling and shifting the cytokine profile toward anti-inflammatory mediators.

Advanced:
- Henry's Law / Plasma Oxygen Dissolution: at 2.0 ATA breathing 100% oxygen, the partial pressure of oxygen in arterial blood rises from approximately 100 mmHg to nearly 2,000 mmHg, with dissolved oxygen increasing from 0.3 mL/dL to approximately 4.4 mL/dL. R This sustains tissue oxygenation even when hemoglobin is fully saturated or microvascular flow is compromised by TCLS and glycocalyx degradation.
- HIF-1alpha Stabilization (Hyperoxic-Hypoxic Paradox): during HBOT, increased ROS production from mitochondrial complex III and NADPH oxidase paradoxically promotes HIF-1alpha stabilization upon return to normoxia. The prolonged half-life of antioxidant scavengers (glutathione peroxidase, SOD) relative to ROS creates a low ROS/scavenger ratio post-treatment, mimicking a hypoxic state that stabilizes HIF-1alpha. R This induces VEGF, EPO, SDF-1, and stem cell factor expression.
- VEGF Upregulation / Angiogenesis: HBOT induces VEGF transcription via AP-1 binding to the VEGF promoter through the SAPK/JNK and ERK signaling pathways. R VEGF drives endothelial cell migration, tubule formation, and capillary budding from post-capillary venules. The oxygen diffusion distance from capillaries increases by up to 286%. R
- Stem Cell Mobilization (NO-Dependent): HBOT increases bone marrow nitric oxide concentration by approximately 1,000 nM, which signals the release of CD34+ hematopoietic and mesenchymal stem cells into peripheral circulation. R These cells express VEGFR-2 and CXCR4, directing them to SDF-1-rich hypoxic tissue for angiogenesis and repair.
- Mitochondrial Biogenesis: HBOT increases mitochondrial mass (MTG marker) and oxidative phosphorylation capacity through pathways involving PGC-1alpha, NRF1, and TFAM activation. R This improves cellular energy production in tissues that had been ATP-deficient due to hypoxia, which is particularly relevant in the context of JD-driven mitochondrial dysfunction.
- NF-kB Inhibition / Anti-Inflammatory: hyperoxia interferes with NF-kB nuclear translocation by stabilizing its inhibitor IkBa. R This reduces the transcription of pro-inflammatory cytokines (IL-1beta, IL-6, TNF-alpha) while increasing anti-inflammatory IL-10. HBOT also suppresses microglial EAAT2 expression, reducing excitotoxic glutamate release and secondary neuroinflammation. R
- ROS-Mediated Hormesis / NRF2 Activation: the controlled oxidative burst from HBOT activates NRF2, which drives the expression of AREs including glutathione peroxidase, catalase, HO-1, and SOD. R This strengthens the cell's overall antioxidant capacity, but only if the NRF2-ARE axis is functional (requires DJ-1 and adequate reducing equivalents).
- Collagen Synthesis And Wound Healing: HBOT provides the oxygen substrate required for prolyl hydroxylase, the rate-limiting enzyme in collagen cross-linking and deposition. R Without adequate tissue oxygen tension, the collagen matrix cannot mature and angiogenesis cannot proceed.
Genetics
SOD2
The Superoxide Dismutase 2 (SOD2) gene encodes the mitochondrial manganese-dependent superoxide dismutase, the primary enzyme that quenches superoxide anions produced during oxidative phosphorylation.
The rs4880 (Ala16Val) variant is a functional polymorphism that reduces SOD2 import into the mitochondrial matrix, decreasing the efficiency of superoxide clearance by 30-40%.
Jacob carries this variant himself and flags it as clinically relevant for HBOT, because individuals with reduced SOD2 activity are less able to handle the controlled ROS burst that HBOT produces.
Val/Val (rs4880) homozygotes may need to start soft chamber protocols at 1.3 ATA rather than 1.5 ATA and should ensure adequate manganese and antioxidant support before and during an HBOT course. R
NOS3
The Nitric Oxide Synthase 3 (NOS3) gene encodes endothelial nitric oxide synthase (eNOS), which produces the nitric oxide required for HBOT-mediated stem cell mobilization and vasodilation.
The rs1799983 (Glu298Asp) variant reduces eNOS activity and NO production, potentially blunting the stem cell mobilization response to HBOT. R
Individuals with NOS3 variants may require more HBOT sessions to achieve the same stem cell response, or may benefit from concurrent L-citrulline supplementation (not L-arginine, per Jacob's caution on NO boosters in the JD population).
GPX1
The Glutathione Peroxidase 1 (GPX1) gene encodes the primary selenium-dependent enzyme that reduces hydrogen peroxide to water.
The rs1050450 (Pro198Leu) variant reduces GPX1 activity, impairing the clearance of hydrogen peroxide generated by SOD and by the HBOT-induced ROS burst.
Reduced GPX1 function increases the risk of oxidative stress accumulation during a course of HBOT.
NRF2 / NFE2L2
The Nuclear Factor Erythroid 2-Related Factor 2 (NRF2, encoded by NFE2L2) is the master transcription factor regulating antioxidant response element (ARE) gene expression.
The rs6721961 and rs1806649 variants in the NRF2 promoter region reduce NRF2 expression and ARE activation, potentially limiting the hormetic benefit of HBOT. R
NRF2 function is dependent on DJ-1 stability, which requires sufficient SCFAs from resistant starch and butyrate, as discussed in the integrated stress response post.
The NRF2 pathway is also central to why some individuals with CIRS and multiple chemical sensitivities react poorly to hormetic therapies, which I cover in my NRF2 and CIRS sensitivities post.
The connection between mitochondrial signaling, exercise, and longevity peptides like humanin intersects with HBOT through the shared upregulation of mitochondrial biogenesis and stress resistance pathways.
HBOT's effects on glymphatic clearance and cerebral perfusion overlap with strategies for improving glymphatic function and AQP4 biohacks, since both approaches aim to improve waste clearance from the brain.
More Research
- HBOT is being investigated for aging intervention, with animal studies showing reduced cellular senescence markers and improved telomere length after repeated sessions. R The human data are preliminary and the optimal anti-aging protocol has not been defined.
- The optimal number of HBOT sessions for chronic conditions is unknown. The 40-session protocols used in the long COVID and TBI trials are resource-intensive and may not be accessible. Shorter protocols (10-20 sessions) have shown inconsistent results. R
- HBOT can trigger paradoxical oxidative stress in individuals with poor redox capacity, and there is no validated biomarker panel to predict who will respond well versus worsen. Monitoring symptoms (fatigue, brain fog, pain flare) during the first 5-10 sessions is the most practical clinical tool.
- The combination of HBOT with other neuroplasticity-inducing modalities (exercise, cognitive training, limbic retraining) is underexplored but mechanistically compelling. HBOT may prime the brain for plasticity that other modalities then consolidate.
- For biomarker testing before an HBOT protocol, I use the Cellular Zoomer to assess mitochondrial function and oxidative stress status, the Cardio Zoomer for endothelial baseline, and the Methylation Genetics panel to identify relevant SOD2 and NRF2 variants.
- There is a theoretical concern that the pro-angiogenic (VEGF-mediated) effects of HBOT could theoretically accelerate tumor angiogenesis in individuals with existing malignancies. Clinical trial data on HBOT and cancer recurrence are mixed and insufficient to draw firm conclusions.
- HBOT is sometimes conflated with normobaric oxygen therapy. The pressure component is not optional for the effects described here, and the two modalities are not interchangeable.
- Jacob's clinical observation: the sickest patients (severe ME/CFS, advanced CIRS, multiple chemical sensitivity) often cannot tolerate 2.0 ATA hard chamber protocols and respond better to 1.3 ATA soft chamber sessions of shorter duration (45 minutes). Test tolerance with a single session before committing to a full protocol.
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Lion's Mane
1000mg/day
Omega-3 (DHA)
2g/day
Phosphatidylserine
100mg 3x/day