Epstein-Barr Virus Reactivation: Latency, Chronic Fatigue, Long COVID, And Multiple Sclerosis
By Jacob Gordon, INHC, FMT-CThis article contains affiliate links. As an Amazon Associate, MyBioHack earns from qualifying purchases at no extra cost to you. We only link products we research and stand behind.
Chronic Epstein-Barr Virus reactivation is one of the most dismissed drivers of long-term fatigue, even though almost every adult carries the virus for life.
In this post, we will discuss what EBV latency actually is, what "reactivation" means at the immune level, the real evidence tying it to ME/CFS and long COVID, the causal link to multiple sclerosis, why elevated antibody titers get waved away in the clinic, and what you can actually do to keep the virus quiet.

Basics Of EBV And Latency
Epstein-Barr Virus (EBV), also called human herpesvirus 4, is a gamma-herpesvirus that infects more than 90% of adults worldwide and then stays for life. R
Over 90% of healthy adults carry IgG antibodies to both the viral capsid antigen and the nuclear antigen, which is simply the serological fingerprint of a past infection that never fully left. R
Primary infection in adolescence or adulthood often presents as infectious mononucleosis, while childhood infection is usually silent.
After the acute phase, EBV does not get cleared like a cold.
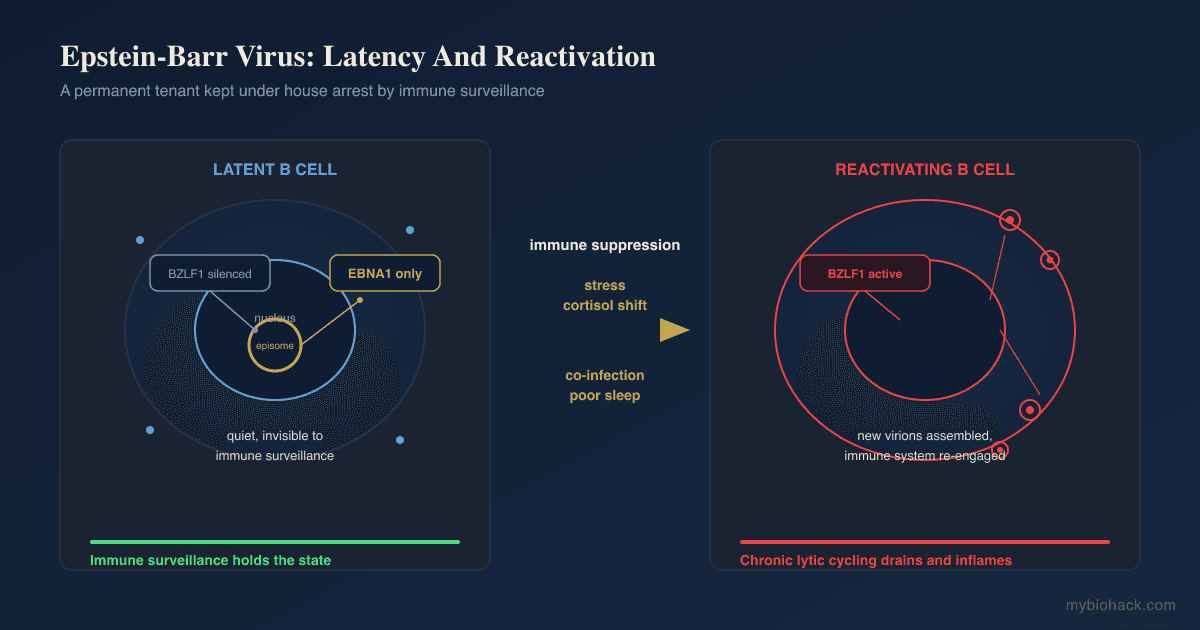
It goes latent inside memory B cells, switching off almost all of its genes to hide from the immune system. R
In the deepest latency programs, the virus expresses only Epstein-Barr Nuclear Antigen 1 (EBNA1), the one protein it needs to copy its genome along with the host cell while staying invisible. R
This is the key point most people miss: EBV is not an infection you "get over," it is a permanent tenant that your immune system spends the rest of your life keeping under house arrest.
When that immune surveillance weakens, the tenant starts moving around again.
What Reactivation Actually Means
Latency is not a static off-switch, it is an active state that the immune system and viral epigenetics hold in place. R
Reactivation is the flip from the latent program to the lytic cycle, where the virus starts making new viral particles again.
The switch is thrown by a single viral gene called BZLF1 (also known as Zta, ZEBRA, or Z), an immediate-early gene whose protein product is sufficient on its own to start the entire lytic cascade. R
BZLF1 turns on BRLF1, the two proteins amplify each other, and that kicks off early gene expression, viral DNA replication, late gene expression, and the assembly of new virions. R
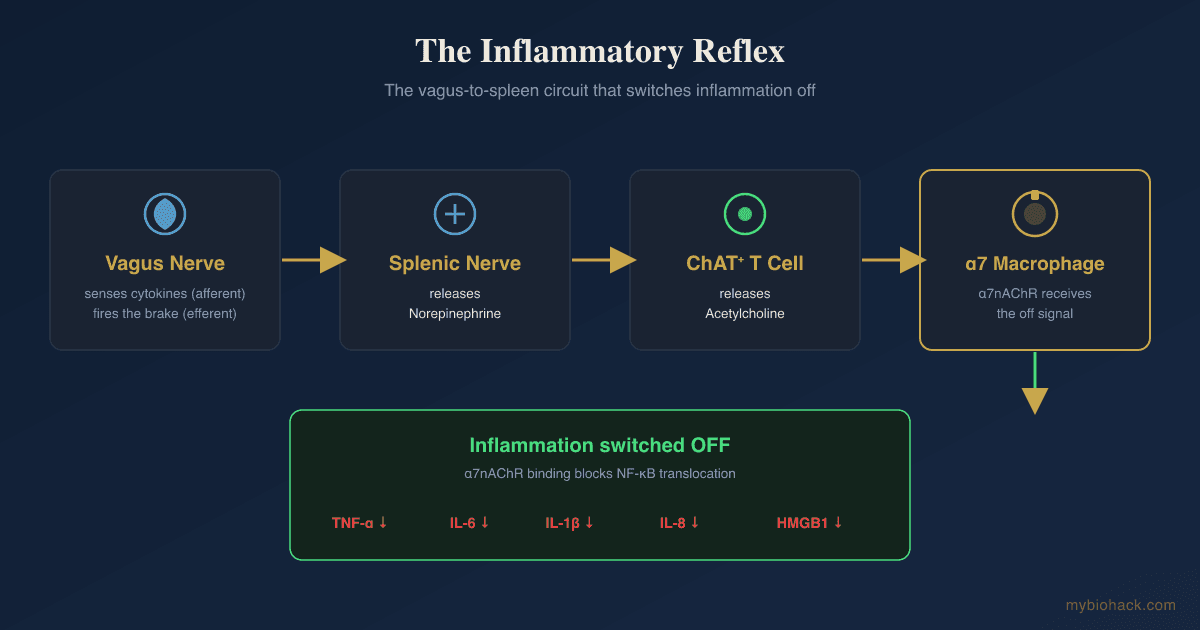
In a healthy person this happens quietly in the throat and gets mopped up by cytotoxic T cells and natural killer cells before it causes trouble.
In someone whose immune system is distracted, exhausted, or suppressed, the lytic program runs harder and longer.
That is what "chronic reactivation" means: not a dramatic new mononucleosis, but a smoldering, repeated re-expression of viral proteins that keeps the immune system agitated and burns through resources.
The triggers are the usual suspects that lower cell-mediated immunity: physical or emotional stress, other infections, poor sleep, sustained cortisol dysregulation, and immunosuppression. R
This is exactly why a second infection like COVID can wake up a virus you caught twenty years ago.

The Evidence In ME/CFS And Long COVID
The link between EBV reactivation and post-viral fatigue is one of the oldest and most reproduced observations in the field.
Antibody-secreting memory B cells specific to EBNA1 and the viral capsid antigen are diminished or absent in up to 76% of chronic fatigue syndrome patients, which points to a specific hole in the immune system's ability to police the virus. R
That study framed it precisely: a deficient EBV-specific B-cell and T-cell memory response, and an impaired ability to control the early steps of reactivation. R
A large body of work has proposed EBV as a driver in a genetically susceptible subset of Myalgic Encephalomyelitis / Chronic Fatigue Syndrome (ME/CFS), particularly in people carrying certain HLA class II alleles. R
Long COVID pushed this from a fringe idea into mainstream immunology.
In one early study, 66.7% of long COVID subjects versus 10% of controls were positive for EBV reactivation based on early antigen-diffuse IgG or viral capsid antigen IgM, suggesting many long COVID symptoms may come from inflammation-triggered EBV reactivation rather than the coronavirus itself. R
A much larger immune-profiling study published in Nature then found that long COVID patients show elevated antibody responses against EBV alongside reduced cortisol, and that these features were strong enough to help distinguish long COVID from recovered controls with machine learning. R
The mechanism is not mysterious.
An acute viral infection, systemic inflammation, and a stress-driven cortisol shift all suppress the cell-mediated immunity that normally keeps EBV latent, and the virus takes the opening.
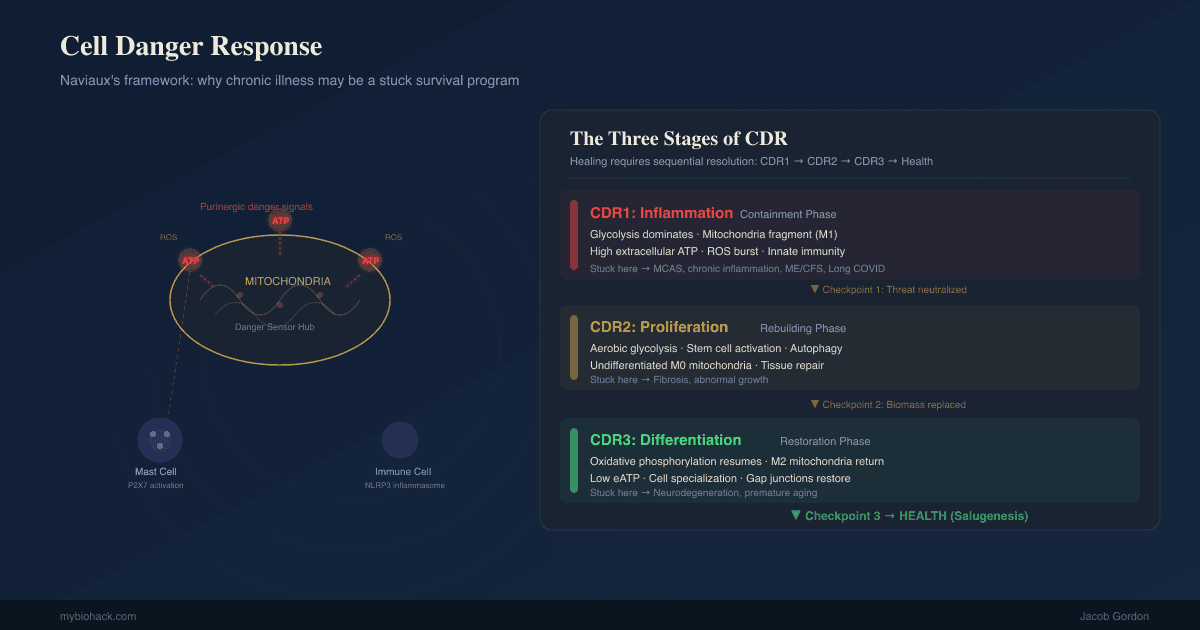
This overlaps heavily with the long COVID recovery picture and with the broader cell danger response that keeps post-viral patients stuck in a defensive metabolic state.
The EBV And Multiple Sclerosis Causal Link
For decades EBV was "associated" with multiple sclerosis, and association is easy to dismiss.
In 2022 that changed.
A longitudinal analysis of more than 10 million young adults in the US military, using stored serum samples taken every two years, found that the risk of multiple sclerosis increased 32-fold after EBV infection, and was not increased after infection with other viruses including the similarly transmitted cytomegalovirus. R
Serum neurofilament light chain, a marker of nerve damage, only rose after EBV seroconversion, not before. R
This is about as close to causal evidence as observational human data gets: the virus came first, the nerve damage followed, and nearly everyone who developed MS had seroconverted to EBV beforehand.
It does not mean EBV alone causes MS, since almost everyone carries EBV and only a fraction develop MS.
It means EBV is very likely a necessary upstream trigger, and that host susceptibility and ongoing reactivation decide who progresses.
That reframing matters for anyone with a chronic EBV picture: this is not a harmless passenger virus.
Why Doctors Dismiss Elevated Titers
Here is where patients and conventional medicine collide.
You get an EBV panel back showing high viral capsid antigen IgG, positive EBNA1 IgG, and elevated early antigen antibodies, you feel terrible, and your doctor says it is normal.
They are not entirely wrong, and understanding why is important.
Because over 90% of adults carry VCA and EBNA IgG, those two markers on their own only prove you were infected at some point, which is true for almost everyone. R
The standard interpretation guides treat the combination of positive VCA IgG, positive EBNA IgG, and elevated early antigen as "past infection with non-specific immune activation," not a discrete clinical disease. R
The evidence-based position is genuinely mixed: one analysis noted that only about 3% of sera with elevated early antigen antibodies actually show detectable EBV DNA by PCR, which is why titers alone are considered weak proof of active viral replication. R
So there is a real MAYBE here.

Elevated early antigen and VCA IgM can reflect true subclinical reactivation, or they can reflect non-specific polyclonal immune activation from some other inflammatory driver.
The honest reading is that antibody titers are a signal, not a verdict.
The mistake conventional medicine makes is going from "titers cannot confirm active disease" to "your symptoms are unrelated," which is a different and unjustified leap, especially given the ME/CFS, long COVID, and MS data above.
The mistake patients make is treating a single high VCA IgG as proof of raging chronic infection when almost everyone has one.
A rising early antigen titer over time, an unexpected VCA IgM in someone with old infection, or a serology pattern that tracks with symptom flares is far more meaningful than any single number.
EBV And Overlapping Conditions
Chronic EBV reactivation rarely travels alone, because the thing that lets it reactivate (weakened cell-mediated immunity) also lets other latent and opportunistic problems surface.
Conditions that cluster with chronic EBV reactivation (not an exclusive list):
- Autoimmune conditions including multiple sclerosis, lupus, and Hashimoto's, where serologic markers of EBV reactivation track with disease activity and interferon-pathway activation R
- Histamine intolerance and mast cell activation, driven by the same inflammatory and hypoxic terrain
- Long COVID and post-viral syndromes, where EBV reactivation is a documented feature R
- Mold and biotoxin illness (CIRS), where immune suppression opens the door to latent viral expression
- Myalgic Encephalomyelitis / Chronic Fatigue Syndrome, the most studied EBV-linked fatigue syndrome R
In Jacob's Junction Dysfunction (JD) framework, this clustering is not a coincidence.
Latent viruses like EBV are covered directly in the Latent Viruses chapter of the JD guide.
Jacob's hypothesis is that a state he calls Micro-Sepsis (MSS), a chronic sub-lethal version of sepsis, drives an acute immune hyperactivation followed by chronic immunosuppression, and it is that immunosuppressed window that allows latent infections to express and co-infections to accumulate.
You can read that model in the Junction Dysfunction and Micro-Sepsis chapter.
The relevant takeaway for this post is mechanistic and modest: chronic inflammation suppresses the immune arm that holds EBV latent, EBV reactivation then reinforces the inflammation, and the loop is self-sustaining.
How To Reduce Reactivation
The goal is not to "kill" EBV, which is impossible once latent, it is to restore the immune surveillance that keeps it latent and to remove the inflammatory triggers that keep flipping the lytic switch.
1. Fix Sleep, Stress, And Cortisol First
Nothing on a supplement list matters if cortisol is dysregulated and sleep is broken, because that is the primary suppressor of anti-EBV immunity.
Reduced cortisol was the single strongest distinguishing feature of long COVID in the Nature immune-profiling data, and stress-driven cortisol shifts are a classic reactivation trigger. R
Prioritize circadian alignment, morning light, and consistent sleep before anything else.
Melatonin supports both sleep and circadian repair, and its role goes well beyond sedation as covered in the melatonin deep-dive.
2. Support Cell-Mediated And NK Immunity
The immune cells that keep EBV latent are T cells and natural killer cells, so the entire strategy is about supporting them rather than blunting inflammation blindly.
Vitamin D is foundational for T-cell function, and most chronically ill people are low, though it needs the right cofactors to convert properly. R
Zinc is required for T-cell development and antiviral defense, best dosed with attention to copper and ceruloplasmin balance. R
Selenium supports glutathione peroxidase and antiviral immunity, and selenium deficiency raises the viral genome mutation rate and worsens outcomes in animal models of RNA viral infection. R
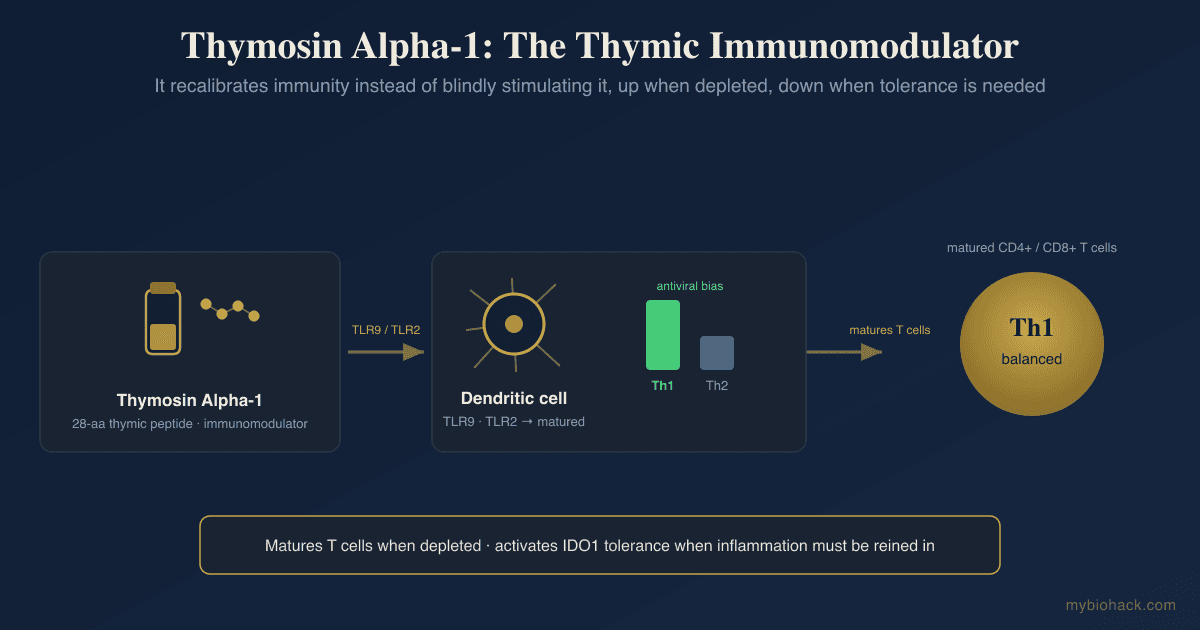
Thymus peptides are worth understanding here, since thymosin alpha-1 and the broader thymosin peptide family are used specifically to rebuild cell-mediated immunity in chronic viral states.
3. Lower The Lysine To Arginine Ratio
Herpesviruses depend on arginine to replicate, and lysine competitively antagonizes that arginine-driven replication.
In tissue culture, lysine supplementation reduced herpesvirus replication by up to 54% in an arginine-dependent, ratio-dependent way. R
The evidence is strongest for herpes simplex rather than EBV specifically, so treat this as a low-risk adjunct, not a cure.
L-Lysine is the practical lever, and it pairs logically with avoiding large arginine boluses during a flare.
4. Use Targeted Antiviral And Immunomodulatory Botanicals
Several plant compounds have direct antiviral or immune-restoring activity relevant to herpesviruses.
Monolaurin disrupts the lipid envelope of enveloped viruses.
Quercetin and Curcumin modulate the NF-kB signaling that EBV exploits during reactivation, and curcumin specifically inhibits transcription of the lytic-switch gene BZLF1 while quercetin shows direct antiherpetic activity in vitro. R R
Sulforaphane from broccoli sprouts activates NRF2, and its broader benefits are covered in the sulforaphane deep-dive.
Reishi and other medicinal mushrooms support NK-cell and T-cell activity. R
5. Consider Prescription Antivirals Where Evidence Exists
This is a physician decision, not a supplement.
In a blinded, placebo-controlled trial, valacyclovir improved a validated energy index in the EBV subset of chronic fatigue syndrome, with the benefit concentrated in patients selected by EBV serology rather than everyone. R
Valacyclovir only works against the lytic (replicating) phase, not latent virus, which is exactly why patient selection by active-reactivation markers matters.
When there is co-infection with cytomegalovirus or HHV-6, some protocols add valganciclovir, again under physician supervision, and a randomized trial of valganciclovir in CFS patients selected for elevated HHV-6 and EBV titers found significant improvement in fatigue and cognitive subscores versus placebo. R
Low-dose naltrexone is a separate, well-tolerated immunomodulatory option many post-viral patients use to calm the inflammatory side of this loop.
6. Address The Gut And Inflammatory Terrain
Because systemic inflammation is what flips the switch, calming the gut-driven inflammatory load reduces the reactivation pressure.
Correcting dysbiosis removes one of the chronic inflammatory inputs that suppresses antiviral immunity.
This is the same terrain work that underlies the long COVID protocol.
What To Stay Away From
(not exclusive list)
- Arginine loading during a flare: high-dose L-arginine and NO-booster pre-workouts feed herpesvirus replication and can reactivate latent virus, which is a specific caution in the post-viral population
- Blind immunosuppression: reflexively suppressing every inflammatory marker can remove the very immune activity that is trying to control the virus
- Chasing a single high titer: do not build an aggressive protocol around one elevated VCA IgG, since almost everyone has one
- Chronic sleep deprivation and unmanaged stress: these are the dominant cortisol-mediated reactivation drivers, and no supplement offsets them
- Overtraining: intense exercise while symptomatic opens a well-documented post-exercise window of reduced NK-cell and T-cell surveillance, so pushing through post-exertional malaise is counterproductive R
Testing
Testing has two jobs here: confirm the serological pattern, and characterize the terrain that is allowing reactivation.
Blood And Urine Markers
EBV Viral Capsid Antigen (VCA) IgG confirms past infection but does not indicate activity on its own, since more than 90% of adults are positive. R
EBV VCA IgM suggests recent primary infection or, in someone with old infection, possible reactivation.
EBV Nuclear Antigen (EBNA1) IgG appears months after primary infection and indicates established, non-acute infection. R
EBV Early Antigen-Diffuse (EA-D) IgG is the marker most associated with active or recent reactivation, though only a minority of elevated results correlate with detectable viral DNA, so it should be read as a signal rather than proof. R
EBV DNA PCR in whole blood or plasma is the most specific test for active replication when reactivation is genuinely suspected.
The single most useful move is to trend these over time and correlate them with symptom flares, rather than reading one snapshot.
Functional Lab Panels
I use the Viral Infections Panel (Vibrant Wellness) to assess EBV alongside other reactivated herpesviruses like HHV-6 and CMV in one snapshot.
I use the Long COVID bundle (Vibrant Wellness) when reactivation sits on top of a post-viral picture, since it pairs the viral panel with cardiovascular, toxin, gut, and cellular markers.
For the immune and inflammatory terrain driving reactivation, I use the Immune Zoomer (Vibrant Wellness) to map autoantibodies and immune reactivity.
For the fatigue and mitochondrial side, I use the Cellular Zoomer (Vibrant Wellness) to look at organic acids, oxidative stress, and mitochondrial function.
Multi-point cortisol matters here, so I use the Hormone Zoomer (Vibrant Wellness) or the DUTCH Complete (Precision Analytical) to capture the cortisol rhythm rather than a single misleading morning value.
For anyone who wants this interpreted in context rather than in isolation, a consultation is the fastest way to connect the serology to the terrain.
Mechanisms Of Action
Simple:
- EBV hides for life inside your immune cells, and it only causes trouble when your immune system gets too weak or distracted to keep it asleep.
- Things like infection, stress, bad sleep, and low cortisol pull your immune guards off duty, the virus wakes up and starts copying itself, and that keeps your immune system inflamed and drained.
Advanced:
- Latency maintenance and the lytic switch: EBV persists in memory B cells expressing minimal genes, often only EBNA1 driven from the Qp promoter, with BZLF1 silenced by cellular repressors and epigenetic marks; reactivation requires derepression of BZLF1, whose product Zta is alone sufficient to trigger the immediate-early to early to late lytic cascade and new virion production. R
- IDO and the kynurenine shunt: EBV infection induces indoleamine 2,3-dioxygenase in monocyte-derived macrophages through p38/MAPK and NF-kB, driven by TNF-alpha and IL-6, which shunts tryptophan down the kynurenine pathway, impairs T-cell function, and creates an immunosuppressive microenvironment that favors viral persistence. R
- Immune-suppression permissiveness: reactivation is gated by cell-mediated immunity, so any state that reduces cytotoxic T-cell and NK surveillance, including cortisol dysregulation and competing infection, lowers the threshold for the lytic program, which is the immunological basis for reactivation observed in long COVID. R
- Neurofilament and downstream nerve injury: in the MS cohort, neurofilament light chain rose only after EBV seroconversion, tying EBV activity temporally to neuroaxonal degeneration rather than the reverse. R
Genetics
HLA Class II (HLA-DRB1 / HLA-DQB1)
The HLA class II genes encode the molecules that present viral peptides to CD4 T cells, setting how well your immune system recognizes EBV.
Certain HLA class II alleles are over-represented in EBV-linked ME/CFS and in multiple sclerosis, suggesting inefficient EBV antigen presentation in susceptible people. R
HLA-DRB1*15:01 is the best-known MS risk allele and interacts with EBV exposure to raise risk further.
IFITM3
Interferon-Induced Transmembrane Protein 3 (IFITM3) restricts entry of enveloped viruses into cells.
Variants that reduce IFITM3 function are linked to more severe viral infection and, plausibly, weaker early control of reactivating virus.
rs12252 (C allele) is associated with more severe viral illness in some populations, though meta-analyses are mixed. R
OAS1
2'-5'-Oligoadenylate Synthetase 1 (OAS1) activates the RNase L antiviral pathway that degrades viral RNA.
Lower-activity variants blunt this innate antiviral response.
rs10774671 sits in a splice-acceptor site and determines which OAS1 isoform is produced, with the derived A allele generating lower-activity isoforms. R
More Research
Antibody interpretation is genuinely unsettled, since elevated early antigen titers correlate with detectable EBV DNA only a minority of the time, so serology should always be read alongside symptoms and, ideally, PCR. R
Autoantibody mimicry is an active research area, and a 2022 Nature paper showed high-affinity molecular mimicry between EBV EBNA1 and the CNS protein GlialCAM, giving a concrete mechanism by which anti-EBV antibodies can cross-react with self-tissue in multiple sclerosis. R
EBV-targeted cell therapy is advancing on the MS side, where a phase I trial of autologous EBV-specific T cells targeting EBNA1, LMP1, and LMP2A produced clinical improvement in a subset of progressive MS patients, an approach that may eventually inform chronic reactivation treatment. R
For testing in practice, I use the Viral Infections Panel and the Long COVID bundle to characterize reactivation, and I trend serology against symptoms rather than treating any single titer as decisive.
Valacyclovir responders are a defined subset, not the whole fatigue population, so the trial data argue for selecting patients by active-reactivation markers rather than treating everyone with elevated lifelong IgG. R
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Quercetin
500mg 2x/day
Vitamin D3 + K2
5000 IU + 200mcg/day
Magnesium Glycinate
400mg at bedtime