L-Citrulline vs L-Arginine For Nitric Oxide: A Safety-First Comparison
By Jacob Gordon, INHC, FMT-CL-citrulline and L-arginine are both promoted as nitric oxide boosters, but they travel fundamentally different metabolic paths with very different safety profiles for the chronically ill.
In this post, we will compare L-citrulline and L-arginine for nitric oxide production, explain why arginine is riskier in the Junction Dysfunction (JD) population, and cover the eNOS uncoupling and BH4 cycle that determines whether NO helps or harms you.

What Is Nitric Oxide
Nitric Oxide (NO) is a gaseous signaling molecule produced by the endothelial lining of your blood vessels.
It is one of the most potent vasodilators in the human body and was named Molecule of the Year in 1992, with its discovery earning the 1998 Nobel Prize in Physiology or Medicine. R
NO signals vascular smooth muscle to relax, which widens blood vessels, lowers blood pressure, improves nutrient delivery, and supports erectile function.
Beyond circulation, NO regulates mitochondrial respiration, immune function, neurotransmission, and platelet aggregation. R
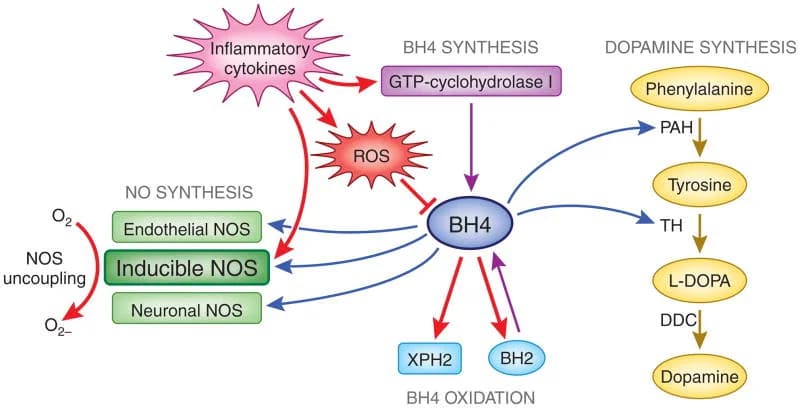
The body produces NO through three Nitric Oxide Synthase (NOS) isoforms: endothelial NOS (eNOS), neuronal NOS (nNOS), and inducible NOS (iNOS). R
All three isoforms convert L-arginine into NO plus L-citrulline, with tetrahydrobiopterin (BH4) as the essential cofactor. R
The NO/Peroxynitrite Fork In The Road
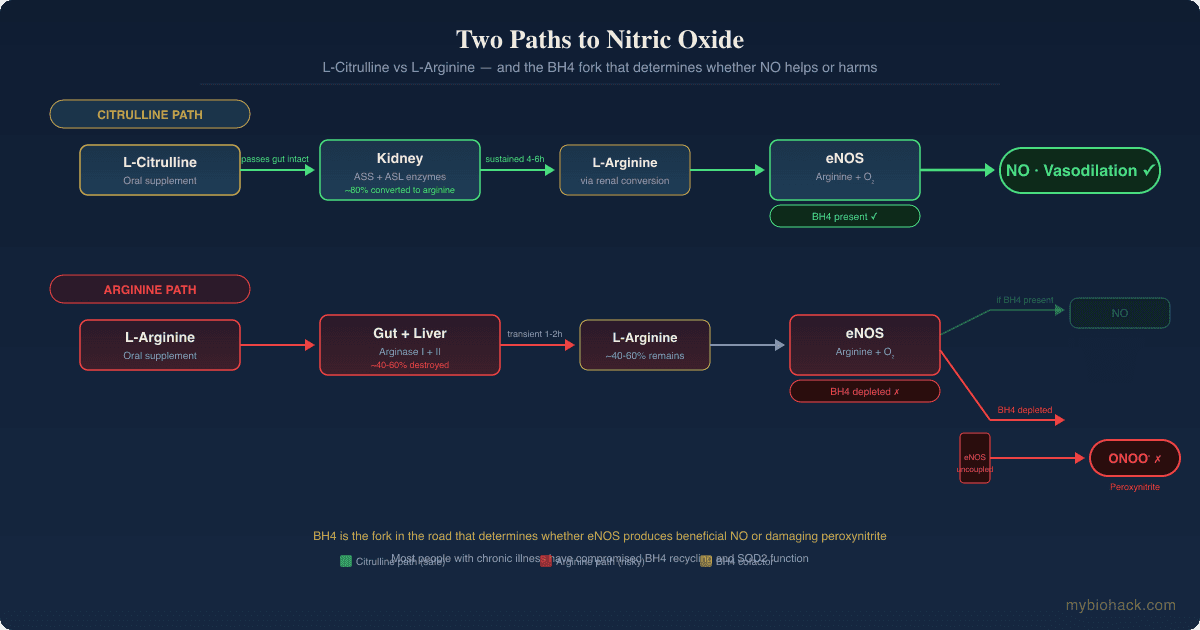
Under ideal conditions, eNOS produces NO that diffuses to smooth muscle and signals vasodilation.
When BH4 is depleted or the enzyme is otherwise stressed, eNOS becomes uncoupled and produces superoxide instead of NO. R
Superoxide reacts with any available NO at near-diffusion-limited speed to form peroxynitrite (ONOO-), a highly destructive oxidant. R
Peroxynitrite oxidizes BH4 into BH2, which further uncouples eNOS, creating a self-sustaining damage loop. R

This is the eNOS uncoupling / BH4 / ONOO cycle that Jacob argues is central to understanding why NO supplementation can either help or harm depending on your redox status.
Martin Hall described a similar NO/ONOO cycle, but Jacob argues Hall did not fully grasp the upstream glycocalyx damage and MSS driving the pathology.
Most people who supplement for NO do not have functioning BH4 recycling and SOD2 activity, which means they may be generating peroxynitrite, not the beneficial NO they expect.
Citrulline Versus Arginine: Biochemical Comparison
L-Arginine
L-arginine is a conditionally essential amino acid and the direct substrate for all three NOS isoforms.
When you swallow L-arginine, approximately 40% is degraded by arginase in the intestinal wall before it ever reaches the portal circulation. R
Of what survives the gut, another 15% is extracted and metabolized by the liver on first pass. R
This extensive presystemic elimination means oral L-arginine produces a modest, short-lived spike in plasma arginine that returns to baseline within 1-2 hours. R
High doses of L-arginine (above 6-9 grams) frequently cause diarrhea, cramping, and nausea due to NO-mediated water and electrolyte secretion in the gut. R
L-Citrulline
L-citrulline is a non-essential amino acid first isolated from watermelon (Citrullus lanatus) and is the natural byproduct of the NOS reaction.
Unlike arginine, citrulline is not a substrate for intestinal or hepatic arginase, so it passes through the gut and liver largely intact. R
Citrulline travels to the kidneys, where proximal tubular cells convert it to arginine via argininosuccinate synthase and argininosuccinate lyase. R
This renal conversion produces a sustained elevation in plasma arginine lasting 4-6 hours, far exceeding what an equivalent dose of arginine achieves. R
The landmark Schwedhelm 2008 study demonstrated that 3 grams of L-citrulline raised plasma arginine area-under-the-curve more effectively than 3 grams of L-arginine. R
Citrulline also inhibits arginase activity, which further spares arginine from degradation. R
Gastrointestinal tolerance is excellent up to 15 grams per day in healthy volunteers. R
Head To Head Summary
| Factor | L-Citrulline | L-Arginine |
|---|---|---|
| Oral bioavailability | ~80% converted to plasma arginine | ~40-60% lost to presystemic metabolism |
| Peak plasma arginine elevation | High, sustained 4-6 hours | Modest, transient 1-2 hours |
| Arginase inhibition | Yes (allosteric inhibitor) | No |
| GI tolerance | Excellent up to 15 g/day | Poor above 6-9 g/day |
| Virus reactivation risk | No known effect | Yes (herpesvirus family) |
| Renal conversion required | Yes | No (direct substrate) |
| Effective dose | 3-6 g/day | 6-12 g/day (with diminishing returns) |
Benefits Of L-Citrulline
1. Superior Plasma Arginine Elevation
Oral L-citrulline 3 grams twice daily increases the arginine/ADMA ratio from 186 to 278 and raises urinary nitrate, a biomarker of systemic NO production. R
No equivalent dose of oral arginine produces a comparable effect. R
2. Blood Pressure Reduction
A systematic review and meta-analysis found L-citrulline supplementation reduces systolic blood pressure, with diastolic BP reductions at doses of 6 g/day or higher. R
In hypertensive postmenopausal women, L-citrulline improved endothelial function and reduced aortic blood pressure. R
3. Improved Endothelial Function
L-citrulline supplementation improves flow-mediated dilation (FMD), a direct measure of endothelial health. R
Chronic daily supplementation for 4 weeks or more produces progressive FMD improvements independent of acute dosing. R
4. Exercise Performance And Recovery
Citrulline malate at 6-8 grams pre-workout reliably increases repetition volume, reduces muscle soreness by approximately 40%, and decreases perceived exertion during high-intensity exercise. R
The mechanism involves both NO-mediated blood flow and ammonia buffering via the urea cycle.
5. No Virus Reactivation
L-citrulline does not serve as a substrate for viral replication.
This is the critical safety advantage over arginine for anyone carrying latent herpesviruses, which includes an estimated 67% of the global population under age 50 for HSV-1 alone. R
6. Gentle On The Gut
Human studies demonstrate tolerance up to 15 grams per day without significant gastrointestinal distress. R
This makes citrulline accessible to people with compromised gut function, which includes most of the JD population.
Benefits Of L-Arginine
1. Direct NOS Substrate
L-arginine is the only direct substrate for NO production.
Intravenous arginine bypasses oral bioavailability limitations and is used clinically for pulmonary hypertension, urea cycle disorders, and growth hormone stimulation testing. R
2. Blood Pressure Reduction In Hypertension
Meta-analyses show L-arginine reduces systolic BP by 2.2-5.4 mmHg and diastolic BP by 2.7-3.1 mmHg in adults with hypertension. R
Effects are more consistent in people with established hypertension than in normotensive individuals.
3. Wound Healing And Immune Support
Arginine is required for collagen synthesis, T-cell function, and macrophage activity. R
Surgical patients receiving arginine-supplemented nutrition show reduced hospital stays and fewer infections. R
4. Erectile Function
Arginine is a precursor to NO in the corpus cavernosum, and supplementation at 3-5 grams daily has shown benefit for mild to moderate erectile dysfunction. R
Citrulline also works for this indication via the same pathway, often with better tolerability.
5. Insulin Sensitivity
Some evidence suggests L-arginine improves insulin sensitivity through NO-mediated increases in skeletal muscle blood flow and glucose disposal. R
Limitations
The bioavailability ceiling limits all benefits.
Acute doses below 6 grams produce no significant increase in NO biomarkers. R
Doses above 6-9 grams cause GI distress in many people. R
Who Should Choose Which
Choose L-citrulline if:
- You have a history of herpesvirus infections (HSV-1, HSV-2, EBV, VZV, CMV) or frequent cold sore outbreaks
- You want sustained NO support without blood level crashes
- You have a sensitive gut or malabsorption issues
- You carry the MTHFR A1298C or SOD2 rs4880 variant
- You take NO for endothelial health, blood pressure, or exercise recovery
- You are part of the JD population (post-viral illness, POTS/VA, CIRS, MCAS, ME/CFS, long COVID)
Choose L-arginine if:
- You are using intravenous arginine in a clinical setting
- You need the growth hormone stimulation effect (diagnostic testing or specific protocols)
- You combine it with an arginase inhibitor like L-citrulline or L-norvaline for synergistic effect
- You have no history of herpesvirus reactivation and tolerate oral arginine without GI issues
The combination works better than either alone. A 2016 study showed that 1 gram L-citrulline plus 1 gram L-arginine raised plasma arginine more effectively than 2 grams of either alone. R

Citrulline inhibits arginase, which spares the arginine you take from degradation, producing both a quick spike and sustained elevation.
Safety And Contraindications
L-Arginine Reactivates Latent Viruses
This is the non-negotiable warning for this post.
Herpesviruses require arginine for capsid protein assembly and DNA packaging.
In arginine-deficient cell culture, HSV cannot produce complete virions. R
When arginine is reintroduced, viral replication resumes immediately. R
A 2024 comprehensive review of L-arginine concluded that carriers of latent herpesviruses should avoid arginine supplements and arginine-rich foods. R
A 2025 case report documented HSV-1 reactivation following an arginine overload in a stressed individual, with resolution after L-lysine administration and arginine restriction. R
Reactivation of Epstein-Barr virus (EBV) has also been linked to arginine availability, and EBV directly stimulates IDO, reinforcing the kynurenine shunt that drives neuroinflammation in long COVID and ME/CFS.
This means arginine supplementation is contraindicated in anyone with latent herpesviruses, which is the majority of the adult population.
L-citrulline does not share this risk because circulating arginine from citrulline conversion is regulated by renal conversion rates, not by direct viral hijacking.
Peroxynitrite Risk In The JD Population
Blind NO boosting of any kind is dangerous when BH4 and SOD2 function are compromised.
Jacob's position is that L-arginine and NO booster supplementation is dangerous in the JD population because without proper BH4 and SOD2 function, NO becomes peroxynitrite. R
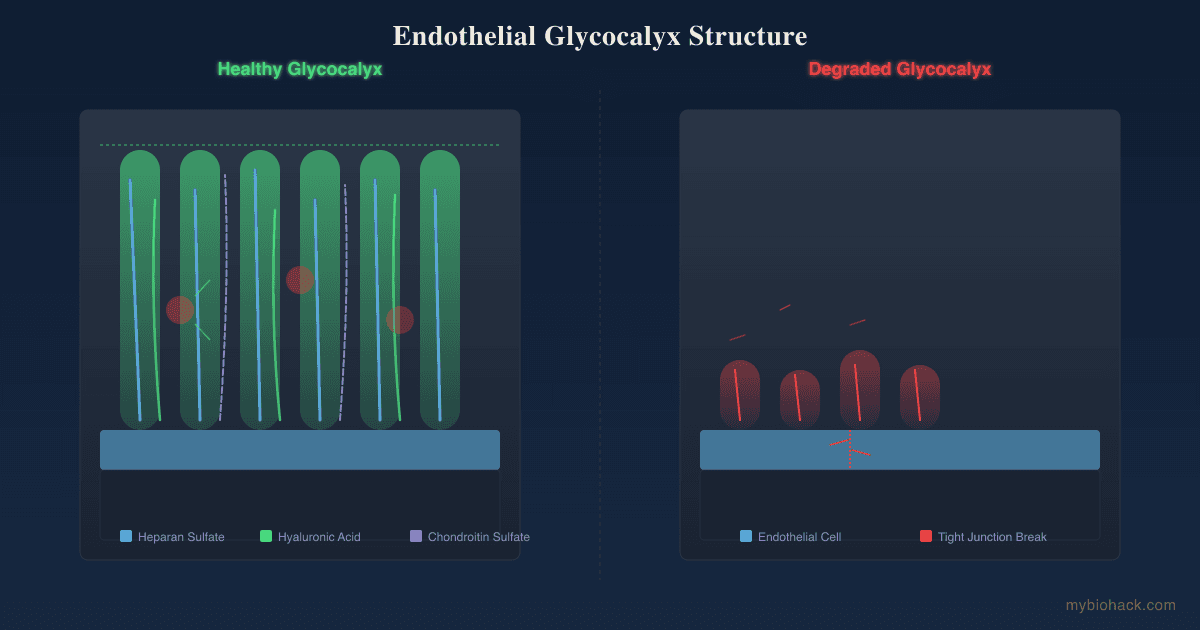
Peroxynitrite damages the glycocalyx, oxidizes BH4, and propagates eNOS uncoupling in a self-sustaining cascade. R
This is detailed in the JD framework as the eNOS uncoupling / BH4 / ONOO cycle: shear stress on the glycocalyx activates eNOS, BH4 quenches NO radicals and becomes BH2, BH2 must be recycled back to BH4 by DHFR, and if BH4 is depleted (genetic A1298C, oxidative overload), the cycle uncouples and produces peroxynitrite instead of NO.
For more on this cascade, see the Junction Dysfunction guide and the BH4 post.
L-citrulline is safer than L-arginine in this population because it does not directly load arginine into viral replication pathways, but it still carries oxidative risk if the BH4/SOD2 system is broken.
General Contraindications
Both supplements should be used with caution in people taking nitrates for angina, PDE5 inhibitors (sildenafil, tadalafil), or antihypertensive medications, as the additive vasodilation can cause hypotension.
L-arginine can worsen herpes outbreaks even at dietary intake levels from nuts, chocolate, and certain meats.
Neither should be used in pregnancy or breastfeeding without medical supervision.
Testing
Before supplementing with any NO precursor, especially if you have chronic illness or post-viral syndrome, testing your redox capacity, BH4 recycling, and SOD2 function is essential.
Blood And Urine Markers
ADMA (asymmetric dimethylarginine) is an endogenous inhibitor of eNOS that competes with arginine for the NOS active site.
Elevated ADMA predicts endothelial dysfunction independently of other risk factors. R
Measurable via Quest Diagnostics through the Cardio IQ Advanced Lipid Panel with Inflammation or the Cardio Zoomer.
Homocysteine is elevated homocysteine associated with oxidative stress, reduced BH4 bioavailability, and increased cardiovascular risk. R
I use the Homocysteine + B12 + Folate test to assess this.
See the homocysteine post for the full analysis.
Oxidative stress markers including 8-OHdG, F2-isoprostanes, and lipid peroxides reflect the balance between NO production and peroxynitrite damage.
Measurable via the Cellular Zoomer (Vibrant Wellness).
Functional Lab Panels
I use the Cardio Zoomer (Vibrant Wellness) to assess endothelial function markers, lipid/lipoprotein profile, ApoB, fasting insulin, and metabolic markers relevant to NO biology.
It includes the lipid panel, insulin resistance markers, and ceramides that predict cardiovascular risk.
I use the Cellular Zoomer (Vibrant Wellness) to assess oxidative stress, organic acids, and methylation markers that reflect BH4 status and redox balance.
I use the Methylation Genetics panel (Vibrant Wellness) to evaluate MTHFR, MTR, MTRR, COMT, BHMT, and other methylation cycle variants that impact BH4 recycling.
See the methylation guide for the full pathway context.
Genetics
I use the Methylation Genetics panel or raw data from a direct-to-consumer genetics test to check the priority SNPs listed in the Genetics section below.
Mechanisms Of Action
Simple:
- L-arginine is the direct raw material that eNOS uses to make NO, but most oral arginine gets destroyed by your gut and liver before reaching your blood.
- L-citrulline takes a back road through your kidneys, where it gradually converts into arginine and provides a steady supply.
- If BH4 (a vitamin-like cofactor) is low, eNOS malfunctions and turns NO production into a free radical factory.
- If SOD2 (an antioxidant enzyme in your mitochondria) is weak, the free radicals from uncoupled eNOS cannot be neutralized and create cascading damage.
Advanced:
- First-Pass Hepatic Metabolism And Arginase Oral L-arginine undergoes extensive presystemic elimination by arginase I and II, which hydrolyze arginine to urea and ornithine. Approximately 40% is degraded in the small intestine by arginase II, and the liver extracts another 15% of what survives. R L-citrulline is not a substrate for arginase and passes through the enterocyte and hepatocyte intact, bypassing this entire bottleneck. R
- Renal Arginine Conversion Citrulline is taken up by proximal tubular cells of the kidney via the B-0,+ amino acid transporter. Once inside, argininosuccinate synthase (ASS) condenses citrulline with aspartate to form argininosuccinate, which argininosuccinate lyase (ASL) cleaves to produce arginine plus fumarate. R This partial urea cycle is highly efficient, converting approximately 80-85% of absorbed citrulline into plasma arginine.
- Arginase Inhibition By Citrulline L-citrulline acts as an allosteric inhibitor of arginase, reducing the degradation of both endogenous and exogenous arginine. R This is why combining citrulline with arginine produces supra-additive increases in plasma arginine. R
- eNOS Uncoupling And The BH4/ONOO Cycle BH4 is the essential cofactor for eNOS that stabilizes the dimeric structure and maintains the coupling of NADPH oxidation to L-arginine oxidation. R When BH4 becomes oxidized to BH2 by peroxynitrite or other ROS, eNOS monomerizes and produces superoxide (O2-) instead of NO. R DHFR (dihydrofolate reductase) recycles BH2 back to BH4, but this pathway becomes overwhelmed under chronic oxidative stress. R The MTHFR A1298C variant impairs DHFR function indirectly through disrupted folate metabolism, reducing BH4 recycling capacity. Superoxide reacts with NO at a rate constant of 6.7 x 10^9 M-1 s-1 to form peroxynitrite, which oxidizes BH4 6-10 times faster than other cellular antioxidants. R This creates a self-reinforcing damage cycle: uncoupled eNOS produces superoxide, superoxide reacts with NO to form ONOO-, ONOO- oxidizes more BH4, and more eNOS uncouples.
- SOD2 Scavenging Manganese superoxide dismutase (MnSOD), encoded by SOD2, is the primary mitochondrial antioxidant enzyme that converts superoxide into hydrogen peroxide. SOD2 sits on the glycocalyx surface and is the first line of defense against superoxide from uncoupled eNOS. R When SOD2 function is impaired (see Genetics below), superoxide accumulates and feeds the ONOO cycle. For the glycocalyx role in this cascade, see the glycocalyx JD chapter and improving the glycocalyx.
Genetics
SOD2 Highest Population Risk
The SOD2 gene encodes mitochondrial manganese superoxide dismutase (MnSOD), the enzyme that converts superoxide to hydrogen peroxide in the mitochondrial matrix.
SOD2 sits on the surface of the glycocalyx and is the only enzyme capable of scavenging superoxide produced by uncoupled eNOS.
rs4880 (Ala16Val) a C-to-T substitution changes alanine to valine at position 16 in the mitochondrial targeting sequence.
The valine variant forms a beta-sheet secondary structure instead of the alpha-helix needed for efficient mitochondrial import. R
This results in 30-40% less active MnSOD reaching the mitochondrial matrix, leading to higher superoxide levels and greater vulnerability to peroxynitrite formation. R
Jacob's clinical observation: most clients with redox imbalances have SOD2 mutations at rs4880 (Jacob has it himself).
This is one of the highest-priority SNPs in the JD framework.
MTHFR
The MTHFR gene encodes methylenetetrahydrofolate reductase, the enzyme that converts 5,10-methylenetetrahydrofolate to 5-methyltetrahydrofolate, the active form of folate used in homocysteine remethylation.
MTHFR also indirectly impacts BH4 recycling because DHFR, the enzyme that reduces BH2 back to BH4, is the same enzyme that initializes the folate cycle by converting folic acid to tetrahydrofolate.
rs1801131 (A1298C) an A-to-C substitution reduces MTHFR enzyme activity to approximately 60-70% of normal in homozygotes.
Unlike C677T, which affects the folate-binding domain, A1298C affects a regulatory domain that modulates DHFR activity.
This variant reduces BH4 recycling capacity, making eNOS uncoupling more likely under oxidative stress. R
See the BH4 post for full details.
GCH1
The GCH1 gene encodes GTP cyclohydrolase I, the rate-limiting enzyme in the de novo synthesis of BH4 from guanosine triphosphate.
Variants in GCH1 reduce BH4 synthesis capacity, which directly impacts eNOS function and NO production.
Reduced GCH1 expression has been linked to hypertension, endothelial dysfunction, and increased cardiovascular risk. R
DHFR
The DHFR gene encodes dihydrofolate reductase, the salvage enzyme that recycles BH2 back to BH4.
DHFR is the same enzyme that converts dietary folic acid into tetrahydrofolate and is inhibited by methotrexate.
Variants that reduce DHFR expression impair BH4 regeneration, decreasing the BH4:BH2 ratio and promoting eNOS uncoupling. R
More Research
- Combination therapy outperforms either alone A randomized crossover study found that 1 gram L-citrulline plus 1 gram L-arginine raised plasma arginine more than 2 grams of either amino acid. R The mechanism is citrulline's arginase-inhibiting effect, which spares the co-administered arginine from degradation. For athletic performance or general NO support, the combination stack is worth considering.
- Arginine/ADMA ratio as a clinical target The arginine/ADMA ratio is a stronger predictor of NO production than arginine levels alone. R L-citrulline 3 grams twice daily consistently improves this ratio. I use the Cardio Zoomer and Advanced Lipid Panel to assess the arginine/ADMA ratio clinically.
- BH4 rescue strategies Supplementing sapropterin (synthetic BH4), folinic acid, or methylfolate can support BH4 recycling and recouple eNOS. See the BH4 post for full protocols. Vitamin C also protects BH4 from oxidation and improves eNOS coupling. R
- L-lysine as arginine antagonist L-lysine competes with arginine for intestinal absorption and renal transport. Supplementation at 1-3 grams daily reduces HSV recurrence frequency by approximately 2.4-fold compared to placebo. R For anyone with active herpesvirus issues who needs NO support, combining L-citrulline with L-lysine may be a viable strategy.
- Dietary nitrate pathway is distinct Beetroot juice and leafy greens provide dietary nitrate that converts to NO via the nitrate-nitrite-NO pathway (oral bacteria reduce nitrate to nitrite, which is then reduced to NO in the acidic stomach and hypoxic tissues). This pathway bypasses eNOS entirely and does not depend on BH4 or arginine, making it safer for the JD population than direct arginine loading. It does not reactivate viruses. See the blood pressure post for more on dietary nitrate.
- Jacob's clinical observation In his practice, Jacob finds that most people who attempt NO supplementation without testing their BH4 recycling and SOD2 status eventually report fatigue, brain fog, or symptom flares. The safest entry point for NO support in the JD population is a low dose of L-citrulline (3 grams, evaluate over 7 days) after confirming SOD2 function and BH4 recycling capacity through genetic and biomarker testing. For the full context on why endothelial health depends on glycocalyx integrity, see the TCLS JD chapter and glycocalyx chapter. For the relationship between NO, VEGF, and angiogenesis, see the VEGF post. For the mitochondrial connection to NO signaling, see the mitochondrial psychobiology post. For the TGF-beta1 and endothelial remodeling connection, see the TGF-beta1 post.
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Electrolyte Complex
1 scoop/day
CoQ10
200mg/day
Magnesium Glycinate
400mg at bedtime