Parasites And Biliary Health: What Lives In Your Bile Ducts And What To Do About It
By Jacob Gordon, INHC, FMT-CThis article contains affiliate links. As an Amazon Associate, MyBioHack earns from qualifying purchases at no extra cost to you. We only link products we research and stand behind.
Parasites of the biliary tract are far more common than most Western clinicians appreciate, and they are a frequently overlooked cause of gallbladder symptoms, gallstone formation, recurrent right upper quadrant pain, and cholangitis.
In this post, we will discuss which parasites directly inhabit or damage the biliary tree, what they do mechanically and immunologically to bile duct tissue, how they drive gallstone formation and cholangiocarcinoma risk, and how to treat them with both pharmaceutical and herbal antiparasitic agents including the CellCore Para protocol.

Basics: Parasites And The Biliary Tree
The biliary tree is not as sterile as once assumed.
Biliary parasites are organisms that either reside permanently in the bile ducts and gallbladder, or migrate there from the intestine, causing obstruction, inflammation, and chronic tissue damage. R
These infections are among the most common causes of biliary obstruction in tropical and subtropical countries and are increasingly encountered in Western populations due to travel, immigration, and global food supply chains. R
Many patients are asymptomatic for years or decades.
When symptoms do occur, they closely mimic cholecystitis, gallstones, and functional biliary disorders, leading to frequent misdiagnosis. R
The key finding that should raise clinical suspicion in any population is peripheral eosinophilia: a sustained elevation of eosinophils in a complete blood count, particularly in anyone with unexplained GI symptoms, right upper quadrant pain, or elevated liver enzymes. R
Common symptoms of biliary parasitic infection include: (not exclusive list)
- Biliary colic-type pain triggered by fatty meals
- Cholangitis (fever, jaundice, right upper quadrant pain)
- Chronic fatigue and malaise
- Eosinophilia on CBC (often the only initial lab finding)
- Elevated liver enzymes (AST, ALT, GGT, ALP)
- Episodic nausea and vomiting
- Intrahepatic bile duct dilatation on imaging
- Jaundice (obstructive, in heavy infections)
- Right shoulder referred pain
- Urticaria or skin rash (in acute/migratory phase)
Primary Biliary Parasites
Ascaris lumbricoides
Ascaris lumbricoides is the most common helminth infection in humans globally, with an estimated 1 billion infections worldwide. R
It normally resides in the small intestine (jejunum), but is actively motile and can enter the bile duct through the ampulla of Vater when host conditions change (fever, heavy worm burden, gastric acid changes, certain medications).
Once inside the common bile duct, Ascaris causes biliary obstruction, biliary colic, obstructive jaundice, and acute cholangitis.
Adult worms are large (15-35cm), and their presence in the bile duct is visible on ultrasound as parallel echogenic lines (the "double tube sign") or on ERCP as worm-shaped filling defects. R
Ascaris is a cause of pigment gallstone formation: dead worm fragments and eggs serve as the nidus around which calcium bilirubinate precipitates. R
Ascaris eggs and fragments have been found as the nidus of 10-66% of intrahepatic stones in endemic areas. R
Transmission: Fecal-oral, through contaminated soil, water, and unwashed produce.
Primary treatment: Albendazole 400mg single dose, or mebendazole 100mg twice daily for 3 days. R
When worms are impacted in the bile duct, ERCP (endoscopic retrograde cholangiopancreatography) with extraction is required before or alongside antiparasitic therapy.
Clonorchis sinensis
Clonorchis sinensis is the oriental liver fluke, endemic to Northeast China, Korea, Taiwan, and Vietnam. R
It infects humans through ingestion of raw or undercooked freshwater fish containing metacercariae (encysted larvae).
After ingestion, metacercariae are released in the duodenum, migrate through the ampulla of Vater, and mature into adult flukes in the peripheral small intrahepatic bile ducts, where they can live for 15-25 years. R
Adult flukes measure 8-15mm in length. R
Chronic infection causes: R
- Bile duct inflammation (cholangitis)
- Bile duct wall thickening and fibrosis
- Intrahepatic stone formation (the flukes serve as nidus)
- Peripheral intrahepatic bile duct dilatation (without obstruction of large ducts)
- Recurrent pyogenic cholangitis
- Cholangiocarcinoma (classified as Group 1 carcinogen by IARC for this association) R
This is not a subtle risk: long-term Clonorchis infection carries a well-documented, statistically significant increase in cholangiocarcinoma risk. R
It is increasingly diagnosed in non-endemic regions in people with travel history or who consume imported freshwater fish products. R
Primary treatment: Praziquantel 25mg/kg three times daily for 1-2 days (the drug of choice). R
Alternative: Albendazole 400mg three times daily for 7 days (lower cure rates than praziquantel). R
Opisthorchis viverrini And Opisthorchis felineus
Opisthorchis viverrini is endemic to Southeast Asia (Thailand, Laos, Cambodia, Vietnam). R
Opisthorchis felineus is prevalent in Siberia, Eastern Europe, and parts of Central Asia. R
Both are closely related to Clonorchis sinensis in life cycle, transmission (raw freshwater fish), and hepatobiliary pathology.
They reside in the peripheral intrahepatic bile ducts and cause the same spectrum of complications: cholangitis, bile duct wall thickening, bile duct dilatation, and cholangiocarcinoma. R
O. viverrini infection is the primary driver of cholangiocarcinoma in Thailand, where the cancer has an incidence 40 times higher than in Western countries in heavily endemic northeastern regions. R
Primary treatment: Praziquantel 25mg/kg three times daily for 1-2 days. R
Biliary abnormalities can reverse after treatment. R
Fasciola hepatica And Fasciola gigantica
Fasciola hepatica (the common liver fluke, a cattle and sheep parasite) is transmitted to humans through ingestion of metacercariae on raw aquatic plants, primarily watercress and other water vegetables. R
Fasciola gigantica is prevalent in Africa and Asia and has a similar pathology.
Fascioliasis has two phases:
Hepatic phase (acute): Larvae migrate through the intestinal wall into the peritoneal cavity and penetrate the liver capsule, migrating through hepatic parenchyma toward the bile ducts over 2-4 months.
This phase causes fever, hepatomegaly, right upper quadrant pain, eosinophilia, and elevated liver enzymes, and on imaging appears as multiple small necrotic tracts or "tunnels" through the liver parenchyma. R
Biliary phase (chronic): Adult flukes (20-40mm, significantly larger than Clonorchis or Opisthorchis) R enter the bile ducts and cause:
- Fibrosing cholangitis
- Biliary colic
- Bile duct dilatation
- Hemobilia in some cases
- Obstructive jaundice
A critical pharmacological note: Fasciola hepatica is resistant to praziquantel. R
This is one of the most important drug-parasite mismatches to be aware of: treating fascioliasis with praziquantel will fail. R
Primary treatment: Triclabendazole 10mg/kg as a single dose (or split into two doses 12 hours apart for heavy infections). R
Triclabendazole was FDA-approved in the US in 2019 and is effective against both immature and adult Fasciola with cure rates up to 92%. R
It is available through the CDC Drug Service in the US under an investigational protocol when not commercially available.
Alternative: Nitazoxanide 500mg twice daily for 7 days (60% cure rate in adults). R
Side effects of triclabendazole treatment often include colicky biliary pain 3-7 days post-treatment, consistent with the dying flukes being expelled through the bile ducts.
Dicrocoelium dendriticum
Dicrocoelium dendriticum (the lancet liver fluke) has an unusual two-intermediate-host life cycle involving land snails and ants, rather than aquatic hosts.
Human infection occurs through accidental ingestion of infected ants, usually on raw vegetables or herbs from fields with grazing ruminants. R
It is globally distributed and often asymptomatic at low worm burdens.
Heavy infections cause cholangitis, bile duct thickening, and hepatomegaly similar to Clonorchis.
Primary treatment: Praziquantel 25mg/kg three times daily for 1 day. R
Giardia lamblia (Biliary Involvement)
Giardia is primarily an intestinal parasite but can migrate into the bile ducts and gallbladder, particularly in heavy infections or immunocompromised hosts. R
Biliary giardiasis causes a clinical picture that can mimic cholecystitis with chronic right upper quadrant discomfort, nausea, and bile duct dysfunction.
It is more common than recognized because stool microscopy often misses it and serology testing is required for confirmation.
Primary treatment: Metronidazole 250mg three times daily for 5-7 days, or tinidazole 2g single dose. R
How Biliary Parasites Damage The Liver And Bile Ducts
All biliary flukes share a common pathological mechanism: physical presence plus inflammatory response plus bile flow disruption.
The flukes themselves cause direct mechanical damage to bile duct epithelium (cholangiocytes) through their suckers, teguments, and excretory-secretory products. R
The immune response to chronic fluke presence drives: R
- Adenomatous hyperplasia of the bile duct epithelium (goblet cell metaplasia)
- Fibrosis of the bile duct wall
- Periductal fibrosis extending into liver parenchyma
- Cholestasis from both mechanical obstruction and impaired bile secretion
Impaired bile acid secretion by damaged cholangiocytes changes the bile acid composition, reduces the bile acid pool, and creates the same lithogenic environment as other causes of biliary disease. R
Gallstone formation from biliary parasites occurs through two mechanisms:
- Worm fragments, eggs, and dead parasite remnants serve as crystallization nidi for calcium bilirubinate in pigment stones.
- Beta-glucuronidase produced by bacteria that superinfect the damaged bile ducts deconjugates bilirubin, releasing free bilirubin that binds calcium to form pigment stones (the same mechanism as dysbiosis-driven stone formation).
Bacterial superinfection of the biliary tree is a direct consequence of the disrupted mucosal barrier: organisms like E. coli, Klebsiella, Enterococcus, Pseudomonas, and Bacteroides establish in bile ducts damaged by flukes, causing pyogenic (pus-producing) cholangitis. R
Cholangiocarcinoma develops in long-standing infections through a sequence of: chronic inflammation, cholangiocyte DNA damage from fluke metabolites, goblet cell metaplasia, progressive dysplasia, and malignant transformation. R
The IARC formally classifies Clonorchis sinensis and Opisthorchis viverrini as Group 1 biological carcinogens (definite human carcinogens) on the basis of this well-established progression. R
Conditions Linked To Biliary Parasitic Infection
Gallbladder sludge and gallstones are direct downstream consequences of biliary fluke infection. Understanding the parasite contribution to bile lithogenicity is a missing piece for many patients who form stones without obvious metabolic drivers.
Recurrent pyogenic cholangitis (RPC), also called Oriental cholangiohepatitis, is a syndrome of recurrent biliary infections, intrahepatic stones, and bile duct strictures that is directly caused by the biliary fluke-bacterial superinfection cycle. It is common in East Asia and increasingly seen in immigrant populations. R
Dysbiosis is both a predisposing factor and a consequence of biliary parasitism. Fluke infections disrupt the gut-liver axis, alter bile acid composition delivered to the colon, and create conditions where pathogenic bacteria proliferate. Fixing dysbiosis without addressing a parasitic burden means rebuilding on an unstable foundation.
Mycotoxin illness and CIRS frequently co-occur with parasitic burden. Compromised bile flow from fluke obstruction reduces the body's ability to excrete fat-soluble toxins including mycotoxins via bile. This creates a situation where both the parasite and the toxin load must be addressed simultaneously to restore biliary function.
Histamine intolerance is driven partly by dysbiosis resulting from parasitic gut disruption. Parasite-associated bacterial overgrowth increases histidine decarboxylase (HDC) activity and histamine production.
Mast cell activation is provoked by parasitic infection through direct mast cell degranulation from parasite antigens and excretory-secretory products. This is part of why active parasitic infections can trigger widespread inflammatory and allergic-type symptoms beyond the GI tract.
Eosinophilic esophagitis and eosinophilic GI disorders have parasitic infection as one legitimate upstream driver, since eosinophils are the primary anti-parasitic immune effector cell.
Nutritional deficiencies are common in helminth infections: Ascaris and hookworms compete for iron, B12, and fat-soluble vitamins directly.
Medical Antiparasitics: What Works For What
The matching of drug to parasite is critical because efficacy profiles diverge significantly.
Praziquantel
Praziquantel is the gold-standard broad-spectrum trematocide and cestocide. R
Mechanism: Increases cell membrane permeability to calcium in helminths, causing sustained muscular contraction followed by paralysis. It also disrupts the tegument (outer surface) of flukes, exposing them to immune attack. R
Covers: Clonorchis sinensis, Opisthorchis viverrini/felineus, Dicrocoelium dendriticum, Schistosoma species, Paragonimus, most tapeworm infections. R
Does NOT cover: Fasciola hepatica (resistance), hydatid disease, larval cestode cysts. R
Standard biliary dosing: 25mg/kg three times daily for 1-2 days for liver flukes. R
Absorption: Greater than 75%, enhanced by carbohydrate-rich meals. R
Adverse effects: Dizziness, drowsiness (do not drive), nausea, headache, abdominal discomfort. Most side effects are mild and related to dying worms. Rarely, allergic/anaphylactic reactions. R
Avoid in: Ocular cysticercosis (can damage the eye via local inflammation from dying cysts), pregnancy (first trimester caution), poor hepatic function.
Albendazole
Albendazole is the primary broad-spectrum nematocide with activity against many cestodes and some trematodes. R
Mechanism: Inhibits tubulin polymerization, blocking microtubule formation. This disrupts cell division and glucose uptake in parasites, causing vermicidal, larvicidal, and ovicidal effects. R
Covers: Ascaris (first line), hookworm, whipworm, strongyloidiasis, hydatid disease (long-term suppression), Clonorchis/Opisthorchis (lower efficacy than praziquantel, used as alternative). R
For biliary Ascaris: Single 400mg dose, or 400mg twice daily for 3 days if severe infection.
Absorption: Less than 5% absorbed orally when fasting. Significantly enhanced by high-fat meals. R
This is why taking albendazole with a fatty meal is clinically important, not optional.
Adverse effects: Generally well-tolerated for short courses. Prolonged use (more than 14-28 days) can cause liver enzyme elevation, neutropenia, and rarely cholestatic liver injury. R
Avoid in: Cirrhosis, pregnancy (teratogenic, avoid first trimester), previous benzimidazole hypersensitivity.
Triclabendazole
Triclabendazole is the drug of choice for fascioliasis and the only pharmaceutical reliably effective against Fasciola hepatica. R
It is also effective against Paragonimus (lung fluke).
Mechanism: Inhibits tubulin-based microtubule polymerization similar to albendazole, but with specific activity against both immature and adult Fasciola stages, which is why it works where albendazole fails for acute fascioliasis. R
Dosing: 10mg/kg as a single dose taken with food (bioavailability significantly improved with food). May be split into two doses of 10mg/kg given 12 hours apart for heavy infections. R
Efficacy: Up to 92% cure rate, though resistance has been documented in livestock in Western Europe, and retreatment is sometimes necessary. R
Adverse effects: Colicky biliary pain (3-7 days post-treatment, caused by dead flukes passing through the bile ducts), transient liver enzyme elevation. R
US access: FDA-approved in 2019 (Egaten). Available through CDC Drug Service via investigational protocol when not stocked commercially.
Mebendazole
Mebendazole shares the same benzimidazole mechanism as albendazole (microtubule disruption) and covers a similar spectrum with some differences.
It is used for Ascaris, hookworm, whipworm, and pinworm, and is an alternative for some biliary infections when albendazole is unavailable. R
For Clonorchis, multiple dose albendazole (400mg three times daily for 7 days) is generally preferred over mebendazole for biliary flukes, as mebendazole has lower tissue penetration. R
Standard dosing for Ascaris: 100mg twice daily for 3 days, or 500mg single dose.
Nitazoxanide
Nitazoxanide (Alinia) has broad-spectrum antiparasitic activity covering Giardia, Cryptosporidium, Blastocystis, and some helminth infections.
For biliary fascioliasis, it achieves approximately 60% cure rate in adults at 500mg twice daily for 7 days, making it a second-line option when triclabendazole is unavailable. R
It is also useful for Ascaris and can be a gentler first choice in patients with multiple sensitivities. R
Ivermectin
Ivermectin is the drug of choice for Strongyloides stercoralis (threadworm), which can invade the biliary tree and cause biliary strongyloidiasis, particularly in immunocompromised patients.
It is also first-line for onchocerciasis, lymphatic filariasis, and scabies.
Standard dosing for Strongyloides: 200mcg/kg once, repeated 2 weeks later for complete clearance. R
Hyperinfection syndrome from Strongyloides in immunosuppressed patients (steroid use, HTLV-1, malnutrition) can be life-threatening and requires immediate treatment with ivermectin.
Herbal Antiparasitics: Evidence And Application
Pharmaceutical antiparasitics are essential for confirmed biliary parasite infections.
Herbal antiparasitics occupy a different role: they are most appropriately used as broad-spectrum supportive agents when laboratory-confirmed parasitic species are not identified, as adjuncts to pharmaceutical treatment to address concurrent intestinal parasitic burden, and for maintenance and prevention in high-risk individuals.
The evidence base for herbal antiparasitics varies considerably by compound.
There is an important caveat: most human evidence for herbals is from in vitro studies or limited clinical trials, not the rigorous dose-response studies we have for pharmaceuticals. This must be stated plainly and not papered over.
With that context, here is what the evidence supports:
Artemisia (Wormwood)
Artemisia absinthium (common wormwood) contains sesquiterpene lactones, flavonoids, and phenolic acids with documented anthelmintic activity.
A 2018 study in Phytomedicine found that Artemisia absinthium extract demonstrated anthelmintic activity against Hymenolepis nana (dwarf tapeworm) comparable to praziquantel in a dose-dependent manner. R
Wormwood is also documented to have activity against Helicobacter pylori, various roundworm species, and Giardia.
A clinical trial found herbal antimicrobial blends including wormwood were as effective as rifaximin for SIBO eradication (46% vs 34% normalization), with fewer adverse effects. R
Artemisia annua (sweet wormwood) contains artemisinin, the compound responsible for the Nobel Prize-winning antimalarial discovery.
Artemisinin generates free radicals within parasitic cells via its endoperoxide bridge, destroying them.
Its antiparasitic action extends well beyond malaria to broad-spectrum protozoan organisms.
Key difference: Artemisia absinthium (bitter wormwood) for helminth infections; Artemisia annua (sweet wormwood, artemisinin) for protozoan/malaria-type organisms. They are different plants with different active compounds and different applications.
Caution: Wormwood contains thujone, a compound that can lower seizure threshold at high doses. Distilled extracts (absinthe) concentrate thujone significantly. Avoid in seizure disorders. Do not use for more than 4 weeks continuously without medical guidance.
Black Walnut Hull
Juglone is the primary antiparasitic compound in black walnut hull (Juglans nigra).
Juglone disrupts the outer surface of parasites and has documented in vitro activity against Giardia, Candida, and several helminth species. R
Tannins in black walnut hull precipitate proteins in parasite tissues, creating an astringent GI environment hostile to adult worms.
Black walnut hull is primarily active against adult worms, not eggs.
Caution: Black walnut hull is a common sensitizer and intolerance is frequent. CellCore Para 4 was specifically formulated for those who react to black walnut hull.
Cloves (Eugenol)
Eugenol from cloves (Syzygium aromaticum) is documented to kill parasite eggs, including those of Giardia, Blastocystis hominis, and Schistosoma species.
This is clinically important because most pharmaceutical antiparasitics and other herbal agents have minimal or no ovicidal activity.
Killing adult worms while leaving eggs intact results in reinfection within 2-4 weeks as eggs hatch and mature.
Cloves in combination with wormwood and black walnut hull address adults, larvae, and eggs simultaneously, which is the pharmacological rationale for the three-herb protocol. R
Eugenol also has broad antimicrobial activity including against Candida, H. pylori, and biofilm-forming organisms.
Oregano Oil (Carvacrol And Thymol)
Carvacrol and thymol from oregano oil (Origanum vulgare) are among the most well-researched botanical antiparasitics.
They disrupt parasite cell membranes and interfere with critical metabolic functions, with documented in vitro activity against Giardia, Blastocystis hominis, Cryptosporidium, and several helminth species. R
Caution: Oregano oil is potent and can cause significant GI irritation. Dilute, start low, and dose away from probiotics.
Berberine
Berberine (from goldenseal, barberry, Oregon grape, and Berberis vulgaris) intercalates into the DNA of parasitic organisms, disrupting transcription and replication. R
It has documented activity against Giardia lamblia, Entamoeba histolytica, Trichomonas vaginalis, and Leishmania species.
It was evaluated as a potential new pharmaceutical antiparasitic drug at one point and found to have genuine activity, though it was not developed further due to lack of commercial incentive.
Berberine also has significant antimicrobial activity against many pathogenic bacteria associated with biliary disease.
Mimosa pudica Seed
Mimosa pudica seed is primarily used for its mechanical action in the gut rather than direct antiparasitic pharmacology.
The seed is extremely gelatinous and becomes jelly-like and sticky in the intestinal tract.
This sticky mass physically binds to parasites, biofilm, mucus buildup, and intestinal debris, mechanically dislodging and capturing them for elimination. R
It is particularly valued in functional medicine for producing visible physical evidence of parasite clearance in stool.
It does not rely on pharmacological antiparasitic mechanisms and does not require drug-parasite matching, making it a useful foundational tool regardless of specific species.
Neem (Azadirachta indica)
Azadirachtin from neem interferes with cholinergic neurotransmission in parasitic worms, causing paralysis and facilitating their expulsion from the digestive tract. R
Neem also has documented antifungal, antibacterial, and anti-biofilm properties.
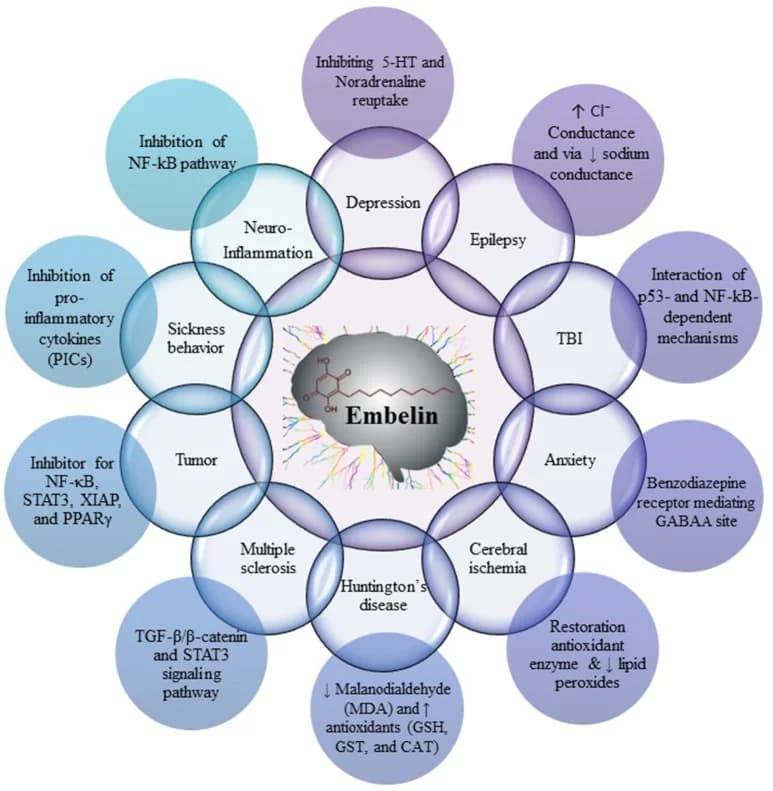
Vidanga (Embelia ribes) And Triphala
Vidanga is an Ayurvedic antiparasitic with documented activity against intestinal helminths including Ascaris.
Triphala (three-fruit combination: amalaki, bibhitaki, haritaki) supports GI motility, microbiome balance, and provides a supportive substrate for antiparasitic clearance rather than direct killing activity.
The CellCore Para Protocol
CellCore Biosciences offers a structured parasite and detox protocol that I use with clients dealing with complex chronic illness, high parasitic burden, or multiple sensitivities.
Their products require a practitioner code to purchase.
You can register as a patient using my code WrNETza8 at cellcore.com to access their full product line.
CellCore's approach is built on BioActive Carbon Technology, which uses extracts of humic and fulvic acid to enhance cellular delivery and tolerability of their herbal formulations.
The core rationale of their protocol is sequencing: open drainage pathways before adding antiparasitic compounds, to minimize die-off reactions and ensure that what is cleared can actually exit the body.
The Para Products
Para 1 is 100% pure Mimosa pudica seed.
The seed becomes gelatinous and sticky in the GI tract, physically scrubbing and capturing parasites, biofilm, and intestinal buildup.
It does not rely on pharmacological killing. It is mechanical.
This is why it often produces visible evidence of parasite clearance in stool that other approaches miss.
Dose: 2 capsules on waking and 2 at bedtime, away from food. Keep 1 hour away from binders.
Para 2 is an encapsulated multi-herb blend: vidanga, neem, triphala, clove, holarrhena (kutaja), and BioActive Carbon fulvic acid extracts.
It adds pharmacological antiparasitic activity to Para 1's mechanical action, covering helminths (vidanga), neuromuscular paralysis in worms (neem), ovicidal activity (clove), and amebic/protozoal organisms (holarrhena).
Dose: 1 capsule three times daily on an empty stomach.
Para 3 is a seven-herb liquid tincture: sage, tansy, thyme, epazote (wormseed), black walnut hull, holy basil, and clove bud.
It is the most potent product in the protocol and the one most relevant to biliary parasite burden.
Being a tincture, it absorbs rapidly and acts systemically beyond the gut lumen, reaching tissue-dwelling organisms including parasites in the biliary tree.
Para 3 is specifically formulated to address Strongyloides, liver flukes, Clostridium, and Blastocystis hominis, which is directly relevant to the biliary context of this post.
Dose: Start at 5-10 drops in water three times daily before meals. Increase gradually to 25 drops three times daily.
Cycle: 3 weeks on, 1 week off. Repeat as needed.
For sensitive patients, start at 1-3 drops and titrate over several weeks. Die-off from Para 3 can be significant.
Para 4 is an 11-herb blend (cordyceps, celery seed, holy basil, horse tail, noni root, sarsaparilla, and others) formulated without black walnut hull for those who react to it.
It provides immune support, detoxification support, and antiparasitic activity and is appropriate as a Para 3 substitution in highly reactive patients or those with known black walnut intolerance.
BioToxin Binder contains humic acid, fulvic acid, yucca root, and broccoli sprout extract.
Binders are not optional during antiparasitic treatment. Dead parasites release endotoxins, ammonia, and biotoxins that cause significant herxheimer-type reactions if they are reabsorbed.
Take BioToxin Binder at least 1 hour away from Para 1 and 2 hours away from other supplements.
The Comprehensive Protocol: 5 Phases Over 10 Months
For patients dealing with intense chronic illness and significant parasitic or toxic burden, CellCore offers a structured 10-month, 5-phase Comprehensive Protocol.
The sequencing is the point: each phase builds on the previous one, and starting with antiparasitic products before drainage is open is the most common mistake practitioners make.
Phase 1: Energy And Drainage (Month 1)
The goal is to establish functional drainage pathways and energy production before any significant die-off is triggered.
Products: Bowel Mover, Advanced TUDCA, BioToxin Binder, CT-Minerals, MitoATP, InQamma Control.
Advanced TUDCA supports liver and bile duct drainage, which is directly relevant to biliary parasite clearance: poor bile flow allows biotoxins and parasite debris to recirculate rather than exit.
Bowel Mover ensures intestinal motility is functional so cleared material actually leaves the body.
MitoATP supports mitochondrial energy, which is required to power detoxification processes.
BioToxin Binder captures whatever is mobilized in the gut.
Phase 2: Gut And Immune Support (Month 2)
Antiparasitic work begins in the gut.
Products carried forward: Advanced TUDCA, BioToxin Binder, CT-Minerals, MitoATP.
New additions: KL Support, Para 1, Para 2.
KL Support addresses kidney and liver drainage, ensuring both clearance organs are functioning before the parasitic load intensifies.
Para 1 (Mimosa pudica) begins mechanical gut scrubbing.
Para 2 adds the herbal antiparasitic layer for gut-resident organisms.
Phase 3: Whole Body Immune Support (Month 3)
The protocol moves from gut-focused to systemic.
Products carried forward: Advanced TUDCA, Para 1, CT-Minerals, MitoATP.
New additions: LymphActiv, ViRadChem Binder, Para 3, Fulvic Iodine.
Para 3 is introduced here because drainage is now established and the gut has been addressed. The systemic tincture can now work on tissue-dwelling organisms and biliary parasites specifically.
ViRadChem Binder is designed to travel beyond the gut, supporting systemic detox of viruses, radiation, and chemicals.
LymphActiv supports lymphatic drainage, which is critical for moving immune complexes and die-off debris.
Phase 4: Systemic Detox (Month 4-5)
The focus deepens to lingering everyday toxins and environmental contamination.
Products carried forward: Advanced TUDCA, ViRadChem Binder, CT-Minerals, Fulvic Iodine, MitoATP.
New addition: HM-ET Binder (addresses heavy metals and environmental toxins).
InQamma Control is reintroduced here for additional inflammatory support.
Phase 5: Deeper Immune Support (Months 4-10, runs concurrently with Phase 4)
The immune system cleanup phase addresses what has been hiding in joints, organs, and the nervous system.
Products: LymphActiv (4 bottles sequentially), IS-BORR, IS-BART, IS-BAB, IS-BOOST.
These are introduced one at a time, one bottle per month, targeting specific immune and microbial challenges.
Each IS product targets different organisms or immune pathways.
Starting dose for IS products is 1 dropperful twice daily, working toward 10 droppersful twice daily by end of the bottle.
The key principle across all phases: drainage before antiparasitic action, binding during antiparasitic action, and sequential layering so the body is never overwhelmed beyond what it can process and eliminate.
What To Stay Away From
- Raw or undercooked freshwater fish (primary transmission route for Clonorchis, Opisthorchis, and other biliary flukes; this includes ceviche, sushi, and traditionally prepared raw fish dishes from endemic regions)
- Raw watercress and aquatic vegetables from areas where livestock graze (Fasciola hepatica transmission route; cooking destroys metacercariae)
- Unwashed produce from areas with soil contamination (Ascaris and Toxocara transmission)
- Praziquantel for Fasciola infection (it will not work; the only evidence-based treatment is triclabendazole) R
- Die-off without binders (antiparasitic treatment without concurrent binder use allows endotoxins from dying parasites to be absorbed, causing severe herxheimer-type reactions including worsening fatigue, brain fog, headaches, and systemic inflammation)
- Aggressive antiparasitic treatment in the context of impaired liver function (both pharmaceuticals and herbal antiparasitics are hepatically cleared; albendazole is specifically contraindicated in cirrhosis; assess baseline liver function first) R
- Taking albendazole without fat (less than 5% is absorbed on an empty stomach; fat is required for meaningful tissue levels; a consistent fatty meal is not optional) R
- Wormwood in seizure disorders (thujone content can lower seizure threshold)
- Cloves and black walnut on blood thinners without practitioner monitoring (both have anticoagulant properties that can add to warfarin and other anticoagulants)
- Treating biliary Ascaris with herbs alone (impacted Ascaris in the common bile duct requires endoscopic extraction; herbal agents cannot dislodge a mechanically obstructing worm)
Testing
Stool Testing
Microscopic examination of stool for ova and parasites (O&P) is the primary first-line test for biliary and intestinal parasites, but has significant sensitivity limitations for fluke infections.
Multiple stool samples (three samples on different days) are recommended because fluke egg shedding is intermittent. R
PCR-based stool testing is significantly more sensitive than microscopy for most GI parasites including Giardia, Cryptosporidium, Entamoeba histolytica, Ascaris, hookworm, and others.
The Gut Zoomer from Vibrant Wellness includes comprehensive parasite detection via multiplex PCR alongside microbiome analysis and intestinal permeability markers.
Serology (Blood Antibody Tests)
For liver flukes and Fasciola, stool may be negative during the hepatic migration phase because the worms have not yet reached the bile ducts and are not producing eggs.
Fasciola serology (IgG ELISA) is the most sensitive test during the acute hepatic phase and becomes positive within 2-4 weeks of infection. Available through specialty reference labs.
Clonorchis/Opisthorchis serology is available but less widely used; stool PCR or ERCP bile analysis is more commonly employed. R
Ascaris serology exists but is rarely needed since microscopy and PCR are highly sensitive for this large-egg-producing species.
Blood Markers
Complete blood count (CBC) with differential: look for persistent eosinophilia (eosinophils greater than 500 cells/mcL). This is the single most important blood marker suggesting helminth infection. R
Liver function panel (AST, ALT, GGT, ALP, bilirubin): elevated in active biliary inflammation from flukes. GGT and ALP elevation suggests cholestatic/biliary involvement.
IgE (total): elevated in helminth infections, reflecting the Th2 immune response. Included in the Immune Zoomer.
Imaging
Right upper quadrant ultrasound is the first-line imaging study and can detect bile duct dilatation, worm shadows in the bile duct or gallbladder, gallbladder wall thickening, and pericholecystic fluid.
MRCP (Magnetic Resonance Cholangiopancreatography) is non-invasive and the most sensitive imaging modality for visualizing flukes in the bile ducts as filling defects or mobile lesions.
ERCP (Endoscopic Retrograde Cholangiopancreatography) is both diagnostic and therapeutic: it allows direct visualization, biliary aspirate collection for microscopy, and endoscopic extraction of worms when indicated.
Functional And Toxicology Testing
The Foundation Zoomer provides baseline liver function markers (AST, ALT, GGT, ALP, bilirubin, CBC, CMP) to assess hepatic function before, during, and after antiparasitic treatment.
The Toxin Zoomer combined with the Immune Zoomer is appropriate when biliary parasitism is suspected alongside CIRS or mycotoxin illness.
Mechanisms Of Action
Simple:
- Biliary flukes enter through the mouth via infected food, travel to the intestine, migrate up through the bile duct, and take up permanent residence in the bile ducts where they live for decades.
- The flukes damage bile duct epithelium with their feeding structures, generating chronic inflammation and progressive fibrosis.
- Damaged bile ducts cannot secrete bile acid properly, creating a bile composition that favors gallstone nucleation.
- Dead worm fragments and eggs serve as crystallization seeds for calcium bilirubinate pigment stones.
- Bacteria that infect the damaged bile ducts produce beta-glucuronidase, deconjugating bilirubin and generating more free bilirubin to form more stones.
- Long enough, this chronic inflammatory cycle can drive malignant transformation of bile duct epithelium into cholangiocarcinoma.
Advanced:
- Fluke excretory-secretory (ES) products and carcinogenesis: Clonorchis and Opisthorchis ES products include glutathione S-transferase, phosphoglycerate kinase, and granulin-like growth factors. Fluke granulin is a potent proliferative signaling molecule that promotes cholangiocyte proliferation and survival, directly driving the hyperplastic-metaplastic-dysplastic progression. ES product-induced NF-kB activation sustains the inflammatory microenvironment needed for malignant transformation. R
- Praziquantel mechanism: At therapeutic concentrations, praziquantel causes rapid influx of calcium ions into helminth muscle cells via altered membrane permeability. The resulting sustained muscular contraction (spastic paralysis) is followed by tegumental disruption, exposing the parasite surface antigens to immune attack. The host immune response (eosinophils, complement) completes the killing. The tegumental disruption is why praziquantel fails against Fasciola: Fasciola tegument has a different composition and is less susceptible to praziquantel-mediated disruption. R
- Triclabendazole mechanism vs. other benzimidazoles: Triclabendazole and albendazole both target tubulin, but triclabendazole binds more specifically to Fasciola beta-tubulin with higher affinity than to mammalian tubulin. Critically, triclabendazole is active against immature newly excysted juveniles as well as adult flukes, which is mechanistically why it works where albendazole does not for acute fascioliasis (albendazole lacks efficacy against immature stages). R
- Mimosa pudica seed mucosal binding: The seed powder expands to a mucilaginous, high-viscosity hydrogel in the intestinal lumen. The hydrogel physically adheres to the intestinal wall through electrostatic interactions. It traps parasites, heavy metals, and biofilm in the gel matrix and prevents their reabsorption or reattachment to the mucosa. Unlike activated charcoal, Mimosa pudica does not significantly adsorb nutrients, making it usable long-term. R
- Juglone mechanism: Juglone (5-hydroxy-1,4-naphthoquinone) generates reactive oxygen species (ROS) within parasite mitochondria via redox cycling, overwhelming the parasite's antioxidant defenses. It also inhibits succinate dehydrogenase and other mitochondrial enzymes critical to helminth energy metabolism. The parasite, lacking the adaptive ROS defenses of mammalian cells, cannot compensate and dies. R
- Eugenol ovicidal mechanism: Eugenol from cloves disrupts the lipid components of the egg capsule (vitelline membrane), altering membrane permeability and preventing normal embryonic development. It also chelates metal ions required for enzymatic activity in developing larvae. These two mechanisms explain its selective activity against eggs and early larvae that other agents miss. R
- Berberine DNA intercalation: Berberine is a planar quaternary ammonium alkaloid that inserts between base pairs in parasitic DNA (intercalation). This physically distorts the double helix, blocking DNA topoisomerase activity, impairing DNA replication, and triggering parasitic cell death. The selectivity over mammalian cells reflects differences in uptake mechanisms and the sensitivity of the specific topoisomerase isoforms. R
Genetics
HLA-DR/DQ (Parasite Clearance And CIRS Susceptibility)
Specific HLA class II haplotypes (particularly HLA-DR4, DQ8, and related biotoxin-susceptibility haplotypes identified by Shoemaker) impair the ability to produce antibodies against biotoxins including parasite-derived toxins.
Individuals with these haplotypes are more likely to develop persistent symptomatology from parasitic infections and may not mount adequate eosinophilic immune responses to clear helminths effectively.
This is the genetic underpinning of why some individuals become chronically symptomatic from parasitic exposures that others clear asymptomatically.
IL-10 And IL-13 (Th2 Immune Regulation)
Helminth infections drive a strong Th2 immune response: IL-4, IL-5, IL-13, and IgE are the characteristic cytokines of anti-parasitic immunity.
IL-5 drives eosinophilia. IL-13 drives mast cell activation and smooth muscle contraction (facilitating worm expulsion).
Polymorphisms in IL-13 and IL-10 regulatory genes affect the magnitude of the Th2 response, influencing parasite clearance efficiency and risk of allergic sensitization following helminthic infection.
Individuals with attenuated Th2 responses have greater difficulty clearing helminths.
ABCB1 (P-glycoprotein) And Antiparasitic Drug Efflux
ABCB1 (P-glycoprotein / MDR1) is an efflux transporter expressed in the intestinal epithelium and blood-brain barrier that pumps drugs out of cells.
Albendazole sulfoxide (the active metabolite of albendazole) is a substrate of P-glycoprotein.
Gain-of-function variants in ABCB1 can increase efflux of albendazole sulfoxide from intestinal epithelium, reducing drug tissue exposure and potentially contributing to treatment failure.
rs1128503 and rs2032582 (ABCB1 C3435T and G2677T/A) are the most commonly studied functional variants affecting P-glycoprotein activity and drug bioavailability.
This is clinically relevant for patients who fail standard albendazole courses without other explanation.
GSTM1 And GSTT1 (Detox Of Parasite Toxins)
As covered in the mycotoxin post, null polymorphisms in GSTM1 and GSTT1 reduce Phase II glutathione conjugation capacity.
This affects clearance of the reactive metabolites generated both by parasite excretory-secretory products and by benzimidazole antiparasitics.
GSTM1/GSTT1 null individuals may experience greater toxicity from both the parasites and the treatment.
More Research
- Biliary parasitic infections are increasingly encountered in non-endemic Western countries due to travel, immigration, and global food trade; a high index of suspicion should be maintained in anyone with eosinophilia and upper right quadrant symptoms, regardless of geographic history. R
- Clonorchis sinensis and Opisthorchis viverrini are classified as Group 1 biological carcinogens by IARC on the basis of their well-established progression to cholangiocarcinoma through chronic biliary inflammation and cholangiocyte DNA damage. R
- Die-off reactions (Jarisch-Herxheimer-like responses) during antiparasitic treatment are primarily driven by endotoxin release from dying parasites and secondarily from disruption of co-infecting gut bacteria; binders during treatment are not optional but essential for minimizing this response.
- Fasciola hepatica resistance to praziquantel is well-documented; using praziquantel for fascioliasis is a common clinical error that delays effective treatment with triclabendazole. R
- For comprehensive GI parasite testing I use the Gut Zoomer (Vibrant Wellness) when I want simultaneous microbiome, permeability, and parasite data.
- Herbal antimicrobial blends including wormwood outperformed rifaximin in SIBO eradication in a clinical trial (46% vs 34% normalization), with significantly fewer adverse effects, suggesting a meaningful role for botanical antimicrobials in GI infectious conditions even where pharmaceutical data is limited. R
- Most biliary abnormalities from Opisthorchis infection, including bile duct dilatation and wall thickening, can reverse after successful praziquantel treatment, arguing for early detection and treatment before irreversible fibrotic changes develop. R
- O&P (ova and parasite) stool microscopy has poor sensitivity for liver fluke infections in particular; negative microscopy does not rule out biliary parasitism and should not be used as the sole exclusionary criterion when clinical suspicion is present. R
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Spore-Based Probiotics
1 cap with food
L-Glutamine
5g 2x/day on empty stomach
Butyrate
300mg 2x/day with meals