The Glymphatic-Lymphatic Handoff: Meningeal Lymphatics And Brain Drainage
By Jacob Gordon, INHC, FMT-CThis article contains affiliate links. As an Amazon Associate, MyBioHack earns from qualifying purchases at no extra cost to you. We only link products we research and stand behind.
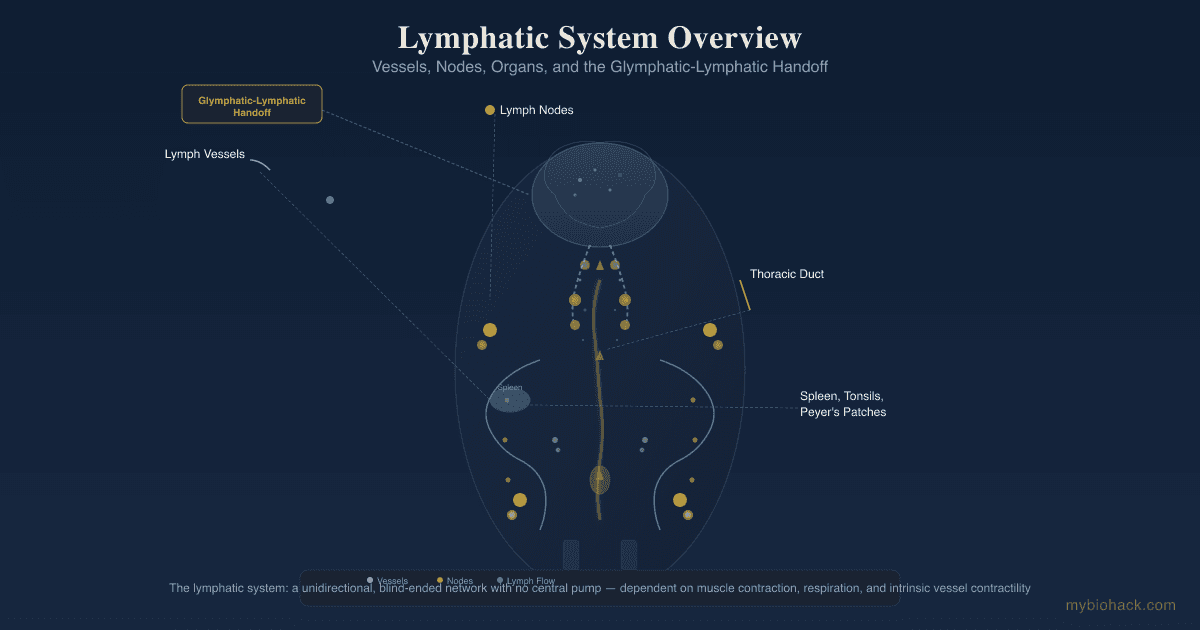
Meningeal lymphatic vessels are the drainage pipes that carry cerebrospinal fluid waste out of the skull, and when they slow down the brain starts to keep its own garbage.
In this post, we will discuss how the glymphatic system hands brain waste off to the meningeal lymphatics, why that handoff fails with age, how it connects to Alzheimer's, long COVID brain fog, and traumatic brain injury, and what you can do to keep brain drainage moving.

Basics Of Meningeal Lymphatic Drainage
For most of medical history the brain was taught as an organ with no lymphatic vessels.
That was wrong.
In 2015 two labs independently found functional lymphatic vessels lining the dural sinuses of the brain, now called Meningeal Lymphatic Vessels (mLVs). R R
These vessels sit in the dura mater, the tough outer layer of the meninges that wrap the brain and spinal cord.
They run alongside the major venous sinuses and the middle meningeal artery, and they express the standard lymphatic endothelial markers (LYVE-1, PROX1, podoplanin, VEGFR-3).
Their job is to collect cerebrospinal fluid (CSF) along with the macromolecules and immune cells suspended in it, and to carry that fluid out of the skull to the deep cervical lymph nodes (dcLN) in the neck. R
From the deep cervical nodes the waste joins the body's general lymphatic circulation and is eventually processed and excreted.
This matters because the brain generates a constant stream of metabolic waste, including the amyloid-beta (Aβ) and tau proteins that aggregate in neurodegeneration.
Waste that is not drained accumulates, and accumulation drives inflammation and protein misfolding.
The meningeal lymphatics are the final common exit route, and they are the part of the system that no one knew existed until recently.
The Glymphatic-Lymphatic Handoff
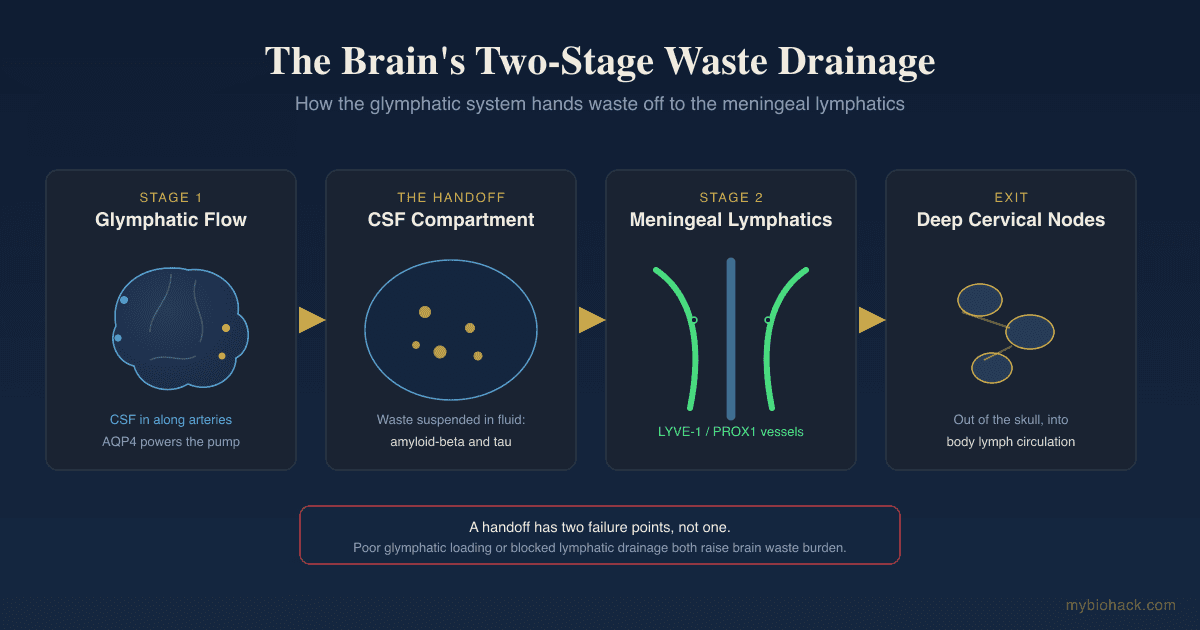
The brain clears waste in two connected stages, and the connection between them is the part most people miss.
The first stage is the glymphatic system, a glia-dependent perivascular network described by the Nedergaard and Iliff groups. R
In the glymphatic stage, CSF flows into the brain along the spaces surrounding penetrating arteries, pushes through the brain tissue, mixes with interstitial fluid (ISF), and flushes dissolved waste back out along the spaces surrounding veins.
That flow depends almost entirely on Aquaporin-4 (AQP4), the water channel packed into the astrocyte endfeet that wrap brain capillaries.
Deleting AQP4 in mice cuts CSF influx and drops interstitial solute clearance, including amyloid-beta clearance, by roughly 70 percent. R
I have covered this first stage in depth in how to improve your glymphatic system and AQP4 and in the post on the glutamate neuroinflammation glymphatic feedback loop.
The second stage is the meningeal lymphatic stage.
The glymphatic system does not actually carry waste out of the head.
It carries waste from deep brain tissue back into the CSF compartments around the brain surface.
The meningeal lymphatics are what take it from there, absorbing that CSF and its solutes and routing it down to the deep cervical lymph nodes. R
This is the handoff.
Glymphatic flow is the upstream pump that loads waste into the CSF, and meningeal lymphatic drainage is the downstream pipe that removes it from the skull.
A handoff has two failure points, not one.
You can have intact AQP4 and good glymphatic flow but blocked meningeal lymphatics, in which case waste circulates in the CSF and is never removed.
You can also have open meningeal lymphatics but poor glymphatic loading, in which case little waste ever reaches the drainage pipe.
Both failure modes raise the brain's waste burden, and the two systems are physically coupled, so dysfunction in one tends to drag down the other.
In the Junction Dysfunction (JD) framework this fits the larger story of fluid handling across the interstitium, the body's third circulatory compartment, and the lymphatic and glymphatic systems chapter covers how AQP4 and Notch signaling tie the two together.
How Aging Breaks Meningeal Lymphatic Drainage
Meningeal lymphatic vessels do not stay healthy on their own.
They regress with age, and the regression is functional, not just structural.
In aged mice the meningeal lymphatic vessels are narrower and cover less area, and the drainage of CSF macromolecules into the deep cervical lymph nodes falls sharply. R
When researchers surgically blocked meningeal lymphatic drainage in young mice, they reproduced the aged pattern, including worse performance on learning and memory tasks. R
The reverse worked too.
Delivering Vascular Endothelial Growth Factor C (VEGF-C), the master growth signal for lymphatic vessels, into the CSF of aged mice expanded the meningeal lymphatic network and improved CSF perfusion and drainage. R
VEGF-C is the lever here because VEGFR-3 on lymphatic endothelium is what drives meningeal lymphangiogenesis, the growth and maintenance of these vessels.

This is one of the reasons I argue against reflexively trying to suppress growth factors, which I cover in the post on VEGF and why you should not reflexively lower it.
Growth factors like VEGF and TGF-beta1 are doing adaptive repair work, and the meningeal lymphatic literature is a clean example of that principle.
The aging decline of brain drainage is not a curiosity.
It tracks with the timeline of when amyloid and tau begin to accumulate, and it is a plausible upstream contributor to why the aging brain clears waste poorly.
Meningeal Lymphatics And Overlapping Conditions
The same drainage failure shows up across conditions that mainstream medicine treats as unrelated.
Alzheimer's Disease
Impaired meningeal lymphatic drainage worsens amyloid-beta deposition in mouse models, and meningeal lymphatic dysfunction is now considered an aggravating factor in age-associated cognitive decline. R
There is also a treatment-relevant twist.
When meningeal lymphatics are ablated, anti-amyloid antibody immunotherapy works worse, with more amyloid deposition, more microglial activation, and worse behavioral outcomes, while VEGF-C delivery improves antibody-driven amyloid clearance. R
This suggests the drainage route is part of why some Alzheimer's drugs underperform.
The handoff also breaks on the glymphatic side in Alzheimer's, because perivascular AQP4 localization is lost in the disease, which impairs clearance and promotes plaque formation. R R
For the broader Alzheimer's protocol I lean on the work I summarized in the Bredesen ReCODE protocol post.
Long COVID Brain Fog
Long COVID brain fog is increasingly described as a neuroinflammatory and neurovascular problem, not a psychological one.
Imaging of long COVID patients with cognitive impairment shows asymmetrical glymphatic dysfunction that correlates with blood-brain barrier (BBB) disruption. R
In the JD framework this is expected.
Jacob coined the terms Transient Capillary Leak Syndrome (TCLS) and Micro-Sepsis (MSS) to describe what happens when the glycocalyx, the sulfated sugar coat that lines blood vessels, lymphatic vessels, and immune cells, becomes degraded.
Once the glycocalyx is shed, tight junctions open, the barrier leaks, and the same inflammatory cascade that opens the BBB also degrades the lining of the drainage vessels themselves.
My full long COVID protocol is in the 7 steps to naturally treat long COVID post, and the deeper glycocalyx mechanics are in the glycocalyx and rebuilding the glycocalyx.
Traumatic Brain Injury
Even mild head trauma severely impairs meningeal lymphatic drainage, and the impairment starts within hours and lasts for at least a month after injury. R
Worse, mice with pre-existing meningeal lymphatic dysfunction before the injury had more neuroinflammation and worse cognitive outcomes afterward. R
This is one mechanistic bridge between a history of concussions and later cognitive decline, and it is a reason that pre-existing drainage health may set the ceiling on how well a brain recovers from any insult.
Physical neck and skull-base anatomy matters here too, because the deep cervical outflow runs through the neck, which is why I treat craniocervical instability as relevant to brain drainage and not just to pain.
How To Support Brain Drainage
You cannot inject VEGF-C into your own CSF, but most of the levers that move this system are behavioral.
The protocol below is ordered by leverage, not alphabetically, because these are sequential lifestyle priorities.

1. Sleep, And Sleep On Your Side
Glymphatic clearance is gated by sleep.
During natural sleep and under anesthesia, the interstitial space expands and the rate of amyloid-beta clearance roughly doubles compared to the awake state. R
Body position during sleep then changes how efficiently that clearance runs.
In a contrast-MRI study, glymphatic transport was most efficient in the lateral (side-lying) position compared to lying on the back or the stomach. R
Side sleeping is the cheapest brain-drainage intervention available.
For sleep depth I use a small dose of Melatonin, which I cover in the melatonin benefits post, and Glycine after a hot shower.
My full sleep approach is in my sleep experiments and how I get 3 to 4 hours of deep sleep every night.
2. Lower Sympathetic Tone Before Bed
The glymphatic system is switched off by adrenergic (noradrenaline) signaling.
Blocking adrenergic signaling increases glymphatic clearance, which is part of why deep sleep and anesthesia open the system while a racing, sympathetic-dominant nervous system keeps it closed. R
This is the JD connection that ties drainage to dysautonomia.
In post-viral illness the gut loses serotonin synthesis through the tryptophan and kynurenine shunt, the vagus loses its parasympathetic signal, and the body sits in sympathetic dominance, which I cover in the JD chapter on tryptophan, the kynurenine pathway, and the vagus nerve.
Lowering noradrenergic drive before bed (no screens or stimulants late, breathwork, magnesium) is not just calming, it is mechanically opening the drain.
Magnesium Glycinate before bed is my baseline, and Magnesium L-Threonate is the form that reaches the brain.
3. Exercise (Within Your Energy Envelope)
Voluntary exercise improves glymphatic clearance of amyloid-beta and reduces astrocyte and microglial activation in aged mice, partly by restoring AQP4 expression and polarization. R
This is not only an animal finding.
In humans, twelve weeks of cycle-ergometer training increased measures of both glymphatic and meningeal lymphatic vessel flow. R
The caveat for the chronically ill matters.
In the post-viral and POTS population, overexertion damages the glycocalyx and triggers post-exertional malaise, so the dose has to stay inside your energy envelope (see POTS root causes).
For this group, gentle and consistent movement beats hard training that you crash from.
4. Omega-3 Fatty Acids
Omega-3 polyunsaturated fatty acids promote amyloid-beta clearance from the brain, and the effect depends on the AQP4-based glymphatic system. R
In a TBI model, omega-3s also helped preserve AQP4 polarity and improved glymphatic drainage after injury. R
Fish Oil high in DHA is the practical way to get this, and DHA is also a structural component of the neuronal membrane.
5. Support The Cervical Outflow Route
The meningeal lymphatics drain through the base of the skull into the deep cervical lymph nodes in the neck. R
That means neck position and neck lymphatic flow sit directly on the exit path.
Manual lymphatic drainage of the neck, avoiding chronic forward-head posture, and addressing structural neck issues like craniocervical instability are reasonable ways to keep the downstream pipe open.
This is mechanistically sensible rather than heavily trialed, so treat it as a low-risk adjunct, not a proven cure.
6. Keep The Glycocalyx And Barrier Intact
This is the JD layer underneath everything above.
Meningeal lymphatic endothelium, like all endothelium, carries a glycocalyx, and in Jacob's framing the integrity of that coat is what determines whether the vessel can selectively absorb and transport fluid or whether it leaks and stalls.
Rebuilding the glycocalyx with high and low molecular weight sulfated polysaccharides such as Fucoidan, plus the broader protocol in rebuilding the glycocalyx, supports the same vascular and lymphatic linings that brain drainage depends on.
Reducing the endotoxin load that drives glycocalyx shedding in the first place is covered in how to inhibit lipopolysaccharides.
What To Stay Away From
These are the inputs that suppress the glymphatic-lymphatic handoff.
- Chronic sleep deprivation (clearance largely happens during sleep, so lost sleep is lost drainage) R
- Chronic sympathetic overdrive (sustained noradrenergic tone keeps the glymphatic system switched off) R
- Overexertion in post-viral illness (it damages the glycocalyx and triggers post-exertional malaise rather than helping)
- Unaddressed head trauma (even mild injury impairs meningeal drainage for weeks) R
- Untreated obstructive sleep apnea (it fragments the deep sleep the glymphatic system depends on)
Testing
There is no single clean clinical test of meningeal lymphatic flow yet, so this section combines an emerging imaging proxy with the inflammatory and barrier markers that sit upstream and downstream of drainage.
Imaging
The research proxy for glymphatic function is the DTI-ALPS index, a diffusion-MRI measure of water movement along perivascular spaces, which drops in long COVID patients with cognitive impairment and correlates with blood-brain barrier leak. R
This is a research and specialist tool right now, not a routine order, but it is the metric to watch as it moves toward the clinic.
Functional Lab Panels
I use the Neural Zoomer (Vibrant Wellness) to assess blood-brain barrier integrity, demyelination, and brain autoimmunity markers when drainage failure and neuroinflammation are suspected.
I use the Cardio Zoomer (Vibrant Wellness) to assess endothelial function and inflammatory markers, since the same vascular biology drives both peripheral and meningeal vessel health.
I use the Cellular Zoomer (Vibrant Wellness) to assess oxidative stress, mitochondrial function, and methylation, which is the redox layer that determines how fast the glycocalyx is shed.
For a broad baseline of CBC, metabolic, liver, and thyroid status I use the Foundation Zoomer (Vibrant Wellness).
When the picture is post-viral, the Long COVID bundle (Vibrant Wellness) pairs the cardio, toxin, gut, cellular, and viral panels in one pass.
Because mold and environmental toxins drive the same neuroinflammatory cascade, the Toxin Zoomer (Vibrant Wellness) is worth adding when exposure is on the table.
Genetics Panels
For the AQP4 and APOE variants below, 23andMe raw data plus an APOE add-on (Vibrant Wellness) covers the highest-yield markers.
Mechanisms Of Action
Simple:
- Your brain washes its own waste into the spinal fluid while you sleep, and the meningeal lymphatic vessels are the drainpipes that carry that dirty fluid out through your neck.
- Aging, head injury, poor sleep, and a stressed nervous system all slow those drainpipes, so waste like the proteins behind Alzheimer's builds up.
- Side sleeping, exercise, omega-3s, and a calm nervous system before bed all help the system run.
Advanced:
- Glymphatic influx and AQP4 polarization CSF enters the brain along periarterial spaces, exchanges with interstitial fluid, and exits along perivenous spaces, and this convective flux requires AQP4 channels concentrated at astrocyte endfeet, where loss of perivascular AQP4 polarization cuts solute clearance by roughly 70 percent and promotes amyloid plaque formation. R R
- Meningeal lymphatic uptake to deep cervical nodes LYVE-1 and PROX1 positive lymphatic endothelium in the dura absorbs CSF and macromolecules and transports them through skull-base foramina to the deep cervical lymph nodes, completing the route out of the CNS. R R
- VEGF-C and VEGFR-3 driven meningeal lymphangiogenesis VEGF-C signaling through VEGFR-3 maintains and expands meningeal lymphatic vessels, and delivering VEGF-C to aged mice restores vessel caliber, CSF perfusion, and drainage while improving cognition, whereas ablating these vessels worsens amyloid pathology and blunts anti-amyloid immunotherapy. R R
- Adrenergic gating of clearance noradrenergic tone constricts the interstitial space and suppresses glymphatic flux, so sleep and reduced adrenergic signaling expand interstitial volume and accelerate amyloid-beta clearance, linking sympathetic dominance directly to impaired brain drainage. R
- Trauma-induced lymphatic failure mild traumatic brain injury produces rapid and durable deficits in meningeal lymphatic drainage, and pre-existing lymphatic dysfunction amplifies post-injury neuroinflammation and cognitive deficit, identifying drainage reserve as a modifier of injury outcome. R
Genetics
AQP4
AQP4 encodes the aquaporin-4 water channel that astrocytes concentrate at their perivascular endfeet, where it powers glymphatic fluid exchange.
Variants in the gene do not abolish the channel but they shift how much amyloid the brain accumulates for a given amount of poor sleep.
In the AIBL cohort, several AQP4 single nucleotide polymorphisms moderated the relationship between sleep and brain amyloid-beta burden, with rs72878776 associated with poorer overall sleep quality and other variants altering how strongly disturbed sleep translated into amyloid load. R
rs72878776 is linked to poorer subjective sleep quality, a relevant background risk when glymphatic clearance already depends on sleep. R
rs9951307 and rs3875089 are among the variants that moderated how sleep latency and duration mapped onto amyloid accumulation. R
APOE (Highest Population Risk)
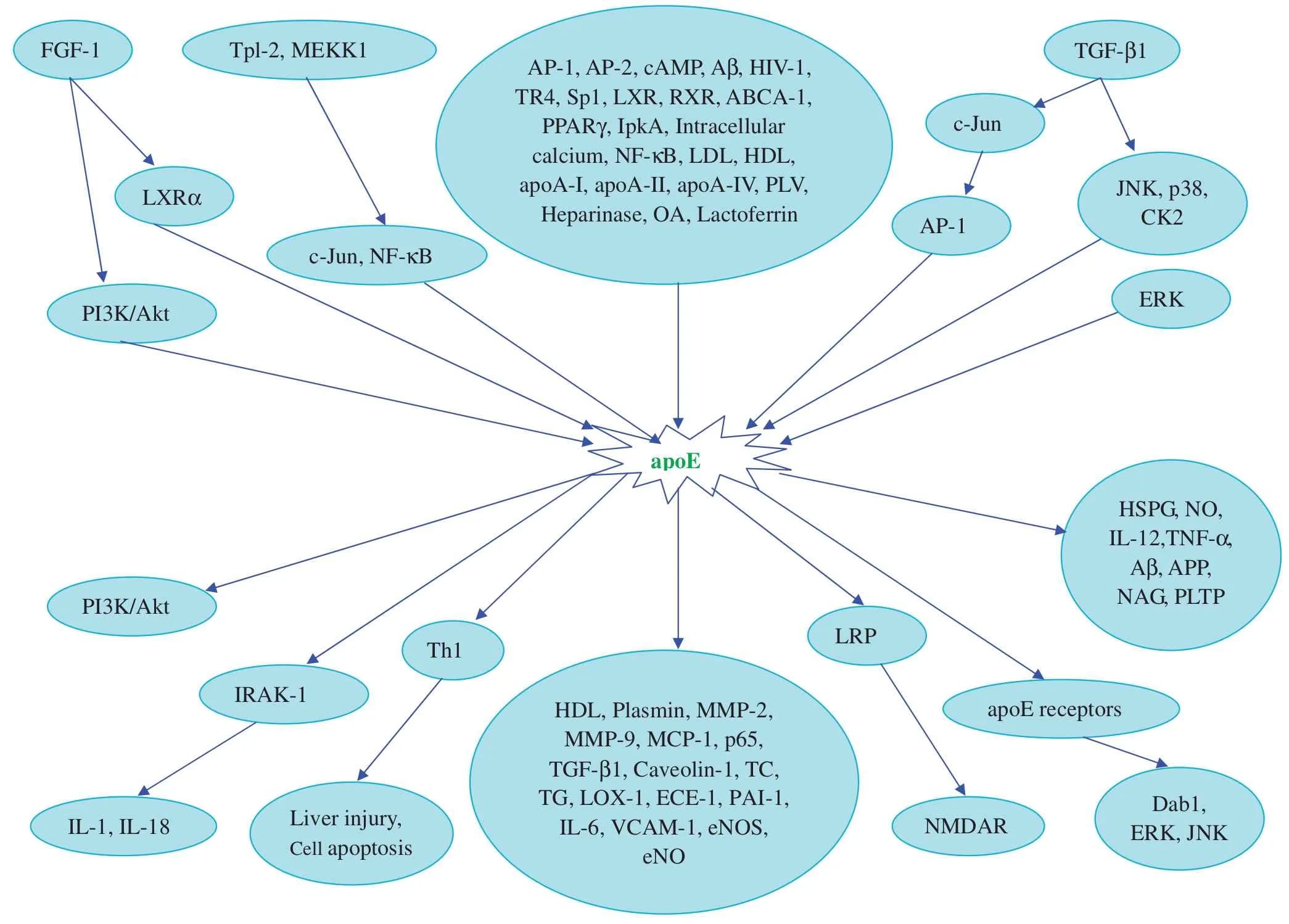
APOE encodes apolipoprotein E, the main lipid-transport protein in the brain and a strong determinant of amyloid handling.
The APOE4 variant is the largest common genetic risk factor for late-onset Alzheimer's, and it is associated with loss of perivascular AQP4 localization, the same depolarization that impairs glymphatic clearance and promotes plaque. R
rs429358 and rs7412 are the two variants that together define the APOE2, APOE3, and APOE4 alleles, and carrying APOE4 raises amyloid burden (covered in detail in the ApoE post).
More Research
The meningeal lymphatic field is young, and several questions are still open.
A central uncertainty is whether the human meningeal lymphatic system can be expanded therapeutically the way VEGF-C expands it in mice, since direct CSF delivery is not a consumer option and the durable human levers so far are sleep, exercise, and nervous-system regulation. R
Anti-amyloid immunotherapy appears to depend on intact drainage, which raises the unanswered clinical question of whether drainage-supporting behaviors change how well those drugs work in people. R
For brain-drainage and neuroinflammation testing I use the Neural Zoomer (Vibrant Wellness) for barrier and demyelination markers and the Cellular Zoomer (Vibrant Wellness) for the oxidative and methylation layer that governs glycocalyx turnover.
Glymphatic imaging via the DTI-ALPS index is the metric most likely to reach routine clinical use, and it already separates long COVID patients with cognitive impairment from those without. R
In the JD framework the meningeal lymphatics are one node in a larger fluid-handling story that also includes the interstitium, the glymphatic system, and the glycocalyx that lines every one of these vessels, and the JD chapter on lymph and the glymphatic system ties them together.
The role of astrocytes in neuroinflammation is the upstream layer that determines whether AQP4 stays polarized and the handoff keeps working.
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Electrolyte Complex
1 scoop/day
CoQ10
200mg/day
Magnesium Glycinate
400mg at bedtime